Multidrug-Resistant Candida auris and its Role in Carcinogenesis: A Scoping Review
Wan NurHazirah Wan Ahmad Kamil, Mukarramah Zainal, H.M.H.N. Bandara, Mohd Hafiz Arzmi

TL;DR
This paper reviews the link between multidrug-resistant Candida auris and cancer, finding that while C. auris infections increase cancer patients' susceptibility, they are not directly linked to cancer development.
Contribution
The study is the first to systematically review the potential role of C. auris in carcinogenesis and its risk factors in cancer patients.
Findings
C. auris infections are more common in cancer patients due to their weakened immune systems.
No direct evidence links C. auris to cancer development due to limitations in diagnostic tools.
Accurate detection methods and infection control measures are urgently needed for cancer patients.
Abstract
Candida auris was listed as a critical fungal priority group pathogen by the World Health Organization (WHO) in 2022. It has become a leading cause of invasive candidiasis in serious nosocomial infections globally. While Candida species, particularly C. albicans, are linked to cancer development, the role of C. auris in carcinogenesis remains unexplored. This scoping review aimed to evaluate the existing evidence on the role of C. auris infection in carcinogenesis and its associated risk factors. Following the PRISMA-ScR guidelines, a comprehensive search of three databases was conducted from January 2003 to January 2024 to identify studies addressing the role of C. auris infection in cancer development and its associated risk factors. A total of 124 articles were identified, of which six met the inclusion criteria. These studies reported the risk factors associated with C. auris…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
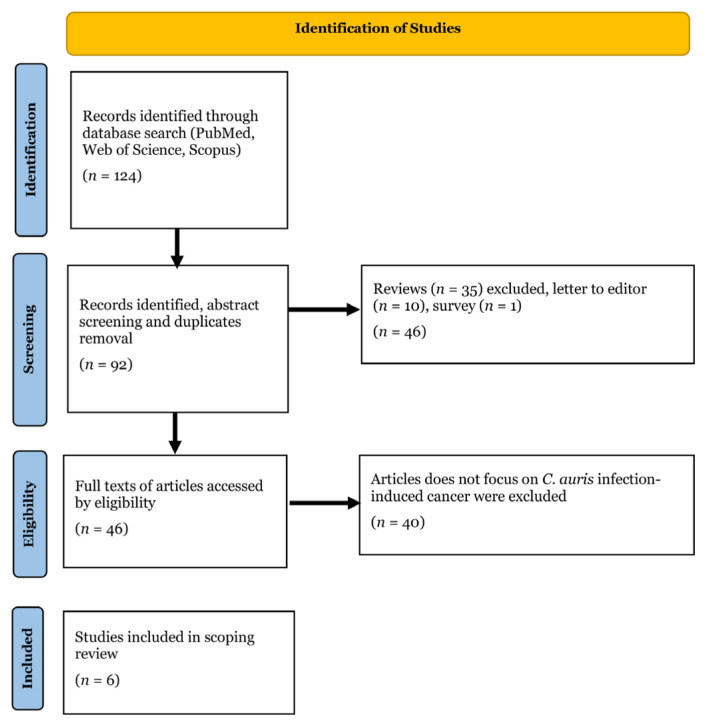 Figure 1
Figure 1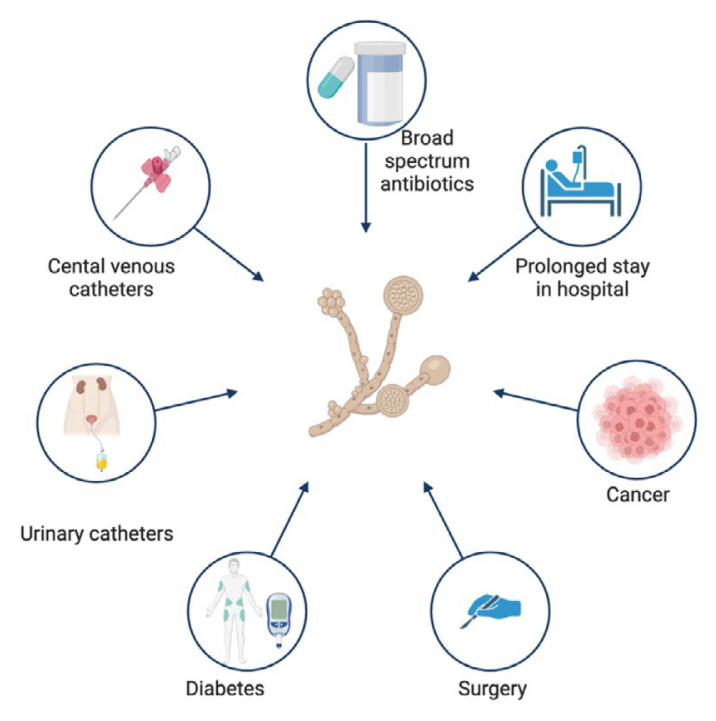 Figure 2
Figure 2- —Ministry of Higher Education, Malaysia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Pneumocystis jirovecii pneumonia detection and treatment
Introduction
Since 2022, Candida auris (C. auris) has been categorised as a critical group of fungal pathogens by the World Health Organization (WHO) due to its ability to cause invasive candidiasis in healthcare settings (1). It was first identified in 2009 in over 40 countries, with alarming morbidity and mortality rates, especially in immunocompromised individuals (2). C. auris infection has been reported in several Asian countries, including Malaysia and Singapore. In Malaysia, the first fatal case of C. auris infections was reported in a neutropenia patient (3).
