Clinical and epidemiological profile of pregnant and postpartum women affected by COVID-19 who required respiratory support
Carolina Maria Pires Cunha, Melania Maria Ramos Amorim, Julianna de Azevedo Guendler, Alex Sandro Rolland Souza, Leila Katz

TL;DR
This study examines the clinical and demographic characteristics of pregnant and postpartum women with severe COVID-19 requiring respiratory support in Brazil.
Contribution
The study provides a detailed profile of pregnant/postpartum women with severe COVID-19 requiring respiratory support in Brazil.
Findings
Most patients were brown-skinned, in the third trimester, and referred from another hospital.
High rates of cesarean sections, maternal near miss, and death were observed.
Non-invasive ventilation was most commonly used, with a significant proportion needing invasive mechanical ventilation.
Abstract
This study described the clinical and epidemiological profile and the management provided to pregnant and postpartum women with COVID-19 who required respiratory support. A descriptive study was conducted with pregnant and postpartum women with confirmed COVID-19 who received care between April 2020 and December 2021 in eight referral centers in northeastern Brazil. Statistical analysis was conducted using Epi-Info 7.2.5 and Medcalc, version 20.112. Of the 720 patients admitted, 208 (32.7%) required respiratory support. Mean age of the participants was 28.9±7.1 years. Most (52.8%) were brown-skinned; 31.3% had little formal schooling; 41.1% had a personal income and 23.1% were married. Around half were referred from another hospital. Overall, 36.8% were obese and 36.9% were hypertensive. Criteria for severe acute respiratory syndrome (SARS) were present in 80.7% of cases. Overall, 151…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
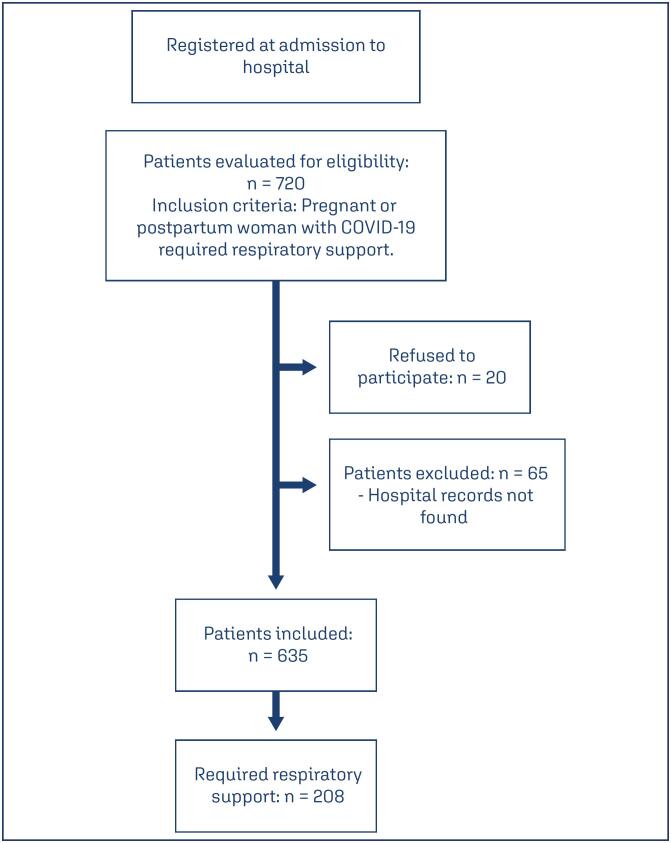 Figure 1
Figure 1| Characteristics | ||
|---|---|---|
| Age (years) (mean/standard deviation) | 28.9(7.1) | |
| Ethnicity/skin color (n / %) | ||
| White | 28(13.5) | |
| Brown | 110(52.8) | |
| Black | 11(5.3) | |
| Indigenous | 1(0.5) | |
| Of Asian descent | 1(0.5) | |
| Unknown | 57(27.4) | |
| Poor education | 35(31.3) | |
| Income of her own | 39(41.1) | |
| Marital status (n / %) | ||
| Married | 48(23.1) | |
| In a stable union | 35(16.8) | |
| Divorced/separated | 3(1.4) | |
| Widowed | 1(0.5) | |
| Single | 44(21.2) | |
| Unknown | 77(37.0) | |
| Origin of patient (n / %) | ||
| Came straight from home | 44(21.2) | |
| Referred from a primary healthcare unit | 15(7.2) | |
| Referred from another hospital | 106(50.9) | |
| Unknown | 43(20.7) | |
| Pregnancies | ||
| Median/interquartile range | 3(2-4) | |
| Range | 1-9 | |
| Parity | ||
| Median/interquartile range | 1(1-3) | |
| Range | 0-8 | |
| Obesity or overweight described on hospital records | 46(36.8) | |
| Hypertensive syndromes | 69(36.9) | |
| Number of prenatal visits | ||
| Median/interquartile range | 5(3-6) | |
| Range | 0-9 | |
| Gestational age at admission (of the women admitted to hospital while pregnant) (in weeks) | ||
| Median/interquartile range | 32.5(29-35.5) | |
| ≤ 22 weeks (n / %) | 16(8.8) | |
| 23-28 weeks (n / %) | 28(15.4) | |
| 29-34 weeks (n / %) | 60(33.0) | |
| 35-36 weeks (n / %) | 47(25.8) | |
| ≥ 37 weeks (n / %) | 31(17.0) | |
| Admitted postpartum (n / %) | 26(12.5) | |
