Retroperitoneal Necrotizing Fasciitis Following Prolonged Physical Activity: A Case Report
Jordan R. Pollock, Edmundo Chantler, Bhavesh Patel, Nelly Tan, Wayne Martini

TL;DR
A 64-year-old woman died from a rare and fast-spreading infection after a long bike ride, highlighting the importance of early detection and treatment.
Contribution
This case report adds a rare clinical scenario linking prolonged physical activity to retroperitoneal necrotizing fasciitis.
Findings
The patient developed retroperitoneal necrotizing fasciitis and acute kidney injury after a 20-mile bike ride.
Despite aggressive treatment, the patient progressed to septic shock and multiorgan failure.
Cutaneous signs of infection were absent, complicating early diagnosis.
Abstract
Retroperitoneal necrotizing fasciitis is a rare, rapidly progressive, and often fatal infection of the retroperitoneum. In many cases the source of infection is unclear, and cutaneous signs of necrotizing fasciitis may be absent. We present the case of a 64-year-old female with a history of hypertension, hyperlipidemia, and breast cancer who developed acute kidney injury (AKI) and retroperitoneal necrotizing fasciitis following a 20-mile bike ride. The patient’s initial symptoms included severe muscle aches, nausea, vomiting, and flank pain. Diagnostic imaging and laboratory results indicated myositis and severe AKI. Despite aggressive treatment with antibiotics, intravenous fluids, and pain management, the patient developed septic shock and multiorgan failure, ultimately leading to her death. This case highlights the rapid progression and complexity of managing necrotizing fasciitis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
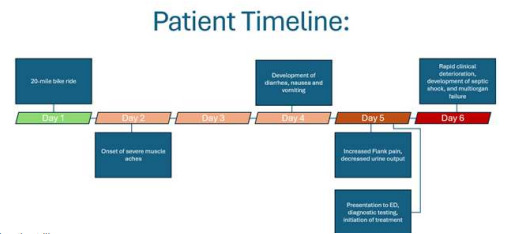 Figure 1
Figure 1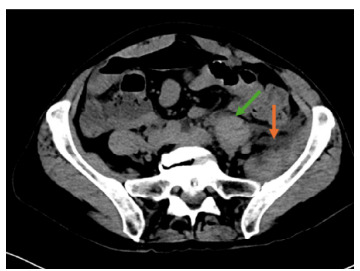 Figure 2
Figure 2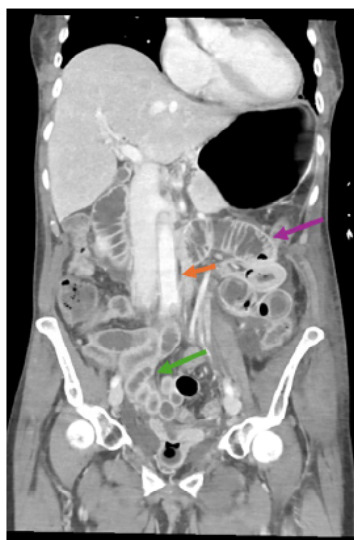 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMuscle and Compartmental Disorders · Streptococcal Infections and Treatments
INTRODUCTION
Retroperitoneal necrotizing fasciitis is a rare, rapidly progressive and often fatal infection of the retroperitoneum. This infection has a high mortality rate, estimated to be 40–60%.1 In many cases the source of infection is unclear. A systematic review of peritonitis caused by streptococcus found that 69% of patients developed the infection from an unknown source, 16% of patients’ source of infection was from ascending vaginal infection, 9% from a droplet infection, and 6% from pharyngitis.2
Cutaneous manifestations of necrotizing fasciitis, such as necrosis and erythema, will often present in patients with a defined infectious source such as a wound or surgical site. However, according to another study, more than half of patients with necrotizing fasciitis had no defined portal of entry and arrived to the emergency department (ED) with the main symptom of increasingly severe pain. This pain can begin at a site of recent trauma such as a joint injury, hematoma, or muscle strain.3
CASE REPORT
A 64-year-old female with a history of hypertension managed with lisinopril, hyperlipidemia, and breast cancer status post mastectomy and current letrozole use presented to the ED with severe muscle aches, nausea, vomiting, diarrhea, decreased urine output, frontal headache, and flank pain. She was physically active most days of the week including walking, running, and occasional bicycle riding. Four days prior to arrival, the patient had completed a challenging 20-mile bike ride on a summer day. Three days prior to arrival, she developed severe muscle aches. One day before arrival, she experienced diarrhea, nausea, vomiting, and headache. The patient came to the ED due to these symptoms, in addition to left flank pain and decreased urine output. (See Figure for a timeline of patient illness.)