Epidemiological studies revealed that C. auris infections are primarily associated with healthcare facilities, particularly intensive care units, long-term care facilities, and hospitals (4). The overall mortality of invasive candidiasis with C. auris ranged from 29% to 53% (1). Cancer patients are among the populations at a higher risk of C. auris infections due to their compromised immune systems and frequent exposure to healthcare environments, making them susceptible to infections (2, 5). The pathogen can be easily transmitted from patient to patient, potentially contaminating the healthcare environment and leading to outbreaks (6, 7).
Cancer is the leading cause of death worldwide, posing a threat to life expectancy in every country regardless of the level of economic development (8). According to GLOBOCAN 2022, an incidence of 19,976,499 cancer cases have been reported, with 9,743,832 deaths in 2022 (9). As the disease advances, uncontrolled cell growth and tissue invasion occur, leading to distant metastases. Metastases are the main cause of cancer-related death (9). This disease advancement promotes the shedding of malignant cells from the primary site tumour to distant organs via the bloodstream, where they attach and grow, mimicking the behaviour of the primary tumour (9).
Recent studies have suggested a connection between yeast infection and an increased risk of developing certain types of cancer (10, 11). These infections are reportedly involved in cancer development, such as cancer initiation, establishment, and spread (12, 13). Candida infections are often associated with a weakened immune system. Individuals with compromised immune systems, such as those undergoing cancer treatment or HIV/AIDS patients, are susceptible to Candida infections, including C. auris, which is common in cancer patients, especially those undergoing chemotherapy (14, 15).
Given the growing threat of C. auris and its potential impact on cancer patients, it is crucial to understand the current epidemiology, risk factors, clinical manifestations, and management strategies for this emerging fungal pathogen. The association between C. auris infections and cancer involves various aspects, including clinical, epidemiological, and microbiological. However, the role of C. auris in carcinogenesis remains unclear. This scoping review aims to elucidate the association between C. auris infections and cancer, synthesising findings from various studies highlighting the epidemiology, clinical characteristics, and risk factors of C. auris infections in cancer patients.
Methods
Data Sources
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines (16, 17). The literature review was based on a search of PubMed, Scopus, and Web of Science databases for articles dealing with in vitro, in vivo, ex vivo trials, case reports, retrospective studies, and observational studies reporting the association of C. auris infection in carcinogenesis, dated between January 2003 to January 2024. The following search string was applied to the databases: “(Candida auris or “C. auris”) and (cancer* OR carcinogenesis OR oncogenesis)” [PubMed] and “(Candida auris) and (infection)” [Scopus and Web of Science].
Inclusion Criteria
The works included in the scoping review include:
Papers dealing with in vitro, in vivo, and ex vivo trials reporting C. auris infection associated with carcinogenesis.Retrospective analyses, observational studies, and case reports related to C. auris infection in cancer patients.
Exclusion Criteria
The works excluded from the scoping review include:
Reviews, book chapters, and letters to editors.Articles discussing Candida infection without C. auris.Non-English articles.
Selection of Articles
The electronic literature searches in PubMed, Scopus, and Web of Science databases resulted in 124 articles. Three independent reviewers (WNH, MZ, and MHA) were unanimous regarding the literature selection process. After applying the exclusion and meeting the inclusion criteria, only six articles were included in the scoping review. The selection process of the articles is demonstrated in Figure 1. The analysis of the articles, including an overview of the epidemiology study design, types of cancer, and main findings of the articles, is summarised in Table 1.
Results and Discussion
Epidemiological Findings and Risk Factors Associated with C. auris Infection
Over 400,000 bloodstream infections per year have been attributed to Candida spp., which are the most common fungi in hospital settings worldwide (4, 18). C. albicans is the primary pathogen responsible for candidiasis (25). However, C. auris has been reported in over 25 countries on five continents, causing fungemia outbreaks with crude mortality rates varying from 32% to 66% (26–28). Since Candida spp. are highly heterogeneous, C. auris differs markedly from common and well-studied pathogenic Candida spp., such as C. albicans and C. glabrata (29, 30). C. auris can persistently colonise the host skin, making it easily transmissible between patients (24).
