Surface Anatomy and Sensory Evaluation of Dermatomes: A Guide for Residents
Balamurugan Rajendran, Muhammad Asyraf Yunos, Harivarmah Nagalinggam, Mohamad Lokman Abdul Aziz, Jafri Malin Abdullah

TL;DR
This paper explains the surface anatomy of dermatomes and sensory evaluation to help medical trainees in Malaysia identify neurological issues.
Contribution
It provides a guide tailored for Malaysian medical students and trainees on lesion localisation using dermatome anatomy and sensory exams.
Findings
Dermatome surface anatomy and sensory points are described for the face and body.
The guide aims to improve lesion localisation skills for neurological disorders.
It supports medical trainees in conducting effective sensory and neurological examinations.
Abstract
The surface anatomy of dermatomes and sensory examination play crucial roles in assessing and diagnosing various medical conditions. Understanding the distribution of dermatomes and conducting sensory examinations are essential in identifying and localising neurological disorders, such as nerve damage or compression. This manuscript describes the surface anatomy of the face and body and their respective key sensory examination points for sensory and neurological examination to aid Malaysian medical students and trainees in lesion localisation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
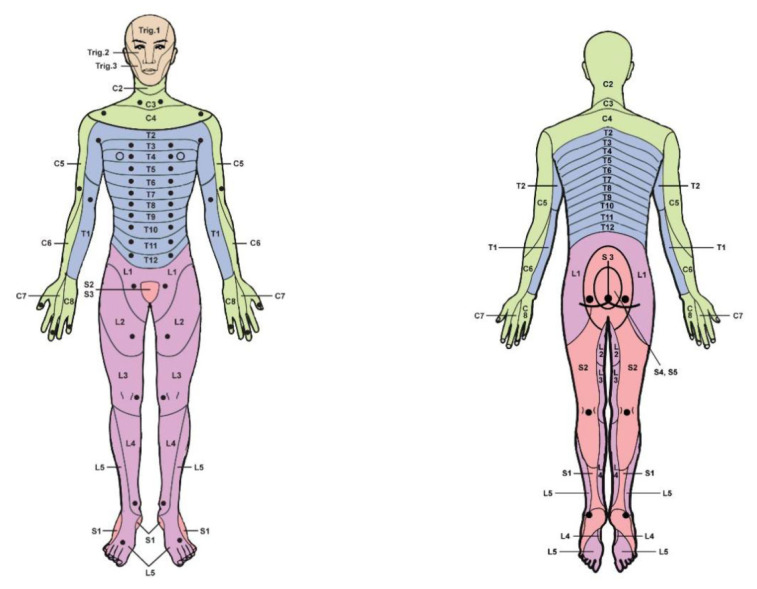 Figure 1
Figure 1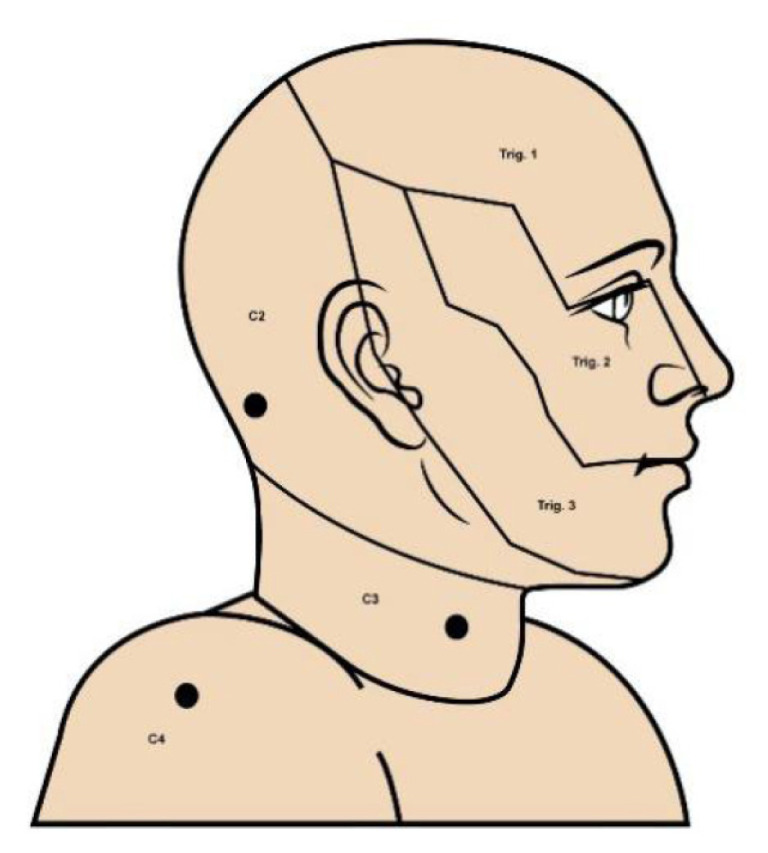 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management
Introduction
Sensory examination is critical in neurological examination and diagnostic assessment, particularly in lesion localisation (1). The primary aim of sensory testing is to validate sensory integrity and to unravel the complex interactions between the central nervous system and peripheral nervous system, thereby guiding us in localising the lesion (2).
