Healthcare workers’ attitudes and factors affecting provision of sexual and reproductive health services to adolescents in refugee settlements, Western Uganda
Simon Binezero Mambo, Moazzam Mohiuddin Lodhi, Isa Asiimwe, Gloria Neema Bizimana, Amos M’yisa Makelele, Solomom Adomi Mbina, Mathew Chibunna Igwe, Umar Ibrahim

TL;DR
The study examines healthcare workers' attitudes and factors influencing the provision of sexual and reproductive health services to adolescents in refugee settlements in Uganda.
Contribution
The study identifies key factors like residence, designation, and facility type that influence service provision attitudes among healthcare workers in refugee settings.
Findings
Healthcare workers showed good attitudes toward comprehensive sexuality education and antenatal care but poor attitudes toward safe abortion care.
Government facilities were more likely to offer adolescent sexual and reproductive health services compared to private facilities.
Training is recommended to improve knowledge and attitudes, especially among older professionals and non-counselors.
Abstract
Provision of sexual and reproductive health services has an important impact on the adolescents standard of life. Healthcare workers interactions with clients has been highlighted as one of the main barriers keeping adolescents from seeking sexual and reproductive health services. This study aimed to assess the Healthcare workers’ attitudes and factors affecting provision of sexual and reproductive health services in the Nakivale, Kyaka II, and Rwamwanja refugee settlements. This was a cross-sectional quantitative study in which healthcare workers from public and private health facilities refugee communities in south-western Uganda responded to a questionnaire. Binary logistic regression was done to assess the baseline characteristics associated with provision of these services using SPSS version 26. Of the 386 medical professionals enrolled, 194(50.3%) were females with a mean age of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
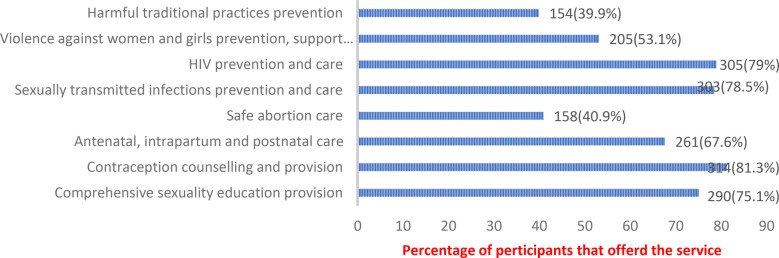 Figure 1
Figure 1| ASRH services | Comprehensive sexuality education provision | Contraception counselling & provision | Antenatal, intrapartum and postnatal care | Safe abortion care | STI prevention and care | HIV prevention and care | Violence against females prevention and care | Harmful traditional practices prevention |
|---|---|---|---|---|---|---|---|---|
| Attitude | Percentage of participants who checked response | |||||||
| They are careless | 19.4 | 19.9 | 17.4 | 23.8 | 19.9 | 16.3 | 14.0 | |
| They have no morals | 21.8 | 22.3 | 17.4 | 20.7 | 17.6 | 14.8 | 17.1 | |
| They were poorly brought up | 29.5 | 23.8 | 22.0 | 18.1 | 16.6 | 19.7 | 19.7 | |
| They will be punished by God | 18.7 | 16.8 | 13.5 | 16.1 | 13.5 | 12.4 | 13.2 | |
| They are irresponsible | 22.8 | 20.7 | 13.7 | 21.0 | 14.8 | 13.0 | 14.5 | |
| They are stupid | 14.2 | 12.7 | 12.2 | 12.2 | 14.0 | 13.0 | 13.0 | |
| They need to be helped | ||||||||
| They need to be educated | ||||||||
| I don't want to help them | 13.2 | 15.5 | 14.0 | 14.0 | 16.1 | 16.1 | 13.7 | |
| Mistakes are part of Life | 21.0 | 19.2 | 15.5 | 21.5 | 16.6 | 20.2 | 16.6 | |
| Others | 1.6 | 2.3 | 1.8 | 2.6 | 1.8 | 1.0 | 1.0 | |
| ASRH services | Comprehensive sexuality education provision | Contraception counselling & provision | Antenatal, intrapartum and postnatal care | Safe abortion care | STI prevention and care | HIV prevention and care | Violence against females prevention and care | Harmful traditional practices prevention |
