What is Really Refractory Intracranial Hypertension in The Paediatric Group in 2025? Suggestions for ICP and CPP Guidance for Early Intervention in Malaysia
Shah Ozair Shaharuddin, Jafri Malin Abdullah

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
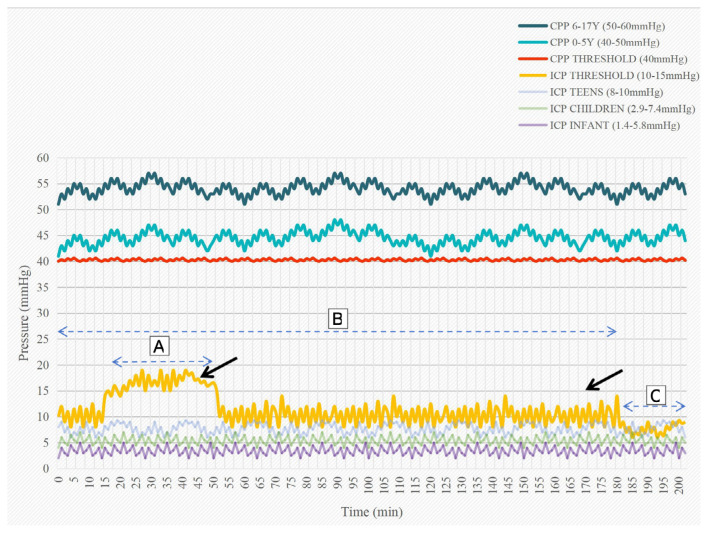 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Visual Health Research · Cerebral Venous Sinus Thrombosis · Neonatal and fetal brain pathology
Dear Editor,
We read with great interest the article entitled “Prognostic Factors of Severe Traumatic Brain Injury Outcome in Children Aged 2–16 Years at a Major Neurosurgical Referral Centre”, which was published in the Malaysian Journal of Medical Sciences in 2009 (1).
Sixteen years since the publication of the article, multiple published guidelines have concurred that a standard intracranial pressure (ICP) of above 20 mmHg indicates a poor prognostic outcome across paediatric population (2–8). The wide age range from birth to adulthood makes the ICP cut-off point becomes physiologically precarious in the management of neonates, infants, and young children in the intensive care unit (ICU) (2, 3, 9). However, to date, no ICP threshold value has been established for each age group in the paediatric population.
We highlight that recent advanced studies have evidently shown via decay curves that paediatric patients are less tolerant of ICP increases than adult patients (7–9). Using pressure-time-dose studies, poor outcomes were extrapolated in paediatric patients with 30-minute ICPs > 15 mmHg and 150-minute ICPs >10 mmHg across all age groups (9).
As shown in Figure 1, we hypothetically postulate that a more aggressive treatment should be administered 5 minutes before the 30-minute threshold for elevated ICPs > 15 mmHg and 10 minutes before the 150-minute threshold for elevated ICP > 10 mmHg. However, continuous management of intracranial hypertension should be performed at any time to avoid prolonged elevated ICP (2, 3, 10–12).
Therefore, we strongly support the need to reduce the elevated ICP threshold for ICU paediatric patients. For the past 30 years, Malaysia has seen a significant paradigm shift in ICP management for paediatric patients with traumatic brain injury, especially towards improving the future outcome of childhood brain trauma, which is common in the country.
In addition, cerebral perfusion pressure (CPP) is a key factor that influences the outcome of traumatic brain injury. Recent studies have concluded that paediatric patients should have a CPP > 40 mmHg. Figure 1 shows the target CPP ranges for two paediatric age groups (5, 13–15).
We acknowledge that recently published studies have reported that CPPopt, ΔCPP, and PRx have predictive values for the outcome of traumatic brain injury (5). Thus, we encourage further studies to provide evidence to support their findings in paediatric populations with traumatic brain injury.
Figure 1 summarises CPP values and ICP values. Target CPPs (CPP 6 to 17 years, and CPP 0 to 5 years) (3, 4, 15). CPP Threshold is, in actuality, a single value of 40mmHg, which should be avoided as values lower than this carry a strong, independent risk factor for poor outcome (2). “Physiological” ICP for teens, children, and infants (16, 17) are shown as a guide and comparison to ICP threshold. ICP threshold constitutes a set of values of ICP above 15 mmHg for 30 minutes (dashed line A) and ICP above 10 mmHg for 150 minutes (dashed line B) are not tolerated by the paediatric age group, and the timing of intervention shall be taken within this period of time (thick black arrows) to control the ICP (9) (dashed line C).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kan CH Saffari M Khoo TH Prognostic factors of severe traumatic brain injury outcome in children aged 2–16 years at a major neurosurgical referral centre Malays J Med Sci 2009164253310.21315/mjms 2017.24.1.1PMC 321613722135509 · doi ↗ · pubmed ↗
- 2Adelson PD Bratton SL Carney NA Chestnut R Mdu Coudray HEM Goldstein B Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Chapter 6. Threshold for treatment of intracranial hypertension Pediatr Crit Care Med 200343 Suppl S 25S 2712847342 · pubmed ↗
- 3Kochanek PM Tasker RC Carney N Totten AM Adelson PD Selden NR Guidelines for the management of pediatric severe traumatic brain injury, third edition Pediatr Crit Care Med 2019203 SS 1S 8210.1097/PCC.000000000000173530829890 · doi ↗ · pubmed ↗
- 4Lui A Kumar KK Grant GA Management of severe traumatic brain injury in pediatric patients Front Toxicol 2022491097210.3389/ftox.2022.91097235812167 PMC 9263560 · doi ↗ · pubmed ↗
- 5Svedung Wettervik T Velle FHånell A Howells T Nilsson P Lewén AICP, P Rx, CPP, and ΔCP Popt in pediatric traumatic brain injury: the combined effect of insult intensity and duration on outcome Childs Nerv Syst 2023392459246610.1007/s 00381-023-05982-537270434 PMC 10432317 · doi ↗ · pubmed ↗
- 6Skoglund TS Nellgård B Long-time outcome after transient transtentorial herniation in patients with traumatic brain injury Acta Anaesthesiol Scand 200549333734010.1111/j.1399-6576.2005.00624.x 15752399 · doi ↗ · pubmed ↗
- 7Güiza F Depreitere B Piper I Citerio G Chambers I Jones PA Visualizing the pressure and time burden of intracranial hypertension in adult and paediatric traumatic brain injury Intensive Care Med 2015411067107610.1007/s 00134-015-3806-125894624 · doi ↗ · pubmed ↗
- 8Donnelly JGüiza F Depreitere B Meyfroidt G Czosnyka M Smielewski P Visualising the pressure-time burden of elevated intracranial pressure after severe traumatic brain injury: a retrospective confirmatory study Br J Anaesth 20211261 e 15e 1710.1016/j.bja.2020.09.01833183738 · doi ↗ · pubmed ↗