| At hospital admission | Worst value during hospitalization | |||
|---|---|---|---|---|
| Respiratory rate (breaths/minute) (median / interquartile range) | 28 | 22-32 | 34 | 28-40 |
| Respiratory rate >25 breaths/minute (n / %) | 111 | 60 | 160 | 85,5 |
| SpO2 levels (%) (median /interquartile range) | 96 | 93-98 | 91 | 88-94 |
| SpO2levels <95% (n / %) | 66 | 34.4 | 149 | 76.8 |
| Characteristics | n(%) | |
|---|---|---|
| Dry cough | 132(63.5) | |
| Fever | 137(65.8) | |
| Headache | 168(80.7) | |
| Dyspnea | 164(78.8) | |
| Chest pain | 28(13.5) | |
| Criteria for SARS | 168(80.7) | |
| Abnormalities at chest x-ray | 70(80.5) | |
| Diffuse pulmonary infiltrate | 36(51.4) | |
| Abnormalities on computed tomography of the chest | 32(69.6) | |
| Ground-glass opacity | 30(93.7) | |
| Corticoid therapy | 151(74.7) | |
| Antibiotic treatment | 171(82.2) | |
| Neuromuscular blocking agents | 34(16.3) | |
| Admission to maternal ICU | 150(76.1) | |
| Mode of delivery | ||
| Vaginal | 13(8.4) | |
| Cesarean section | 142(91.6) | |
| 1-minute Apgar score (median /interquartile range) | 8(7-9) | |
| 5-minute Apgar score (median /interquartile range) | 8(5-9) | |
| Neonatal near miss***** | 17(14.2) | |
| Neonatal death***** | 7(4.5) | |
| Maternal near miss | 50(24.0) | |
| Maternal death | 27(12.9) | |
| Total | 208(100) | |
| Characteristic | n(%) | |
|---|---|---|
| Non-invasive ventilatory support | 186(89.4) | |
| Nasal catheter | 115(55.3) | |
| Venturi mask | 9(4.3) | |
| Non-rebreather mask | 26(16.8) | |
| Continuous positive airway pressure (CPAP) | 7(3.4) | |
| Mechanical ventilation | 78(37.5) | |
| Extracorporeal membrane oxygenation (ECMO) | 1(0.5) | |
| Assisted mechanical ventilation in prone position | 10(4.8) | |
| Spontaneous ventilation in prone position | 17(8.2) | |
| Total | 208(100) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Impact on Reproduction · Maternal Mental Health During Pregnancy and Postpartum · Pregnancy and Medication Impact
Introduction
Pregnancy leaves women more vulnerable to viral diseases such as Coronavirus Disease 2019 (COVID-19) due to physiological factors, abnormal respiratory mechanics and increased oxygen consumption, hypercoagulability and changes in the immune system.^(1)^
The COVID-19-related maternal complications and mortality have been the focus of several studies worldwide. An increased incidence of the severe forms of COVID-19 has been shown during pregnancy and in the postpartum and an association has been found between COVID-19 and adverse gestational and perinatal outcomes.^(2,3)^ In Brazil, a country where maternal mortality is habitually high, the number of deaths during pregnancy and in the postpartum has increased since the beginning of the COVID-19 pandemic.^(4)^
Although pregnant women with COVID-19 are less likely to show symptoms, they are more likely to require hospitalization, to be admitted to an Intensive Care Unit (ICU) and to require invasive ventilation, and they are at a greater risk of severe acute respiratory syndrome (SARS) compared to non-pregnant women of reproductive age.^(5)^ An increased risk of death from the disease has also been documented.^(4)^