|---|---|---|---|---|---|---|---|---|
| Factor/reason | Percentage of participants who checked response | |||||||
| Inadequate training | ||||||||
| Contradiction with my values | 26.9 | 24.6 | 18.4 | 28.5 | 18.4 | 15.8 | 21.8 | 22.0 |
| Contradiction with my beliefs | 25.6 | 24.4 | 18.7 | 19.9 | 18.4 | 16.3 | 23.3 | |
| Contradiction with my culture | 22.3 | 25.9 | 20.7 | 18.9 | 17.4 | 20.2 | 23.3 | |
| Contradiction with faith/religion | 25.6 | 32.6 | 18.1 | 17.9 | 23.1 | 22.8 | 25.1 | |
| Services are not available | 24.6 | 30.1 | 21.5 | 31.6 | 18.9 | 26.4 | 26.7 | 31.3 |
| Services are expensive | 26.7 | 25.9 | 37.0 | 28.0 | 28.2 | 27.7 | 23.6 | 21.2 |
| No time to offer the services | 17.4 | 11.1 | 8.3 | 8.0 | 7.3 | 9.3 | 16.1 | 15.3 |
| I will be imprisoned | 2.8 | 1.3 | 7.3 | 2.6 | 3.6 | 5.2 | 4.1 | |
| Others | 2.8 | 5.4 | 4.4 | 3.1 | 5.7 | 7.0 | 4.4 | |
| Characteristic | Bivariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| cOR | 95% CI | aOR | 95% CI | |||
| Age | ||||||
| 19–30 | 1.008 | 0.974–1.043 | 0.636 | |||
| Above 30years | Ref. | |||||
| Sex | ||||||
| Male | Ref | |||||
| Female | 1.072 | 0.675–1.700 | 0.769 | |||
| Residence | ||||||
| Rural |
|
| ||||
| Urban | Ref | |||||
| Education | ||||||
| Primary | 0.452 | 0.036–5.707 | 0.539 | |||
| Secondary | 0.516 | 0.154–1.729 | 0.284 | |||
| Certificate | 0.653 | 0.270–1.583 | 0.346 | |||
| Diploma | 0.697 | 0.282–1.727 | 0.436 | |||
| Degree | Ref | |||||
| Designation | ||||||
| Counselor | Ref | |||||
| Nurse |
|
| ||||
| Clinical officer | 0.329 | 0.104–1.046 | 0.060 | 0.338 | 0.104–1.102 | 0.072 |
| Lab technician | 0.412 | 0.090–1.881 | 0.252 | 0.371 | 0.080–1.729 | 0.207 |
| Doctor | 1.882 | 0.194–18.228 | 0.585 | 1.564 | 0.159–15.394 | 0.701 |
| Other | 0.275 | 0.050–1.508 | 0.137 | 0.156 | 0.026–0.922 | 0.040 |
| Religion | ||||||
| Anglican | 0.689 | 0.372–1.276 | 0.236 | |||
| Catholic | 0.793 | 0.429–1.468 | 0.461 | |||
| Muslim | 3.080 | 0.669–14.171 | 0.249 | |||
| Other | Ref | |||||
| Type of facility | ||||||
| Government |
|
| ||||
| Private | Ref | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent Sexual and Reproductive Health · Migration, Health and Trauma · Poverty, Education, and Child Welfare
Introduction
Globally there are about 1.3 billion of adolescents, between the ages of 10 and 19 years, nine out of 10 people in this age-group live in less developed countries (1, 2). Adolescent sexual and reproductive health (ASRH) care needs are rising in both low and middle-income countries, especially for young women and marginalized groups such as refugees, faces unique challenges, including long waiting times at health facilities, lack of privacy, mistreatment and general poor quality of services (3). Such factors deter these patients from using health services, ultimately placing them at risk for negative SRH outcomes, including HIV infection, unintended pregnancy and unsafe abortion (4). In Uganda, more than 30% of the total population is aged 10–24 years, making it one of the youngest countries in the world, with 1,252,470 refugees and asylum seekers, Uganda is the third refugee-hosting nation in the world after Ethiopia and Kenya (5). Uganda's approach to refugee management is recognized as one of the most progressive in the world. The Office of the Prime Minister (OPM), specifically the Department of Refugees, plays a central role in refugee management, have put in place a system that ensures refugees living in settlements have access to healthcare services and facilities per Ministry of Health guidelines (5, 6).