The skin is divided into several areas known as dermatomes. Dermatomes, which are specific areas of skin innervated by sensory nerves emerging from a single spinal nerve root (3, 4), are the cornerstone of sensory testing. During vertebrate development, the somite gives rise to the sclerotome, myotome, and dermatome (3). The sclerotome develops into the vertebrae, the myotome into the skeletal muscle, and the dermatome into the skin (3). Each dermatome comprises a patch of skin covered in nerve fibres that provide sensory to the corresponding spinal root (5).
This article provides a comprehensive overview of dermatomes, their anatomical basis, and their clinical significance in the sensory examination.
History and Development of Dermatome Models
The history of dermatome mapping showcases the evolution of scientific exploration of the nervous system, starting with basic observations and leading to the creation of clinically essential tools.
Early studies, especially those conducted by Sir Henry Head in 1893, were crucial in identifying the segmental patterns of skin innervation based on the lesion distribution caused by herpes zoster (shingles) (6). Head’s dermatome maps, although limited by subjective data and variability among patients, were the first to illustrate the connection between spinal nerves and specific regions of skin sensation (7). These findings mark a crucial step in understanding the connection between nerve roots and sensory distribution, paving the way for significant advancements that followed.
Subsequent studies, especially those conducted by Otto Foerster in 1933, significantly advanced the field. Foerster employed a systematic approach that included rhizotomy, the surgical severance of nerve roots, to investigate sensory loss in individual dermatomes (8, 9). His work led to a more precise understanding of dermatomes, emphasising their overlap and variability (8). By systematically correlating sensory deficits with the affected spinal nerves, Foerster’s research provided strong evidence that became the foundation for modern dermatome maps (8). Later, in 1948, Keegan and Garrett refined these maps by examining the limb’s segmental distribution of cutaneous nerves (10).
Based on a literature systemic review by Lee et al. (11), Table 1 summarises the three standard dermatome maps and the quality of evidence based on the review. Two commonly used and accepted maps are the Keegan and Garrett map (10) and the Foerster map (3), the latter of which is featured in the American Spinal Injury Association scale of assessing spinal injury (12, 13).
Discrepancies in dermatome maps arise from methodological differences, population variability, and the complexity of sensory nerve distributions (4, 7). Early maps, like those by Head, relied on clinical observations, while later maps by Foerster, Keegan and Garrett used experimental approaches, leading to variations in defining boundaries. Genetic diversity and anatomical variations among populations investigated can yield different findings (7). Another discrepancy stems from the contrast between clinical and embryological perspectives. Embryological maps focus on the developmental origins of dermatomes from somites, while clinical maps are based on sensory loss among patients (11, 14). The overlap between dermatomes and sensory compensatory mechanisms further complicates the consistency of these maps.
According to Foerster (3), Keegan and Garrett (10), each dermatome overlaps with an adjacent dermatome. Dermatome overlap is an inherent feature of the nervous system and has evolutionary, anatomical, and functional origins. From an evolutionary perspective, overlap ensures redundancy in sensory innervation, reducing the risk of complete sensory loss if a single nerve root is damaged (11). Anatomically, the formation of nerve plexuses, such as the brachial and lumbar plexuses, contributes to the blending of fibres from adjacent spinal nerves. This anatomical intertwining results in the innervation of a single skin area by multiple nerve roots, particularly in regions like the trunk (15). Functionally, this overlap allows adjacent nerves to compensate for sensory input, maintaining sensation even when one nerve is compromised (16). This redundancy is vital for protecting the body from environmental hazards.