Some studies have reported a greater risk of SARS in pregnant and postpartum women.^(6,7)^ Nevertheless, more robust data on pregnant women with COVID-19-related SARS admitted to ICU are not yet available for this particular setting. Therefore, it is important to characterize this population as well as the course of the disease, its management and outcomes, adding data to what is already known and contributing substantially to improving maternal and child healthcare.
Consequently, the objective of the present study was to describe the clinical and epidemiological profile, management and neonatal prognosis of pregnant women with COVID-19 requiring respiratory support and receiving care at referral centers in northeastern Brazil.
Methods
This was a descriptive study that included pregnant and postpartum women with COVID-19 who required respiratory support. The study was conducted between April and December 2021. It is an offshoot of a multicenter study, initiated in 2020 and registered at Clinical Trials under reference NCT04462367, which was conducted to describe the clinical, epidemiological and laboratory characteristics of cases of COVID-19-related maternal near miss and death in northeastern Brazil. Data were collected at six referral centers in northeastern Brazil: two in the state of Pernambuco, four in Paraíba and one in Ceará. The study involved both retrospective and prospective stages. Sample size was not calculated because all the patients who received care at the referral hospitals in the first two years of the pandemic who met the eligibility criteria were included in the study. A non-probabilistic, consecutive convenience sample was obtained. Patients whose hospital records could not be located or were incomplete were excluded from the current analysis.
The variables analyzed were: patients’ biological and sociodemographic characteristics (maternal age, skin color/ethnicity, education, maternal occupation including income, marital status and origin of the patient prior to admission); obstetric characteristics (whether pregnant or postpartum at inclusion in the study, number of pregnancies, parity, number of prenatal visits, gestational age at admission and mode of delivery), characteristics of respiratory rate and oxygen saturation; comorbidities/complications associated with pregnancy/postpartum (SARS, hypertensive syndromes, obesity/overweight and asthma), COVID-19-related symptoms (cough, fever, headache, dyspnea and chest pain) and radiologic findings (chest x-ray and tomography) and forms of treatment administered during hospitalization (admission to ICU, treatment with corticoids, antibiotics, neuromuscular blocking agents, assisted mechanical ventilation and non-invasive ventilation). Finally, maternal outcome (maternal near miss and death) and neonatal outcome (1-minute and 5-minute Apgar scores) were evaluated.
COVID-19 was confirmed by positive real-time polymerase chain reaction. SARS was defined as a flu-like syndrome (fever, cough, dyspnea and other non-specific symptoms) together with oxygen saturation (SpO_2_) <95%, respiratory distress or tachypnea, hypotension and worsening clinical conditions of the primary disease.^(8)^ Need for mechanical ventilation was defined as having used one of the following modes of treatment: non-invasive ventilation (nasal catheter, Venturi mask, non-rebreather mask, continuous positive airway pressure [CPAP]); mechanical ventilation; extracorporeal membrane oxygenation [ECMO]; assisted mechanical ventilation in prone position and spontaneous ventilation in prone position.