Humanitarian settings in Uganda are associated with high prevalence of gender based violence (GBV) which is a risk factor for poor ASRH outcomes (7). In Uganda, ASRH services such as HIV and AIDS, and contraceptive use are often neglected, moreover, access and availability to ASRH is limited due to social and structural factors and over-bur dened health systems within humanitarian settlements lack of respect for adolescents' privacy and confidentiality, and the ill treatment by healthcare workers are some of the reported negative behaviors that discouraged sexually active adolescents from seeking SRH services (7, 8). Healthcare workers interactions with clients has been highlighted as one of the main barriers keeping adolescents from seeking SRH services (8). In humanitarian settings, international recommendations emphasize giving priority to the provision of SRH information and services (9). Adolescent girls continue to have poor understanding of and access to SRH services in humanitarian situations like the Nakivale settlement (3–10).
Provision of sexual and reproductive health services has an important impact on the adolescents standard of life (11). These services must be available, and staff qualities like competence, secrecy, and provider privacy, as well as attitudes, play a significant role in how often people use them (8–12). Settlements of refugees are highly susceptible to problems with sexual and reproductive health (13). The study give insight about health care workers' attitudes toward adolescent sexual and reproductive health in humanitarian settings could be helpful in designing appropriate intervention measures to improve adolescent sexual and reproductive health in the settlements.
Methods
Study design and setting
We conducted a cross-sectional survey in 3 refugee settlements of the south-western Uganda, specifically Nakivale, Kyaka II and Rwamwanja. All 3 settlements had one health Centre IV government-led facility and privately owned facilities. Healthcare workers of the different cadres, Doctors, Clinical officers, nurses, midwives and counselors both from Public and private facilities were enrolled into the study.
Sample size and sampling
Kish and Leslie formula was used to identify the necessary minimum sample size. n = z^2^(pq)/e^2^. Since no quantitative study had been done in Uganda on the subject, 50% was used for the proportion. Therefore P = 0.5, q = 0.5, e = 0.05 and z = 1.96. On substituting, n = 385.1 = 386. Therefore, a minimum of 386 participants was required.
All health workers that agreed to participate in the research were enrolled after signing an informed consent document until the sample size was attained.
Data collection procedure
Data were collected using a self-administered structured questionnaire provided to respondents at their respective health institutions. The questionnaire was adapted from Tilahun et al. (13) and pretested on a convenience sample of 20 health workers that were not included in the study and corrections were made afterwards. The sociodemographic characteristics of the healthcare provider (age, sex, tribe, religion, place of residence, level of education, and marital status) as well as the attitude of the healthcare provider (positive (supportive, understanding) or negative (judgmental, stigmatizing, abusive, stereotyping) were the independent variables. Factors connected to health facilities (availability of services and availability of staff) were the intervening variables. Provision of the SRH services was the dependent variable.
The participant were consecutively selected in the health facilities for the 3 settlements, they gave information on the sexual and reproductive health services offered to the adolescents. The participants also responded to the questions relating to their attitude toward provision of each of the services. The questions relating to factors affecting provision of sexual and reproductive health services were also responded to. Data collection took place from August to October, 2023.
