A Case Report of a Rare, but Important, Cause of Delerium Presenting to an Emergency Department
Daniel G. Miller

TL;DR
This case report highlights a rare condition causing sudden mental decline in an emergency setting, linked to a past hypoxia event.
Contribution
The paper introduces delayed post-hypoxic leukencephalopathy as a diagnosable emergency condition not previously documented in emergency medicine literature.
Findings
A 53-year-old man showed akinetic mutism 14 days after fentanyl overdose recovery.
MRI revealed symmetric frontoparietal white matter demyelination consistent with delayed post-hypoxic leukencephalopathy.
The condition can present as altered mental status days to weeks after cerebral hypoxia recovery.
Abstract
Delayed post-hypoxic leukencephalopathy is a rare cause of acute neuropsychiatric decline diagnosable in the emergency department (ED), but it has not been described in the emergency medical literature. We present a case report of a pathognomonic presentation. A 53-year-old man developed akinetic mutism 14 days after being discharged from a hospitalization for fentanyl overdose. Magnetic resonance imaging demonstrated symmetric frontoparietal white matter demyelination. Delayed post-hypoxic leukencephalopathy can present to the ED as altered mental status days to weeks after apparent full recovery from an initial episode of cerebral hypoxia. This report will help emergency physicians avoid missing this diagnosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
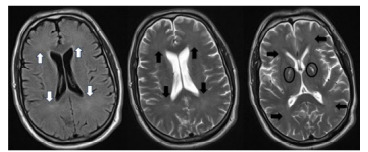 Figure 1
Figure 1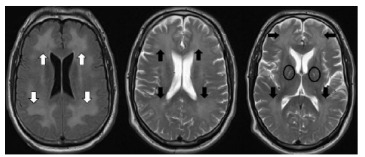 Figure 2
Figure 2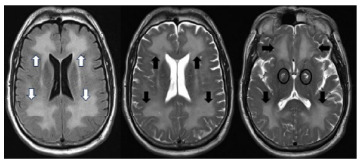 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade
INTRODUCTION
Delayed post-hypoxic leukencephalopathy (DPHL) is a demyelinating brain disorder that causes an abrupt onset of neuropsychiatric dysfunction (either acute onset of parkinsonism or akinetic mutism) days or weeks after apparent full recovery from coma following an episode of profound cerebral hypo-oxygenation. This biphasic presentation distinguishes DPHL from acute anoxic encephalopathy.1 The lucid interval (median 22 days) makes the emergency department (ED) a likely venue for presentation.2 Characteristic findings on magnetic resonance imaging (MRI) aid in diagnosis. The increasing use of MRI in EDs will give emergency physicians (EP) increasing opportunities to make (or to miss) the diagnosis of DPHL.3,4 We present a case report of a patient presenting with acute akinetic mutism three weeks after appearing to fully recover from a fentanyl overdose. His presentation demonstrates characteristic historical, physical, and imaging features of DPHL.
CASE REPORT
A 53-year-old man with no known neurologic or psychiatric history was brought to the ED after being found unresponsive after accidental fentanyl overdose. Emergency medical services initially noted apnea and percentage oxygen saturation in the 40s. After administration of naloxone and oxygen he was observed to be moving all four extremities but remained unresponsive to verbal stimuli in the ED; so, he was intubated for airway protection. Fever and hypotension prompted initiation of sepsis care. Head computed tomography (CT) showed no acute findings. A urine toxicology panel was positive for fentanyl, amphetamines, and benzodiazepines, but negative for opiates. Over the following day his vital signs stabilized, and on day three an electroencephalogram (EEG) showed no signs of epileptiform activity. He tolerated extubation and had no focal neurologic deficits. Seven days after admission he was discharged to home and resumed work.
Nineteen days after the anoxic event, family members found the patient “spaced out and drowsy” and brought him to the ED. He had normal vital signs, but speech was very slow, nearly mute, and he answered orientation questions with “I am here.” Movement was markedly slow. He would squeeze fingers placed in his palms, but he did not follow any complex commands and was incontinent of urine. Illicit drug toxicity, hypercarbia, electrolyte abnormalities, traumatic brain injury, and meningitis were all considered and were evaluated with the following studies: toxicology screening was negative, venous blood gas and chemistry profiles were normal, CT brain showed signal hyperintensity in the basal ganglia but no other acute finding, and lumbar puncture yielded clear fluid with normal cell counts and no organisms or viruses detected. An MRI (Image 1) showed hyperintensity of basal ganglia and hyperintensity of white matter tracks. This raised concern for an autoimmune encephalopathy and for opioid-related conditions that cause encephalopathy persisting long after the offending drug has been metabolized: DPHL and opioid-induced leukencephalopathy (OIL).