According to the definition of the World Health Organization (WHO), maternal near miss (MNM) refers to a woman who nearly died but survived a complication that occurred during pregnancy, childbirth or within 42 days of termination of pregnancy.^(9)^ Maternal death is defined as the death of a woman while pregnant or within 42 days of termination of pregnancy from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.^(9)^ Neonatal near miss refers to a newborn infant with a severe complication at birth (five-minute Apgar <7; birthweight <1,750 grams or gestational age <33 weeks) or who requires certain management (parenteral antibiotics, nasal CPAP or intubation up to 7 days and before the 28^th^ day of life, phototherapy within 24 hours of life, cardiopulmonary resuscitation, use of vasoactive drugs, use of anticonvulsants, use of blood derivatives, use of corticoid therapy to treat refractory hypoglycemia and surgery) but who survives up to the 27^th^ day of life.^(10)^ Neonatal death was defined as death occurring within the first 27 days of life.^(11)^
The statistical analysis was performed using the Epi Info software program, version 7.2.5 and Medcalc, version 20.112. Measures of central tendency and dispersion were used to describe the numerical variables, while frequency distribution tables were constructed for the categorical variables.
The institutional review board approved the study protocol under reference CAAE 58466822.0.0000.5201. Since the research consisted of analyzing a secondary database previously created for the original study, the need for informed consent was waived.
Results
During the period of the original study, 720 patients were admitted to hospital. Of these, 20 refused to participate. In addition, 65 were excluded from the current analysis because their records could not be located. Of the 635 remaining patients, 208 (32.7%) required some form of respiratory support and constituted the present sample (Figure 1).
Patient admission process
The mean age of the participants was 28.9 ± 7.1 years. Most (52.8%) were brown-skinned, while 13.5% were white and 5.3% were black; however, in 27.4% of cases this information was missing from the records. In relation to their sociodemographic characteristics, 35 patients (31.3%) had little schooling and 39 (41.1%) had a personal income. Overall, 48 (23.1%) were married and 44 (21.2%) were single; however, in 77 cases (37%) information on marital status was missing from the charts. Most of the women (50.9%) were referred to this hospital from another healthcare institute, while 21.2% came straight from home (Table 1).
Patients had had from 1 to 9 pregnancies, with a median of 3 (interquartile range [IQR] 2-4) and the number of births ranged from 0 to 8, with a median of 1 (IQR 1-3). The number of prenatal visits attended ranged from 0 to 9, with a median of 5 (IQR 3-6), while the median gestational age at admission was 32.5 weeks (IQR 29 - 35.5 weeks). When gestational age was stratified by week intervals, 60 patients (33%) were at 29-34 weeks of pregnancy, 47 (25.8%) were at 35-36 weeks and 31 patients (17%) were over 37 weeks pregnant. In 26 cases (12.5%), the patient was admitted to hospital during the postpartum period (Table 1).
At admission, 46 women (36.8%) were obese or overweight and 69 (36.9%) had hypertensive syndromes. Furthermore, 13.4% of the women had gestational diabetes and 6% had pre-gestational diabetes mellitus (Table 1).
Median respiratory rate at admission was 28 breaths/minute (IQR 22-32), with the worst median value during hospitalization being 34 breaths/minute (IQR 28-40). Median SpO_2_ at admission was 96% (IQR 93-98), with the worst median during hospital stay being 91% (IQR 88-94) (Table 2).
The principal signs and symptoms in the patients were: headache (80.7%), dyspnea (78.8%), fever (65.8%) and dry cough (63.5%). The criteria for SARS were present in 168 patients (80.7%). While most patients were not submitted to imaging tests, abnormalities were found in 70/87 patients (80.5%) submitted to chest x-ray and in 32/46 (69.6%) patients who had a tomography. The most common abnormality found at x-ray was diffuse pulmonary infiltrate, present in 51.4% of the women evaluated, while the most common abnormality found at tomography was ground-glass opacity, found in 93.7% of patients evaluated (Table 3).