Statistical analysis
Information was summarized in excel and entered into SPSS version 26 for analysis. The proportion of health workers providing specific services was computed. The proportion of health workers with a specific attitude category was computed. The proportion of factors reported by health workers to affect provision of sexual and reproductive services to adolescents was computed. To measures attitude and Factors affecting provision of services, Compute descriptive statistics were done with the Percentage of participants who checked response the to facilitate interpretation and comparison. Bivariate analysis was done for the study participants' characteristics against provision of specific adolescent sexual and reproductive health care services. Variables with p-value below 0.2 at bivariate were re analyzed at multivariate using binary logistic regression to determine health worker related factors significantly affecting provision of sexual and reproductive health care services. P-value less or equal to 0.05 was regarded as significant.
Ethical clearance
The Instituttional Research Ethics Review Committee of Bishop Stuart University approved the protocol with the number BSU REC 2023–203 and authorization to collect data from Refugee settlements was granted by Office of the Prime Minister refugee department were granted with the reference No OPM/41/1. The healthcare workers were provided information about the study and its importance, and confidentiality of the information requested. Written consent was then obtained. from participants in a form provided with the study questionnaire.
Results
Baseline characteristics of the study participants
In this study that enrolled 386 medical professionals, majority were females 194(50.3%) with a mean age of 30.9 years (SD = 6.9), from rural areas 335(86.8%). Majority were nurses 227(58.8%), certificate holders 183(47.4%) from private health facilities 279(72.3%).
The services provided are shown in Figure 1. The service that was most commonly offered was contraception counselling and provision offered by 81.3% of the participants, followed by HIV prevention and care (79.0%), sexually transmitted infections prevention and care (78.5%) and comprehensive sexuality education provision (75.1%). The least offered services were safe abortion care offered by only 40.9% of the study participants and harmful traditional practices prevention offered by only 39.9% of the participants.
Adolescent sexual and reproductive health services offered by healthcare professionals in the refugee camps of Nakivale, Kyaka II, and Rwamwanja.
Table 1: provides information about the majority of the study participants had a good attitude regarding offering services for adolescent sexual and reproductive health as evidenced by their responses on the questions regarding attitude. Majority responded that “adolescents need to be helped” and “adolescents need to be educated”. The good attitudes were highest towards comprehensive sexuality education provision and antenatal, intrapartum and postnatal care with about 80% of the participants reporting that adolescents that need these services need to be helped and educated. The bad attitudes were highest toward safe abortion care with 21.8% of the participants reporting that “they don’t want to help adolescents who need safe abortion care”.
Table 2: Provides information on the main factor that hindered delivery of adolescent sexual and reproductive health services that cut across all services was inadequate training with up to 62.7% of the participants reporting that they had inadequate training regarding harmful traditional practices prevention. Compared to other services, safe abortion care was more hindered by contradiction with beliefs of medical professionals reported by 32.6% of the study participants, contradiction with culture of medical professionals (31.6%), contradiction with faith/religion of medical professionals (43.8%) and fear of imprisonment (19.4%). Compared to other services, violence against women and girls prevention was more hindered by “other” factors which were not explored in this study (41.7%).
Table 3: Both bivariate and multivariable analyses were conducted regarding the association between baseline characteristics and adolescent sexual and reproductive health services.The study showed that residence, designation of medical professional and type of health facility had a statistically significant association with offering of the different adolescent SRH services (P < 0.05 at multivariate level of analysis). Being from rural area was positely associated with ASRH services (cOR = 2.685, 95% CI = 1.414–5.098). Being a nurse was associated with reduced provision of services as compared to being a counselor (cOR = 0.295, 95% CI = 099–0.882). Government facilities were more likely to offer adolescent sexual and reproductive health services compared to private facilities (cOR = 2.155, 95% CI = 1.169–4.075).