The extent of dermatome overlap is most evident in the trunk, where the sensory territories of adjacent nerves often blend extensively (4, 7). In contrast, overlap is less pronounced in distal areas like the hands and feet, where sensory territories are more distinct (4). This variation in overlap has significant clinical implications. For instance, the extensive overlap in the trunk can make it challenging to pinpoint the exact nerve root involved in a sensory deficit. In contrast, the less pronounced hand and foot overlap can provide more reliable diagnostic information.
Interindividual dermatome variation can occur due to intersegmental anastomoses of posterior spinal rootlets (17). This term refers to the situation when the sensory neurons of a dorsal root ganglion enter the spinal cord at a different level, leading to a potential overlap in the sensory territories of adjacent dermatomes (17, 18). Understanding the distribution of dermatomes is crucial for diagnosing and treating neurological and spinal cord injuries. The boundaries between respective dermatomes supplied by each nerve root could have been more precise due to some overlap between adjacent nerve territories (16). For example, sensory changes in the L5 dermatome may also reflect contributions from L4 and S1, complicating the identification of a specific lumbar nerve root lesion.
Surface Anatomy and Key Examination Points
Dermatomes, the intricate components of the human nervous system, transmit sensory information from the skin. The distribution of dermatomes on the thorax and abdomen, in a striped pattern, and their dip inferiorly as they course from posterior to anterior present a fascinating complexity (17). However, the unique patterns of the upper and lower limb dermatomes, influenced by the early embryonic stages of limb development, captivate the imagination and add another layer of intrigue to their study (17).
To better comprehend the distribution of limbs dermatome, envision someone standing upright with their limbs abducted and thumbs pointing upwards. In this position, the dermatomes aligned as before the limbs rotated (18). It is essential to note that the innervation region of peripheral nerves is not equivalent to dermatomes (18). Peripheral nerves are derived from various plexuses, including brachial, lumbar, and sacral, which contain fibres from multiple spinal nerves (18).
Cervical 1 (C1) root does not have a dermatome to be tested (15). Dermatomal levels according to the Foerster map and the international standards booklet for neurological and functional classification of spinal cord injury have been summarised in Table 2 (13, 19) and illustrated in Figure 1.
Their reliability and safety underpin the committee’s recommendation of key sensory points. Each point corresponds to a specific dermatome identified in widely recognised anatomical references, providing a solid foundation for examination (13, 19). Furthermore, these points are associated with anatomically distinct bony landmarks, making them safe and easy to locate. This recommendation ensures consistency and reliability among examiners, instilling confidence and security in the process and the results (19).
Face sensory, on the other hand, is supplied by the trigeminal cranial nerve, which gives rise to three cutaneous branches: ophthalmic, maxillary, and mandibular nerve. Each branch of the trigeminal nerve supplies the face according to its distribution, as shown in Figure 2 (20). The key examination point of each dermatome can be described according to the plastic aesthetic unit, a concept in plastic surgery that divides the face into distinct regions based on the natural lines and contours of the face and based on the surface tension lines (21). Table 3 summarises the dermatome distribution of trigeminal nerve branches supplying the face and the key sensory examination points.
Despite these tools, the variability in sensory territories necessitates clinicians to adopt a comprehensive approach. Dermatome testing alone may not reliably localise lesions, underscoring the importance of complementary diagnostic tools such as imaging and electrophysiological studies. Magnetic resonance imaging can identify structural abnormalities affecting spinal nerves, while nerve conduction studies and somatosensory evoked potentials can confirm the functional integrity of sensory pathways. Together, these methods enhance the accuracy of diagnosis, highlighting the crucial role of medical professionals in ensuring conclusive clinical findings.
Sensory Examination Technique
There are two types of sensation: exteroceptive and proprioceptive (22). Exteroceptive sensation, or superficial sensation, involves skin and mucous membrane receptors. It includes tactile or touch sensation, pain sensation, and temperature sensation. The segmental distribution of proprioceptors does not follow the dermatomal map but is closely associated with the muscle innervation pattern (22).