C. auris is an opportunistic pathogen that has gained attention due to its ability to cause severe infections and outbreaks in healthcare settings. This yeast can cause life-threatening infections, particularly in individuals with a compromised immune system (30). The risk factors for contracting C. auris infection are similar to those for contracting bloodstream infections (BSIs) (Figure 2). These factors include the use of invasive medical devices, such as central venous or urinary catheters, broad-spectrum antibiotic therapy, prolonged hospitalisations, immunosuppressive therapies, the elderly, and major surgical procedures (31, 32).
Patients with cancer are vulnerable and at a higher risk for C. auris infections due to several factors, including the malignancy itself and the immunosuppressive treatments they undergo. Treatments such as chemotherapy, radiation therapy, and immunosuppressive agents further compromise immune function, thus reducing the ability to overcome infections (4). The ability of C. auris to adhere to medical devices and form biofilms causes its spread and persistence in healthcare settings (6, 33). Biofilms have been found in 90% of catheter-associated infections, indicating the impact that C. auris can have in a hospital setting where catheter infections are the leading cause of morbidity and mortality (21).
A retrospective study emphasises the prevalence of C. auris infections in adult cancer patients, particularly those with cholangiocarcinoma, prostate cancer, multiple myeloma, Hodgkin’s lymphoma, and colorectal carcinoma with metastases (18). The study highlights that C. auris colonisation is common among cancer patients with comorbid conditions, such as diabetes and gastrointestinal or liver diseases (18). The findings emphasise the need to properly screen and monitor C. auris in this vulnerable patient population. Other studies have also discussed the types of cancers associated with C. auris infections, including colorectal, brain, and pancreatic carcinoma (18–23).
Few case reports have shown that patients tend to develop C. auris infection during long-term hospitalisation and with extensive use of broad-spectrum antibiotics (20–22). These cases highlight the increased susceptibility of immunocompromised cancer patients to C. auris infection due to their weakened immune systems and frequent hospitalisations (21). This is due to the characteristics of C. auris, which can colonise multiple body sites, including the axilla, groin, oral cavity, or the bloodstream, as observed in patients with central venous catheters and those undergoing intensive treatments (34). It can colonise hosts within days to weeks of exposure, and invasive infections may occur within days to months of colonisation (30). C. auris is an opportunistic pathogen that inhabits the skin and causes systemic infections in hospital environments, particularly among patients with underlying medical conditions, including those who have contracted COVID-19 (35).
Only one study reported in paediatric patients that C. auris bloodstream infections occurred in children with haematological malignancies (19). The incidence of C. auris bloodstream infections in the paediatric group was due to the susceptibility of paediatric cancer patients to fungal infections. Strict adherence to infection-control protocols, including contact precautions, hand hygiene, and environmental cleaning, is essential to prevent the spread of C. auris in paediatric oncology wards. Healthcare facilities should also consider separating infected patients into separate wards to minimise transmission.
C. auris and Carcinogenesis
Biofilm formation, phenotypic switching, secretion of lytic enzymes, and high-stress tolerance are the virulence factors of C. auris that contribute to nosocomial infection. In addition, C. auris can persistently colonise healthcare environments and human hosts despite the reduced adhesins in its genome (36). However, the role of C. auris in cancer development remains unclear.
Most of the articles examined in this review did not demonstrate a direct link between C. auris and cancer development; rather, cancer patients are more prone to be infected by the species. The true occurrence of C. auris candidemia remains poorly defined due to the failure of conventional methods to identify the species (31). Furthermore, the species has also been reported to be wrongly diagnosed with Candida haemulonii (37). Thus, these findings highlight the importance of accurately detecting C. auris to prevent its spread, particularly among immunocompromised cancer patients.
Regarding the methods of identifying C. auris infection, a study mentioned that the yeast is difficult to identify accurately due to the lack of proper diagnostic tools (19). Some studies emphasised the need for rapid and accurate identification of C. auris to prevent nosocomial infections and outbreaks. Thus, infection-control measures are needed to manage the spread in healthcare settings (19, 21).
Candida spp. including C. auris, have the potential to initiate and promote the progression of cancerous processes; however, they are not considered causative agents of cancer (38–42). Candidiasis can occur due to the existing cancer and can be used to predict the cancer severity. Their development may be favoured by immunosuppression resulting from cancer chemotherapy. Candida infections have been reported to promote cancer progression by affecting the host via various mechanisms (43):
Perturbations in the DNA-damage response in host cells cause genetic mutations that accumulate inside the cell, modifying the oncogene expression involved in cell survival and proliferation.Oncogenic inflammation in the host cells induced by DNA-damaging fungal toxins and their carcinogenic-inducing metabolites.Fungal colonisation or infection results in intense inflammation, favouring the growth of primary tumours and metastases, making tumours resistant to chemotherapy drugs and suppressing the host’s anti-cancer immune responses.