Discussion
This study assessed the healthcare workers attitudes and practices in addition to the factors affecting adolescent sexual and reproductive health care in the Nakivale, Kyaka II, and Rwamwanja refugee settlements. The study enrolled 386 medical professionals, majority were nurses, from private health facilities. We noted that the service that was most commonly offered was contraception counselling and provision, followed by HIV prevention and care, sexually transmitted infections prevention and comprehensive sexuality education provision. The least offered services were safe abortion care and harmful traditional practices prevention. In agreement with our findings, a systematic analysis of the data on adolescent sexual and reproductive health services discovered that the majority of services offered in refugee populations focused on HIV/STIs and maternal and newborn health (14). The review found that services like prevention of Harmful traditional practices, provision of safe abortion and post-abortion care were not commonly offered (14). The services like contraception counselling/provision, HIV prevention/care, sexually transmitted infections prevention and comprehensive sexuality education provision were part of the care packages for all patients irrespective of the age which can explain why they were the most commonly offered. The possible reason for low safe abortion care is the controversy that surrounds abortion in terms of the country laws as well as the beliefs and norms of the different communities. The low harmful traditional practices prevention services female genital mutilation are most likely as a result of inadequate knowledge and cultural practices in refugees community.
Contrally to our findings, a systematic analysis of the data on adolescent sexual and reproductive health services discovered that the majority of services offered in refugee populations focused on gender-based violence (14, 15), yet in our study only about 53% of the respondents offered services relating to violence against women and girls. This low provision of such services could be because of low knowledge however, about 41% of the participants reported that there were other challenges which affected these services that were not explored in this study.
In this study, majority of the study participants had a good attitude regarding offering services for adolescent sexual and reproductive health. The good attitudes were highest towards comprehensive sexuality education provision and antenatal, intrapartum and postnatal care while the bad attitudes were highest toward safe abortion care. The fact that antenatal, intrapartum and postnatal care is part of routine care offered to all patients could have contributed to the good attitudes. In agreement with our findings, in a South African study, nurses said they had trouble understanding and implementing the notion of abortion (16). They clarified that their traditional ideas and values were in conflict with this practice, which resulted in a negative attitude toward the adolescents who came in need of this assistance (16).Non-marital sex and its repercussions, such as pregnancy, abortion, and sexually transmitted illnesses, were noted to be viewed as immoral, disrespectful, and disobedient in Ghana (17), which is similar to many cultures in Uganda and across Africa.
We also observed that the main factor that hindered delivery of adolescent sexual and reproductive health services that cut across was inadequate training. In agreement with our findings, lack of knowledge of SRH, was one of the main obstacles preventing the use of SRH in Ethiopia (18). Compared to other services, safe abortion care was more hindered by contradiction with beliefs of medical professionals, contradiction with culture, contradiction with faith/religion and fear of imprisonment. In agreement with this, negative cultural attitudes was one of the main barriers blocking young people in the Lao People's Democratic Republic from utilizing sexual and reproductive health services (3). Also a thorough investigation focusing on Africa reported that one of the main limiting factors was stigma (19).
Increasing age of the medical professional was associated with less contraception counselling and provision which was in agreement with a study done in Nigeria where access to sexual and reproductive health care was shown to be substantially correlated with age (20). This may be because older people are more likely to have stronger beliefs in culture and tradition as compared to younger people.
Rural residence was associated with increased provision of majority of the services. This was in agreement with findings by (18) in Ethiopia who reported that area of residence was substantially linked with the application of sexual and reproductive health services. This could be because in urban areas, patients are more likely to seek care from private facilities, which brings in the issue of costs as was seen in Congo, where Urban participants brought up costs as the hindrance to these services (21)
Being a nurse or doctor was associated with reduced provision of services as compared to being a counselor, Doctors and nurses focus on physical health: diagnosing and treating illnesses, providing vaccinations, managing injuries, and ensuring basic medical care while Counselors their strength lies in providing psychosocial support, education, addressing trauma and other psychological needs for adolescents (22). Also lower education level was associated with less contraception counselling and provision. In Nigeria access to sexual and reproductive health care was shown to be substantially correlated with education (23) This association could be arising as a result of knowledge about the subject. Counselors were more likely to offer these services possibly because they learn to understand every person and to avoid being judgmental which could have improved their attitude towards provision of these services.