A total of 151 patients (74.7%) were treated with corticoids for COVID-19, while 171 (82.2%) used antibiotics, 34 (16.3%) neuromuscular blocking agents and 150 (76.1%) were admitted to the ICU. There were 50 cases (24%) of maternal near miss and 27 (12.9%) women died (Table 3). Information on the mode of delivery was available for 155 patients, with 142 patients (91.6%) having undergone a cesarean section and 13 (8.4%) having had a vaginal delivery. In relation to the neonatal endpoints, the median 1-minute Apgar score was 8 (IQR 7-9) and the median 5-minute Apgar score was 8 (IQR 5-9). Adverse neonatal outcomes included 17 cases (14.2%) of neonatal near miss and 7 neonatal deaths (4.5%) (Table 3).
A total of 208 women required some type of ventilation strategy or respiratory support during hospitalization. Non-invasive ventilation was used in 186 cases (89.4%), with 115 using a nasal catheter, 26 (16.8%) a non-rebreather mask, 9 (4.3%) a Venturi mask and 7 (3.4%) CPAP. Invasive mechanical ventilation was the resource used in 78 cases (37.5%), with 1 patient using ECMO, 17 (8.2%) using spontaneous ventilation in the prone position and 10 (4.8%) assisted mechanical ventilation in the prone position (Table 4).
Discussion
Although the acute phase of the COVID-19 pandemic has passed, its consequences on maternal and neonatal health remain a crucial field of study. Pregnant women are a vulnerable population, and our research provides valuable data on how COVID-19, specifically Severe Acute Respiratory Syndrome, affected this population in the Northeast of Brazil. The hospital records of 635 pregnant or postpartum women were analyzed and, of these, 208 were found to have required respiratory support. The sociodemographic characteristics of these patients show that most were brown-skinned, married and had been referred from other hospitals. The most common comorbidities present were obesity, diabetes and hypertensive syndromes.
The mean age of the patients who required ventilatory support in the present study was lower than that reported in a prospective, multicenter study involving pregnant women who had tested positive for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). In that study, published in April 2020 by the German Society of Perinatal Medicine, the median age of the pregnant women who required intensive care was 33 years.^(12,13)^ An epidemiological bulletin published in Brazil showed that, of the cases of SARS in pregnant women who required ventilatory support, the age group with the most number of notified cases of COVID-19 was the 20-29-year age group,^(14)^ as reported in the present study.
Most of the women in the present study self-reported as being brown-skinned, followed by white and then black women. This finding is in agreement with a survey of data from the Brazilian nationwide surveillance database on seasonal influenza, which described pregnant women of 10 to 49 years of age hospitalized due to SARS-CoV-2 between January and November 2020, in which almost half the sample self-reported as being brown-skinned.^(15)^ The inequalities associated with race/ethnicity are well known in Brazil. Evidence of this disproportional impact is also apparent in ethnic groups that have been historically oppressed in the country, the current epicenter of the global pandemic.^(16)^ In Brazil, the intersection of gender, race and social class compounds the tragedy of the maternal deaths resulting from COVID-19, particularly when the country fails to adopt measures that would truly contain pandemics.^(15)^ On the other hand, the large amount of missing data on skin color/race may in itself be a reflection of the structural racism in Brazilian society that permeates healthcare facilities.^(17)^
A significant proportion of the sample had little schooling. Socioeconomic status and poor education can accelerate worsening maternal health, since these factors affect the quality of prenatal care and the effectiveness of treatment, hence being associated with maternal morbidity and mortality.^(17)^ Furthermore, there are chronic problems associated with women's healthcare in Brazil, including insufficient resources, poor quality prenatal care, fewer hospital beds than are required, difficult access to healthcare facilities, racial disparities and obstetric violence.^(4)^
Most of the patients in the present study had been referred from another hospital, with the majority of the others coming straight from home. The possible explanation for the high rate of referral from other hospitals is that the data were extracted from referral centers for northeastern Brazil; therefore, many of the patients who were in a critical state had been transferred from other healthcare facilities. We failed to find data referring to other similar samples, thus making comparison with other databases impossible.