The patient had never smoked or used smokeless tobacco. She consumed about 10 alcoholic drinks per week. She had a family history of hypertension. She had recently traveled from Utah to Arizona after her biking trip. On presentation, she appeared anxious with a heart rate of 70 beats per minute and respirations of 20 breaths per minute; she was afebrile at 36.6 °Celsius and hypertensive to 138/99 millimeters of mercury. Her oxygen saturation was 100% without supplemental oxygen use. The patient rated her flank pain a 10/10. On physical examination, the patient had a normal cardiovascular and pulmonary exam. There was moderate pain to palpation of the left middle and left lower flank, with mild right lower quadrant abdominal tenderness.
Initial laboratory results indicated a white blood cell count (WBC) of 6.1 × 10^9^ cells per liter (L) (reference range: 4.5–11.0 × 10^9^/L) and hemoglobin of 13.4 grams per deciliter (g/dL) (11.6–15.0 g/dL). She had a sodium of 129 millimoles (mmol) per L (135–145 mmol/L), chloride 92 mmol/L (98–107 mmol/L), bicarbonate 18 mmol/L (22–29 mmol/L), and anion gap of 19 (7–15). She had a severe acute kidney injury (AKI) with a creatinine of 4.25 milligrams (mg)/dL) (patient baseline 0.8, reference range 0.59–1.04 mg/dL) and an elevated blood urea nitrogen of 45 mg/dL (6–21 mg/dL). Her lactate was elevated to 4.1 mmol/L (0.5–2.2 mmol/L) and creatine kinase (CK) of 200 units (U)/L (2–192 U/L). Influenza A, influenza B, respiratory syncytial virus, and coronavirus polymerase chain reaction tests were negative.
Diagnostic imaging with computed tomography of the abdomen and pelvis without contrast due to her kidney injury revealed heterogeneous hyperattenuation and asymmetric enlargement of the left quadratus lumborum muscle, external oblique muscle, left psoas major muscle, and iliacus muscle (Image 1).
CPC-EM CapsuleWhat do we already know about this clinical entity?Retroperitoneal necrotizing fasciitis is a rapidly progressive disease associated with a high morbidity and mortality.What makes this presentation of disease reportable?This is a rare case of retroperitoneal necrotizing fasciitis without a clear infectious source and an initially non-specific disease presentation.What is the major learning point? Retroperitoneal necrotizing fasciitis does not always have a clear infectious source and should be considered when in the setting of severe pain or organ failure.How might this improve emergency medicine practice?Early recognition of retroperitoneal necrotizing fasciitis requires a broad differential and recognition of rapidly progressive multisystem organ failure.
The patient was admitted to internal medicine for treatment of her AKI, elevated lactic acid, and pain, and she was treated with aggressive antibiotics including cefepime 1 gm intravenously (IV), doxycyline 100 mg IV, linezolid 600 mg IV, and metronidazole 500 mg IV. She was also treated with IV fluid resuscitation and pain management with morphine 2 mg and multiple 1 mg doses of hydromorphone. She was also given hydrocortisone 50 mg and IV immune globulin (human) 10% infusion 20 g. The patient started continuous renal replacement therapy due to her AKI and subsequent severe metabolic acidosis.
Five hours after admission, the patient developed rapidly progressive multiorgan failure that presented as a possible stroke, after which she was intubated, and additional imaging was obtained (Image 2). Her CK increased from 200 to 5,535 U/L, serum creatinine from 4.25 to 4.41 mg/dL, blood urea nitrogen from 45 to 51 mmol/L, and WBC decreased from 6.9 to 3.7 × 10^9^ cells/L.
Surgical consultation was obtained due to suspicion of necrotizing fasciitis, for which the patient was deemed inoperable due to the extensive organ involvement of the infection. A muscle biopsy was obtained and confirmed to be group A Steptococcus pyogenes. The patient was transitioned to comfort care after family discussions of these findings. She died shortly thereafter due to multiorgan failure and septic shock.
DISCUSSION
In patients with no defined infectious source, the severe pain associated with necrotizing fasciitis can precede cutaneous evidence of infection by 12–24 hours. In our case, the patient presented with increasingly severe left flank pain followed by cutaneous findings of necrotizing fasciitis after admission to the hospital. She did not present with an increased WBC on initial presentation, possibly due to her use of letrozole for breast cancer.