The spinal nerve root sensory level can be graded using the American Spinal Injury Association chart (19), a standardised tool for assessing sensory and motor function in patients with spinal cord injury. The chart assigns a grade to the sensory level according to the relevant dermatome described in Table 2 or Figure 1.
Grading scale for sensation (with comparison to the sensation on the patient’s reference point):
0: Absent, no response1: Altered (impaired or partial appreciation, including hyperesthesia)2: Normal or intact (similar to reference point)NT: Not testable
Sensory examination is a crucial neurological assessment that requires the patient’s optimal cooperation in a comfortable environment (2). The examiner should explain each procedure and what is expected from the patient. Before starting, the patient must be asked if they have experienced abnormal sensations, numbness, or pain in any part of their body. Establish a baseline by ensuring the patient has normal sensation on the forehead or sternum (reference point) and whether they can feel the test object as soft or sharp (22).
Pain examination begins with demonstrating the test on the forehead as a reference point with a neurotip or neurological pin. The examiner then gently pricks the skin, maintaining even pressure over each dermatome C2–S5 bilaterally on the key sensory examination point while the eyes are closed or vision is blocked. The patient’s feedback is crucial, as they should indicate whether the sensation is equal, increased, decreased, or absent compared to the forehead.
The examination was then repeated to assess soft touch using a wisp of cotton wool or 10g Semmes-Weinstein monofilament and temperature using two test tubes with stoppers: one be filled with cold water (between 5°C and 10°C) and the other with warm water (40°C to 45°C). This temperature range ensures an accurate assessment of temperature sensation without overlapping with pain perception, making it a reliable tool for temperature testing in neurological examinations. Examination of two-point discrimination would be conducted by repeating similar steps using a two-point discrimination aesthesiometer.
A detailed step-by-step guide for sensory examination, including visual aids and the rationale for using the respective assessment tools, has been covered by Khoo et al. (22). Please refer to the YouTube videos: https://youtu.be/dcPzgx5kzjY and https://youtu.be/5EhlG9l2wHo
Conclusion
Dermatome and sensory examination are not just tasks but are crucial in assessing and diagnosing various medical conditions. An appropriate examination technique is essential to lessen the disparity between examiners. We hope medical trainees and staff can use this method for neurological assessments.
The link to the dermatome anatomy examination video, a valuable resource for your learning, is readily available at the following link: https://youtu.be/7frtOoeppuo
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Apok V Gurusinghe NT Mitchell JD Emsley HCA Dermatomes and dogma Pract Neurol 201111210010510.1136/jnnp.2011.24222221385968 · doi ↗ · pubmed ↗
- 2O’ Sullivan SB Schmitz TJ Fulk GD Examination of sensory function Chui KK Schmitz TJ Physical rehabilitation 6th ed Mc Graw-Hill Eucation 201487118
- 3Patel S Human dermatomes Tubbs RS Rizk EB Shoja MM Loukas M Barcaro N Spinner RJ Nerves and Nerve Injuries 1st ed Elsevier Ltd 201547748310.1016/B 978-0-12-410390-0.00036-6 · doi ↗
- 4Joseph SC Loukas M History of the dermatomes Tubbs RS Rizk EB Shoja MM Loukas M Barcaro N Spinner RJ Nerves and Nerve Injuries 1st ed Elsevier Ltd 201548549310.1016/B 978-0-12-410390-0.00037-8 · doi ↗
- 5Greenberg SA The history of dermatome mapping Arch Neurol 20036012613110.1001/archneur.60.1.12612533100 · doi ↗ · pubmed ↗
- 6Schott GD Henry Head, herpes zoster and the graphic development of his “scheme of the dermatomes in man.”J Neurol Neurosurg Psychiatr 201788978979310.1136/jnnp-2016-31545628416562 · doi ↗ · pubmed ↗
- 7Downs MB Laporte C Conflicting dermatome maps: educational and clinical implications J of Orthop Sports Phys Ther 201141642743410.2519/jospt.2011.350621628826 · doi ↗ · pubmed ↗
- 8Tan TC Black PM The contributions of Otfrid Foerster (1873–1941) to neurology and neurosurgery Neurosurgery 20014951231123610.1227/00006123-200111000-0003811846917 · doi ↗ · pubmed ↗