The presence of comorbidities increases the risk of developing more severe respiratory distress and introduces a greater likelihood of requiring hospitalization, of developing complications and of death.^18^ Part of the sample was described in the hospital records at admission as being obese or overweight. A study conducted in Brazil using data from the Brazilian nationwide surveillance database on seasonal influenza described 6,073 pregnant women with COVID-19 between 2020 and 2021 and highlighted obesity as one of the most common comorbidities in that population.^(18)^ Some parameters could explain the greater frequency of respiratory complications in obese patients, including: reduced functional residual capacity and expiratory residual volume, as well as hypoxia and ventilation/perfusion abnormalities.
Hypertensive syndromes and gestational diabetes were also very common in the present study. The number of cases reported here is higher than numbers from a systematic review that analyzed 441 pregnant women with COVID-19 in 16 countries and identified the presence of hypertensive diseases (9%) and diabetes (11%) as being among the most common comorbidities.^(19)^
We believe that the high rate of pregnant women with chronic systemic arterial hypertension and also preeclampsia is due to the peculiarities of the hospitals included in the study. All are tertiary hospitals that, during the pandemic, acted as referral services for high-risk pregnancy. Since all pregnant women were tested for COVID-19 at admission, consequently the number of positive tests in women with such comorbidities was higher. On the other hand, the association between COVID-19 and preeclampsia has already been shown numerous times in other studies, with prognosis in such cases being poorer.^(19,20)^ Our research group is also investigating this association; however, it was not one of the objectives of the present study.
Median gestational age was 32.5 weeks. Due to the increase in the size of the uterus in the third trimester of pregnancy, the movement of the diaphragm is restricted, reducing total lung capacity. A study conducted in Brazil found a higher frequency of COVID-19-related SARS in women in the third trimester of pregnancy,^(7)^ corroborating data published by the Ministry of Health in 2021^(21)^ and the present results.
The number of prenatal visits ranged from 0 to 9, with a median of 5. One of the reasons for this insufficient number of prenatal visits could be the fact that the women began prenatal care late, reflecting difficulties in obtaining confirmation of pregnancy. This clearly highlights the need to improve women's access to diagnostic tools and the need to direct them towards prenatal care at an earlier stage.^(22)^ On the other hand, it is possible that the percentage of patients admitted at a lower gestational age could explain the lower median number of visits. Furthermore, information on prenatal visits was missing from a proportion of the sample, hampering analysis.
Although COVID-19 may affect several different organs and systems, SARS-CoV-2 is particularly aggressive to the respiratory system, leading to a wide array of symptoms ranging from a common cold to severe respiratory distress.^(23)^ Median respiratory rate at admission was 28 breaths/minute, with the worst median value during hospital stay being 34 breaths/minute. Median SpO_2_ at admission was 96%, with the poorest median value during hospitalization being 91%. The increased inflammation and reduced innate immune response may provide answers regarding the increased susceptibility to severe SARS-CoV-2 disease in patients with these conditions, including pregnant women.^(24)^ An exploratory cohort study conducted in Brazil on COVID-19 in pregnancy identified the risk factors leading to a need for oxygen in pregnant and postpartum women with COVID-19. The study revealed a greater risk of requiring oxygen therapy in patients with a respiratory rate of 24 breaths/minute and SpO_2_ <95%, data similar to those found in the present study.^(25)^
The principal signs and symptoms found in this group of pregnant women were: headache, dyspnea, fever and dry cough. Similar data were reported from a series of cases investigated in Iran.^(26)^
Although imaging tests were only performed in part of the sample, results showed a high frequency of abnormalities. A systematic review involving 1,316 pregnant women with confirmed COVID-19 reported the most common findings at computed tomography as ground-glass opacity followed by bilateral pneumonia, with prevalence rates of 65.8% and 57.9%, respectively.^(27)^ The frequency of findings at tomography in the present sample is higher than that reported in the systematic review, which could be explained by the fact that the present study included a subpopulation of more severely ill patients among those with the disease, defined as such by the fact that they required ventilatory support. Furthermore, at the specific healthcare units involved in this study, imaging tests are not routinely requested but are restricted to the most complicated cases, which may have resulted in a selection of patients in whom abnormalities at x-ray and tomography were more likely to be found.