The treatment of necrotizing fasciitis includes early recognition, administration of broad spectrum IV antibiotics, and surgical debridement.4 Retroperitoneal necrotizing fasciitis is a rare, aggressive infection associated with a high mortality. A case report of a young, healthy, 33-year-old female patient is similar to our case. She presented to the ED with generalized abdominal pain suspected to be due to gastroenteritis, and a CT demonstrated intrabdominal fluid likely secondary to a ruptured corpus luteal cyst. The patient returned with worsening pain, with repeat CT demonstrating worsening free fluid and evidence of peritonitis. Subsequently laparoscopy confirmed peritonitis with no identified infectious source, with cultures positive for group A S. pyogenes.5 Intra-abdominal necrotizing fasciitis should be part of a broad differential considered in the ED to reduce the mortality and morbidity associated with this condition. One tool is the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score to distinguish necrotizing fasciitis from severe cellulitis or abscess, which takes into account C-reactive protein, WBC, hemoglobin, sodium, creatinine, and glucose.6
In another case, a 33-year-old man had a three-week history of back ache due to trauma, followed by fever, vomiting, and severe left flank pain, which was then diagnosed as retroperitoneal necrotizing fasciitis due to Escherichia coli. The source for this patient was unclear, similar to our patient.7 However, our patient had gone mountain biking for 20 miles, which could have been a source of trauma and back pain for her. In cases of trauma and hematoma formation, necrotizing fasciitis has been known to infect these areas. For example, a 26-year-old man presented with severe pain in his right biceps, which he attributed to a muscle tear, and was diagnosed as a muscle belly tear with hematoma formation. The patient returned four days later with necrotic skin and erythema of the upper extremity and grew group F β-hemolytic streptococci and Bacteroides.8
In our case the source of the patient’s retroperitoneal necrotizing fasciitis remains unclear, but contributing factors included her recent strenuous bike ride and use of letrozole for breast cancer. Kejela et al described 14 cases of retroperitoneal necrotizing fasciitis, with infection sources ranging from Fournier gangrene, fistula, and abscess to perforated diverticulitis, renal stone, and “none.”9
CONCLUSION
This case highlights the rapid progression and complexity of managing necrotizing fasciitis and acute kidney injury in the context of rhabdomyolysis. Early recognition and aggressive management are crucial in cases of suspected necrotizing fasciitis and AKI. Early involvement of a multidisciplinary team can improve patient outcomes in complex and rapidly deteriorating patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tarekegn NG Moges TG Guluju FA Retroperitoneal necrotizing fasciitis mimicking perforated appendicitis: a case report Int J Surg Case Rep Mar 20241161094123838214510.1016/j.ijscr.2024.109412 PMC 10943963 · doi ↗ · pubmed ↗
- 2Westwood DA Roberts RH Management of primary group A streptococcal peritonitis: a systematic review Surg Infect (Larchmt)Apr 201314217162346467810.1089/sur.2012.038 · doi ↗ · pubmed ↗
- 3Stevens DL Bryant AE Severe group A streptococcal infections Ferretti JJ Stevens DL Fischetti VA Oklahoma City, OK University of Oklahoma Health Sciences Center Streptococcus pyogenes: Basic Biology to Clinical Manifestations 201626866208 · pubmed ↗
- 4Wallace HA Perera TB Necrotizing fasciitis Stat Pearls 2024 https://www.ncbi.nlm.nih.gov/books/NBK 430756/ Accessed January 5, 202528613507 · pubmed ↗
- 5Aw AEY Lee JWK Tay KV Primary peritonitis secondary to streptococcus pyogenes in a young female adult: a case report and literature review Infect Dis Rep Jan 1202113126323340139910.3390/idr 13010005 PMC 7838986 · doi ↗ · pubmed ↗
- 6Bechar J Sepehripour S Hardwicke J Laboratory risk indicator for necrotising fasciitis (LRINEC) score for the assessment of early necrotising fasciitis: a systematic review of the literature Ann R Coll Surg Engl May 20179953413462846264710.1308/rcsann.2017.0053 PMC 5449710 · doi ↗ · pubmed ↗
- 7Giri S Kandel BP Kansakar PB Retroperitoneal necrotizing fasciitis presenting with peritonism in a 33-year-old Nepalese man: a case report J Med Case Rep Feb 1020126532232536810.1186/1752-1947-6-53PMC 3296598 · doi ↗ · pubmed ↗
- 8Dunn F Two cases of biceps injury in bodybuilders with initially misleading presentation Emerg Med J Sep 200219546121220500910.1136/emj.19.5.461PMC 1725952 · doi ↗ · pubmed ↗