During inpatient care methylprednisolone 1gram was administered daily for potential autoimmune process, and plasmapheresis was initiated. He later became tremulous and diaphoretic with tachycardia, hypertension, and muscle stiffening and was intubated for airway protection and given valproate for possible seizure disorder. Subsequent EEG showed no ictal changes yet did show diffuse delta slowing consistent with encephalopathy, but not seizure. We considered neuroleptic malignant syndrome (NMS) and serotonin syndrome (SS), as well as tetanus and strychnine poisoning as causes of this change. The patient had received haloperidol early in his course, although only 2 milligrams total. As he was without fever at that time, and he had no clonus or hypereflexia, NMS and SS were unlikely. Additionally, his neurocognitive symptoms continued for several days after resolution of this acute change and without the administration of any further serotonergic or anti-dopaminergic agents, ruling out NMS and SS as causes of his ongoing inability to follow commands. Strychnine poisoning and tetanus cause muscular hyperactivity in awake patients, but our patient had depressed mental status throughout his hospital stay. While his hypertonicity began several days into his hospital course and resolved within minutes, strychnine poisoning is rapid in onset, and tetanus causes more prolonged symptoms.
CPC-EM CapsuleWhat do we already know about this clinical entity?Cerebral hypoxia can cause lasting neurologic sequelae, but emergency physicians (EP) may be unaware of delayed post-hypoxic leukencephalopathy (DPHL).What makes this presentation of disease reportable?This demonstrative emergency department (ED) case of DPHL elucidates this lesser-known cause of acutely altered mental status.What is the major learning point?When a patient presents with new-onset parkinsonism or akinetic mutism days to weeks after recovering from a profound hypoxic episode, DPHL should be considered.How might this improve emergency medicine practice?This case report will help EPs recognize DPHL, a condition that is likely to become increasingly diagnosable in the ED.
A repeat MRI (Image 2) showed progression of symmetric hyperintensity in frontal and parietal lobes and bilateral globi palidi hyperintensity otherwise sparing the gray matter; posterior circulation areas were spared.
We considered posterior reversible encephalopathy syndrome (PRESS); however, his blood pressure was within normal limits upon presentation of encephalopathy, and his condition did not improve with supportive care. Additionally, while PRESS tends to affect the cortical regions and predominates in the posterior areas of the brain, our patient’s abnormal MRI findings were seen in the subcortical regions of the frontal and parietal areas.
Both OIL and DPHL cause mutism, incontinence, confusion, and extrapyramidal symptoms. And both cause symmetric changes that predominantly affect white rather than gray matter, suggesting that myelinotoxicity is a unifying feature. In our case the biphasic presentation distinguished DPHL from OIL, in which a lucid interval after the inciting hypoxic event is not observed.5 Thirty days after his hypoxic episode an MRI (Image 3) demonstrated marked symmetric white matter signal hyperintensity in the frontal and parietal lobes with necrosis of the medial globi pallidi.
It was at this time that we considered the diagnosis DPHL to be conclusive and, given his progressive symptoms, the likelihood of recovery to be extremely low. Palliative care met with the family, and after discussions of prognosis and the patient’s known values his care we transitioned to comfort-focused care. After extubation he had spontaneous eye-opening during which time he appeared to stare at nothing and tracked neither examiners nor family members. He did not speak, follow commands, or eat when offered food. He died peacefully four days later.