Government facilities were more likely to offer adolescent sexual and reproductive health services compared to private facilities. A thorough investigation focusing on Africa reported that one of the main limiting factor was cost (3). Since government facilities offer these services for free, it is understandable that they were more likely to offer these services. Also private facilities are aimed at maximizing profit which could explain why they would provide less of these services given that most of the adolescents may not have the funds to cater for these services even when they need them. This could be because they fear to get money from their parents or guardians for such services in fear of judgment or punishment.
Strength and limitations
This was the first multicentre study in Uganda that assessed the healthcare workers' attitudes and factors affecting provision of sexual and reproductive health services to adolescents in refugee settlements of western Uganda.
This was a cross sectional study in which conclusions about causation could not be made. Compared to other services, violence against women and girls prevention was more hindered by “other” factors which were not explored in this study.
Conclusion
In this study, majority of the study participants had a good attitude regarding offering services for adolescent sexual and reproductive health. The good attitudes were highest towards comprehensive sexuality education provision and antenatal, intrapartum and postnatal care while the bad attitudes were highest toward safe abortion care. The services that was most commonly offered were contraception counselling and provision, HIV prevention and care, sexually transmitted infections prevention and comprehensive sexuality education provision. The least offered services were safe abortion care and harmful traditional practices prevention. The main factor that hindered delivery of adolescent sexual and reproductive health services that cut across all services was inadequate training. Residence, designation of medical professional and type of health facility had a statistically significant association with offering of the different adolescent sexual and reproductive health services. More efforts are still required toward provision of safe abortion care and harmful traditional practices prevention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Berhane Y Canavan CR Darling AM Sudfeld CR Vuai S Adanu R The age of opportunity: prevalence of key risk factors among adolescents 10–19 years of age in nine communities in sub-Saharan Africa. Trop Med Int Health. (2020) 25(1):15–32. 10.1111/tmi.1333931698531 · doi ↗ · pubmed ↗
- 2Adolescent health - World Health Organization (WHO) Available at: https://www.who.int/health-topics/adolescent-health/#tab=tab_1 (Accessed September 07, 2024).
- 3Ivanova O Rai M Kemigisha E. A systematic review of sexual and reproductive health knowledge, experiences and access to services among refugee, migrant and displaced girls and young women in Africa. Int J Environ Res Public Health. (2018) 15(8):1583. 10.3390/ijerph 1508158330049940 PMC 6121882 · doi ↗ · pubmed ↗
- 4Folayan MO Sam-Agudu NA Harrison A. Exploring the why: risk factors for HIV and barriers to sexual and reproductive health service access among adolescents in Nigeria. BMC Health Serv Res. (2022) 22(1):1198. 10.1186/s 12913-022-08551-936151543 PMC 9508705 · doi ↗ · pubmed ↗
- 5Komuhangi H. The contribution of UNHCR and refugee welfare in Uganda (Doctoral dissertation, Kampala International University, College of Humanities and Social Sciences). (2018).
- 6Muhatia M. An Assessment of the Monitoring and Evaluation System For the Refugee Settlement Programme in Uganda (Doctoral dissertation, University of Nairobi). (2023).
- 7Bukuluki P Kisaakye P Mwenyango H Palattiyil G. Adolescent sexual behaviour in a refugee setting in Uganda. Reprod Health. (2021) 18(1):131. 10.1186/s 12978-021-01181-034167555 PMC 8222959 · doi ↗ · pubmed ↗
- 8Jonas K Crutzen R Krumeich A Roman Nvan den Borne B Reddy P. Healthcare workers’ beliefs, motivations and behaviours affecting adequate provision of sexual and reproductive healthcare services to adolescents in Cape Town, South Africa: a qualitative study. BMC Health Serv Res. (2018) 18:1–13. 10.1186/s 12913-018-2917-029433499 PMC 5810035 · doi ↗ · pubmed ↗