Candida spp. has been reported to be isolated from 75% of individuals diagnosed with oral squamous cell carcinoma (OSCC) (44). The majority of Candida isolates were C. albicans. In addition, oral candidiasis has been observed in patients with haematopoietic neoplasms, head and neck malignancies, and those undergoing chemotherapy or radiotherapy, with a prevalence ranging from 7% to 52%. (45, 46). Animal studies have suggested that infections caused by C. albicans can lead to carcinogenesis, similar to other known carcinogenic substances (10, 47, 48). Several studies have also demonstrated a strong correlation between candidiasis and dysplasia in the oral cavity, precancerous disorders, and OSCC (49, 50).
Candida promotes carcinogenesis by producing carcinogens, pro-carcinogen metabolism, and other molecular mechanisms (51). A study performed on Sprague-Dawley rats found that an imbalance in the oral microbiome can cause Candida hyphal invasion, producing and releasing nitrosamines that can promote the growth and progression of oral cancers (52, 53). These results align with the previous research that reported on the ability of C. albicans to catalyse carcinogenesis in the tongues of rats and mice when exposed to repeated applications of nitroquinoline (4-nitroquinoline1-oxide; 4-NQO), similar to the human head and neck cancer (51). In addition, the upregulation of Ki-67, P53, and COX-2 in host cells following infection with Candida implies the potential role of this fungus in the malignant transformation of host cells (51, 54).
Furthermore, the upregulation of cell proliferation markers (Ki-67 and P53) has been extensively documented in several malignant conditions (48). The expression of COX-2, an inflammatory marker that converts arachidonic acid to prostanoids (including prostaglandins, thromboxane, and prostacyclin), has been observed in various cancers and precancerous abnormalities, indicating its potential role in promoting cell growth, tumour invasion, and cell death (48). Even though the evidence indicating a direct link of C. auris to carcinogenesis is still limited, however, the evidence on the role of Candida in cancer development may hypothesise a similar pathway for this emerging fungal pathogen toward cancer initiation and progression (48, 55, 56).
Conclusion
Although evidence directly linking C. auris to cancer development is currently lacking, the increased susceptibility of cancer patients to C. auris infections may indicate the link to cancer initiation and progression. This evidence also emphasises the need for enhanced and improved treatment of C. auris infection in cancer patients. Nevertheless, further research is essential to elucidate the mechanisms of C. auris and its impact on cancer progression. By addressing these challenges, healthcare providers can better manage C. auris infections and improve outcomes for cancer patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO Antimicrobial Resistance Division (AMR) WHO fungal priority pathogens list to guide research, development and public health action [Internet]Geneva World Health Organization 2022[Retrieved 2024 Aug 12]. Available at: https://www.who.int/publications/i/item/9789240060241
- 2Satoh K Makimura K Hasumi Y Nishiyama Y Uchida K Yamaguchi H Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital Microbiol Immunol 2009531414410.1111/j.1348-0421.2008.00083.x 19161556 · doi ↗ · pubmed ↗
- 3Mohd Tap R Lim TC Kamarudin NA Ginsapu SJ Abd Razak MF Ahmad NA fatal case of Candida auris and Candida tropicalis candidemia in neutropenic patient Mycopathologia 2018183355956410.1007/s 11046-018-0244-y 29383574 PMC 5958168 · doi ↗ · pubmed ↗
- 4Cortegiani A Misseri G Chowdhary A What’s new on emerging resistant Candida species Intensive Care Med 201945451251510.1007/s 00134-018-5363-x 30191295 · doi ↗ · pubmed ↗
- 5Pallotta F Viale P Barchiesi F Candida auris: the new fungal threat Infez Med 202331332332810.53854/liim-3102-1237701386 PMC 10495051 · doi ↗ · pubmed ↗
- 6Lone SA Ahmad A Candida auris—the growing menace to global health Mycoses 201962862063710.1111/myc.1290430773703 · doi ↗ · pubmed ↗
- 7Bravo Ruiz G Lorenz A What do we know about the biology of the emerging fungal pathogen of humans Candida auris?Microbiol Res 202124212662110.1016/j.micres.2020.12662133096325 · doi ↗ · pubmed ↗
- 8Bray F Ferlay J Soerjomataram I Siegel RL Torre LA Jemal A Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin 201868639442410.3322/caac.2149230207593 · doi ↗ · pubmed ↗