In the present study, 74.7% of the pregnant women were given corticoids for the treatment of COVID-19. According to the Ministry of Health guidelines, corticoids should be considered seven days after the onset of symptoms if the patient still has significant lung involvement.^(28)^
In the present study, the mode of delivery was recorded for 155 cases, with most having undergone cesarean section. This finding raises the question of what is taken into account when indicating the mode of delivery, since high rates of cesarean section have also been reported in several other studies, including a systematic review involving 385 cases of COVID-19 in pregnancy. In that review, 252 births were reported, with 175 cesarean sections (69.4%) and 77 vaginal deliveries (30.6%).^(29)^ Since the present study is restricted to describing the fraction of patients who required ventilatory support, the limited number of vaginal deliveries can probably be explained by the clinical severity of the patients evaluated here.
Analysis of severe maternal outcomes showed that 24% of the women experienced maternal near miss and 12.9% died. In this respect, a study conducted in the city of New York in the United States reported a maternal mortality rate of 15% and a mean duration of ICU stay due to COVID-19 of 8 days.^(30)^ Another study conducted in Brazil investigated the characteristics and outcome of pregnant women with a SARS-CoV-2 infection and other severe acute respiratory infections (SARI) in Brazil. Mortality among these pregnant women with COVID-19 was high compared to that of other groups with SARI.^(7)^
In relation to the neonatal outcomes, the median 1-minute and 5-minute Apgar scores were 8. This finding is similar to data from one of the first retrospective analyses conducted in China in 2020 involving 9 liveborn infants, with a 1-minute Apgar score of 8-9 and a 5-minute Apgar score of 9-10.^(31)^ In relation to the more severe outcomes, neonatal near miss was recorded in 22 cases and there were 7 neonatal deaths. A systematic review evaluated data on studies from ten countries and showed that, of the 256 newborn infants analyzed, the outcomes reported included admission to an ICU in 8 cases (3.1%), neonatal mechanical ventilation in 3 (1.2%), newborn respiratory distress syndrome in 12 (4.7%), neonatal pneumonia in 3 (1.2%) and disseminated intravascular coagulation in 3 (1.2%). Three infants died.^(32)^
The principles of managing COVID-19 during pregnancy include early isolation, infection control procedures, oxygen therapy, prevention of fluid overload, empirical control with antibiotics (secondary to the risk of bacterial infection), monitoring for uterine contractions, early mechanical ventilation in cases of progressive respiratory failure, an individualized birth plan, and clinical care from a multidisciplinary team.^(33)^ In the present study, non-invasive ventilatory support was the principal resource used, with the most common method being a nasal catheter in slightly over half the patients, followed by a non-rebreather mask.
The objective of ventilatory support is to maintain the levels of maternal partial pressure of oxygen in arterial blood (PaO_2_) at 65-70 mmHg or higher to guarantee adequate fetal oxygen supply. This is contrary to the management for non-pregnant women in whom low levels of PaO_2_ are acceptable.^(34)^ A systematic review evaluated the effects of coronavirus on pregnant women and found that around 78.8% were treated with oxygen therapy, while 18.1% required mechanical ventilation.^(27)^
A considerable number of the patients in the present study were admitted to the maternal ICU and mechanical ventilation was used as a resource in 37.5% of these cases. This finding emphasizes the high numbers in Brazil compared to other countries such as the United States.^(22)^ A cohort study conducted in the United States compared the clinical characteristics and outcomes of hospitalized women with and without COVID-19. The rate of American women with COVID-19 who required intensive care was 3.3%, whereas only 1.3% of patients in that study required mechanical ventilation.^(22)^
Compared to other epidemics of flu-like syndromes, the rate of admission to an ICU for women with COVID-19 (19.5% of cases) was higher than that for SARI of unknown etiology (16.8%) or for influenza (15.8%). The present findings suggest that adverse outcomes in pregnancy during the COVID-19 pandemic period could also be related to poor quality obstetric care, social factors and difficulty in accessing healthcare.^(7)^ The actions of the Brazilian government to contain the COVID-19 pandemic disregarded global recommendations, failing to emphasize the need for social isolation or provide universal screening, with disastrous results. COVID-19 remains an active field of study, with new variants and potential new waves of infection. Our study contributes critical information to the scientific literature by detailing the risk factors and clinical course of SARS in pregnant women infected with SARS-CoV-2.