DISCUSSION
Both OIL and DPHL cause abrupt neuropsychiatric decline and appear to be due to myelin disruption. Opioid-induced leukencephalopathy has commonly been described after inhalation of vaporized heroin (“chasing the dragon”) but has also been described after other methods of heroin use and after use of oxycodone. In DPHL an acute neuropsychiatric decline follows an apparent full recovery from a period of profound cerebral hypoxia. It was first described in 1936 as a sequelae of carbon monoxide (CO) toxicity and has been observed after cardiac arrest, asphyxia, drug overdose, and strangulation.6–8 Common to all causes of DPHL is a period of profound cerebral anoxia. Delayed post-hypoxic leukencephalopathy and OIL have significant clinical overlap, but there are some features to differentiate the two. As mentioned above, DPHL is characteristically biphasic while OIL is not. Whereas the neuroimaging findings in DPHL typically involve the white matter of the frontal and parietal regions, those in OIL most commonly affect the cerebellum, the posterior cerebrum, and the posterior limbs of the internal capsule.9
The decline in DPHL is characterized by symptoms that fit one or both of two categories: parkinsonism and akinetic mutism.10 Common parkinsonian symptoms are rigidity, tremor, and hallucinations. Case reports are mixed on the role of levodopa to treat DPHL-related parkinsonism; however, caution around use of antidopaminergic agents seems prudent, as these could worsen symptoms. Akinetic mutism symptoms include apathy, staring, markedly slowed speech, and functional incontinence. Presentations can overlap with both types, and common physical exam findings include frontal release signs, upper motor neuron signs, and primitive responses to noxious stimuli. This is consistent with our patient’s grasping reflexes, inanition, and periods of increased tone. Several features are suggestive that myelinotoxicity suffered during the hypoxic event leads to DPHL: The cerebral white matter is affected, while gray matter is spared, and elevation of myelin basic protein in cerebral spinal fluid is strongly associated with DPHL.11 The delayed onset of symptoms correlates with the pattern of myelin secretion occurring on average every 20 days.12
In most cases, CT will not be diagnostic, and MRI will be required for diagnosis. The following findings are pathognomonic: cerebral white matter hyperintensities seen on T2-weighted images that symmetrically affect the dorsal frontal and parietal lobes while sparing the cortex, cerebellum, and brainstem.13 On diffusion-weighted sequences a diffusion restriction involving the globi pallidi, which are traversed by numerous myelinated axons, can show high diffusion restriction, indicating cytotoxic edema.14 All these features were present in our case. These findings help distinguish DPHL from other diagnoses in the differential.
Steroids and plasmapheresis have been attempted for treatment of DPHL but have not been reported to be of benefit. Zolipidem has been reported to transiently improve alertness and orientation in patients after anoxic brain injury who are no longer comatose.15 We did not observe any improvement when we administered it to our patient. Care for DPHL is focused on support and rehabilitation if the patient can participate. Among patients with CO-associated DPHL the likelihood of recovery has an inverse relationship to age at onset. The majority of those who survived hospitalization recovered over three to six (median four) months and suffered continued difficulties related to frontal lobe function.9 For patients who progress to coma during the second phase, recovery from DPHL has not been reported.
CONCLUSION
Delayed post-hypoxic leukencephalopathy is a cause of altered mental status that EPs should consider in patients who present with acute neuropsychiatric decline days to weeks after recovering from a severe episode of cerebral hypoxia. Characteristic symptoms are new-onset parkinsonism or akinetic mutism. If an MRI is performed, specifically look at the T2 sequences for the pathognomonic findings of symmetric, white matter hyperintensity involving the anterior portion of the cerebrum, while sparing the areas supplied by posterior circulation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Messina Z Hays Shapshak A Mills R Anoxic encephalopathy Stat Pearls Treasure Island, FL Stat Pearls Publishing 2024 Available at: https://www.ncbi.nlm.nih.gov/books/NBK 539833/Accessed June 26, 202430969655 · pubmed ↗
- 2Choi IS Delayed neurologic sequelae in carbon monoxide intoxication Arch Neurol 19834074335686018110.1001/archneur.1983.04050070063016 · doi ↗ · pubmed ↗
- 3Sánchez Y Yun BJ Prabhakar AM Magnetic resonance imaging utilization in an emergency department observation unit West J Emerg Med 201718578042887492810.5811/westjem.2017.6.33992 PMC 5576612 · doi ↗ · pubmed ↗
- 4Baloescu C Diagnostic imaging in emergency medicine: How much is too much?Ann Emerg Med 2018726637433014644410.1016/j.annemergmed.2018.06.034 · doi ↗ · pubmed ↗
- 5Min SKA brain syndrome associated with delayed neuropsychiatric sequelae following acute carbon monoxide intoxication Acta Psychiatr Scand 1986731806396270710.1111/j.1600-0447.1986.tb 02671.x · doi ↗ · pubmed ↗
- 6Shillito F Drinker C Shaughnessy T The problem of nervous and mental sequelae in carbon monoxide poisoning JAMA 193610666974
- 7Hori A Hirose G Kataoka S Delayed postanoxic encephalopathy after strangulation. serial neuroradiological and neurochemical studies Arch Neurol 19914888714189826610.1001/archneur.1991.00530200113030 · doi ↗ · pubmed ↗
- 8Protass LM Delayed postanoxic encephalopathy after heroin use Ann Intern Med 19717457389555943910.7326/0003-4819-74-5-738 · doi ↗ · pubmed ↗