The limitations associated with the present study include the fact that the data were obtained from analyzing hospital registries, with records for different variables being missing from some charts. Therefore, much information was unknown. In Brazil, the quality of registering healthcare procedures often varies between metropolitan and non-metropolitan areas of the country, hampering access to data on hospitalizations. On the other hand, the strongpoints of the study include the number of patients evaluated and their specific characteristics. The data collected and the conclusions of our study can also serve as a basis for future research exploring the long-term sequelae of COVID-19 in pregnant women and their newborns, in addition to being useful for comparison with data from future pandemics or severe respiratory conditions that may arise. Although the study was conducted in Brazil, its conclusions have global implications, given that COVID-19 affected pregnant women worldwide. Publishing this article will expand the reach of the findings, allowing other regions and countries to learn from the experience of Northeast Brazil.
Conclusion
The most common characteristics of the patients with COVID-19 who required respiratory support included being brown-skinned, having little schooling, poor socioeconomic conditions and having been referred from another healthcare unit. The most common symptoms were headache, dyspnea, fever and dry cough. More severe respiratory findings such as respiratory distress and SpO_2_ <95% were also common in this population. Non-invasive ventilation was used in the majority of cases, followed by mechanical ventilation. Adverse obstetric outcomes were common, notably the high rate of cesarean section, presence of criteria for SARS, and COVID-19-related maternal near miss and death. Further studies should be conducted to delve deeper into the issues raised in this sample.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wastnedge EA Reynolds RM van Boeckel SR Stock SJ Denison FC Maybin JA Pregnancy and COVID-19Physiol Rev 2021101130331810.1152/physrev.00024.202032969772 PMC 7686875 · doi ↗ · pubmed ↗
- 2Mc Gonagle D O’Donnell JS Sharif K Emery P Bridgewood C Immune mechanisms of pulmonary intravascular coagulopathy in COVID-19 pneumonia Lancet Rheumatol 202027 e 437e 44510.1016/S 2665-9913(20)30121-132835247 PMC 7252093 · doi ↗ · pubmed ↗
- 3Adhikari EH Moreno W Zofkie AC Mac Donald L Mc Intire DD Collins RR Pregnancy outcomes among women with and without severe acute respiratory syndrome coronavirus 2 infection JAMA Netw Open 2020311 e 202925610.1001/jamanetworkopen.2020.2925633211113 PMC 7677755 · doi ↗ · pubmed ↗
- 4Observatório Obstétrico Brasileiro OO Br Óbitos de Gestantes e Puérperas 2022 citaado 2024 Mai 12Disponível em: https://observatorioobstetrico.shinyapps.io/obitos-grav-puerp
- 5Mc Clymont E Albert AY Alton GD Boucoiran I Castillo E Fell DB Association of SARS-Co V-2 infection during pregnancy with maternal and perinatal outcomes JAMA 202232720198319913549985210.1001/jama.2022.5906 PMC 9062768 · doi ↗ · pubmed ↗
- 6Badr DA Picone O Bevilacqua E Carlin A Meli F Sibiude J Severe acute respiratory syndrome coronavirus 2 and pregnancy outcomes according to gestational age at time of infection Emerg Infect Dis 202127102535254310.3201/eid 2710.21139434352196 PMC 8462348 · doi ↗ · pubmed ↗
- 7Ferrugini ICL Boldrini NA Costa FL Salgueiro MA Coelho PD Miranda AE SARS-Co V-2 infection in pregnant women assisted in a high-risk maternity hospital in Brazil: clinical aspects and obstetric outcomes Plo S One 2022173 e 026490110.1371/journal.pone.026490135275942 PMC 8916667 · doi ↗ · pubmed ↗
- 8Brasil. Ministério da Saúde Saiba como é feita a definição de casos suspeitos de Covid-19 no Brasil 2021 citaado 2022 Out 17Disponivel em: https://www.gov.br/saude/pt-br/coronavirus/artigos/definicao-e-casos-suspeitos