Can Calcaneofibular Ligament Repair Correct Hindfoot Varus Alignment in the Management of Chronic Lateral Ankle Instability?
Kensei Yoshimoto, Mitsuki Kumaki, Takumi Koseki, Ayako Tominaga, Masahiko Noguchi, Ken Okazaki

TL;DR
This study found that repairing both the ATFL and CFL ligaments does not correct hindfoot varus alignment or reduce ankle instability more effectively than repairing only the ATFL.
Contribution
The study provides new evidence that combining CFL and ATFL repair does not improve outcomes in patients with hindfoot varus and chronic ankle instability.
Findings
Neither ATFL-only nor combined ATFL and CFL repair corrected hindfoot varus alignment.
No significant difference in recurrent ankle instability between the two groups.
SAFE-Q scores did not differ significantly between the groups post-surgery.
Abstract
Background: Hindfoot varus alignment is a risk factor for chronic lateral ankle instability (CLAI) and recurrent ankle instability following anterior talofibular ligament (ATFL) repair for CLAI. This study aimed to assess whether combining calcaneofibular ligament (CFL) repair with ATFL repair can correct hindfoot varus alignment and reduce recurrent ankle instability. Methods: This study retrospectively examined 74 ankles from 71 patients with hindfoot varus alignment who had lateral ankle ligament repair for CLAI. Arthroscopic ATFL repair was performed on 37 ankles (from 36 patients) between 2018 and 2021 (ATFL-only group), whereas open ATFL and CFL repair were conducted on another 37 ankles (from 35 patients) between 2021 and 2023 (CFL-repair group). Long axial hindfoot alignment radiographs were utilized to measure tibiocalcaneal angles (TCA) pre- and postoperatively. The primary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
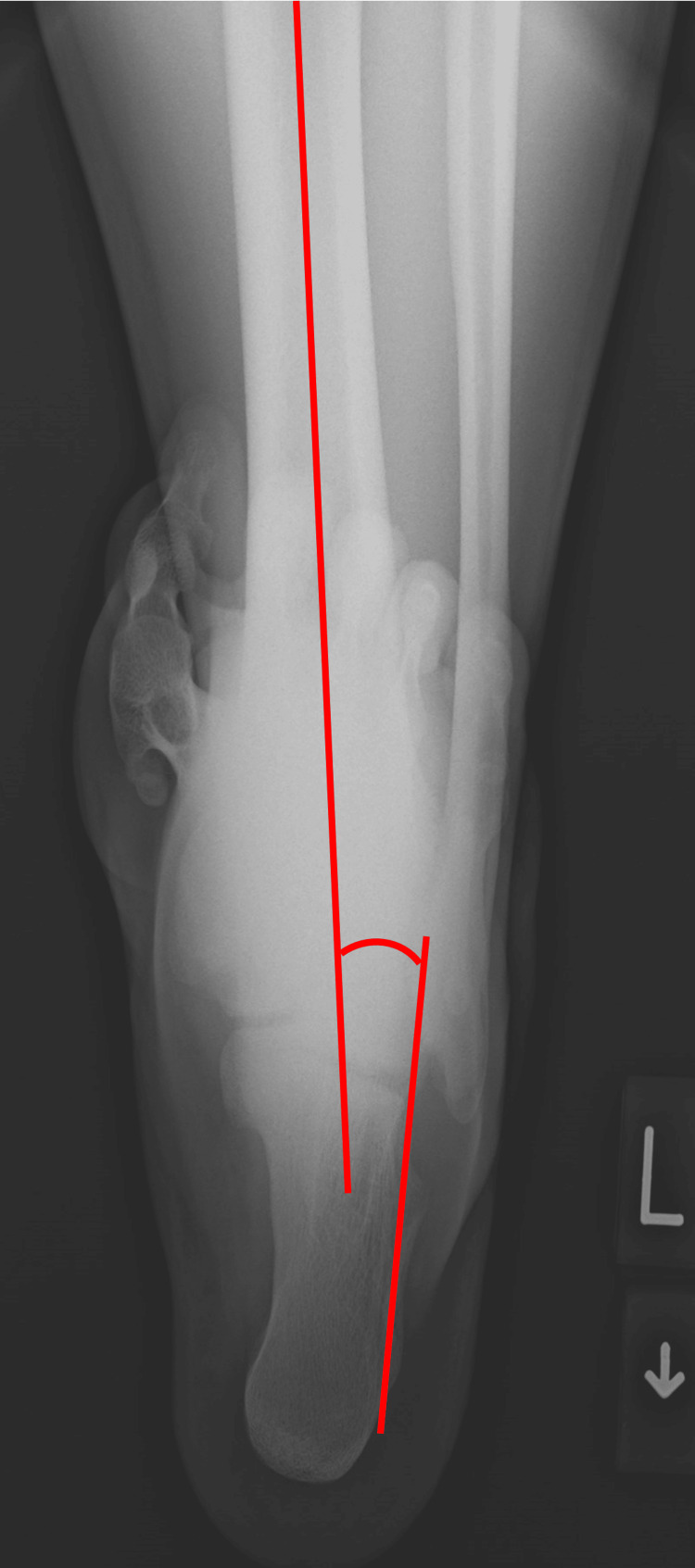 Figure 1
Figure 1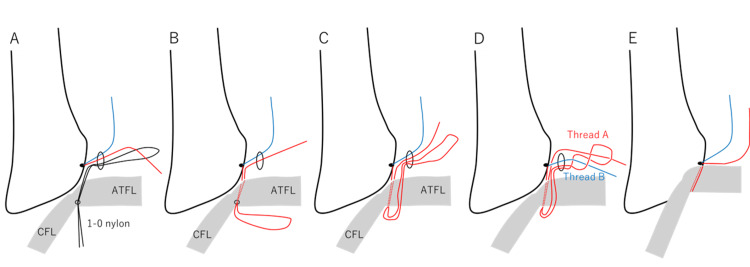 Figure 2
Figure 2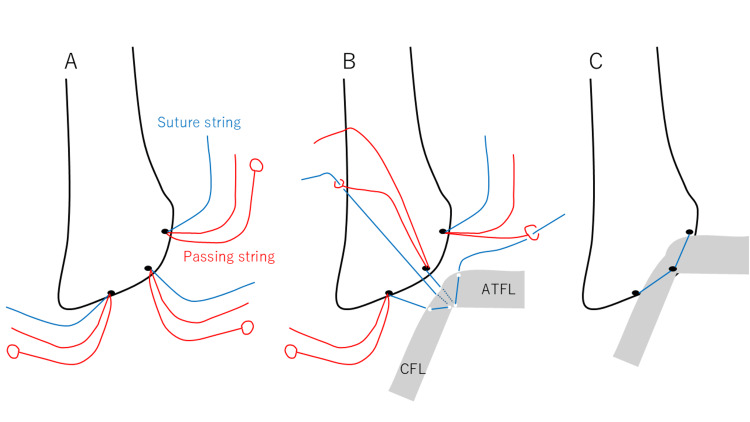 Figure 3
Figure 3| ATFL-only (37 ankles) | CFL repair (37 ankles) | P-value | |
| Age (years) | 38.1 ± 17.1 | 37.5 ± 15.3 | 0.867 |
| Males | 17 (45.9%) | 16 (43.2%) | |
| Females | 20 (54.1%) | 21 (56.8%) | 0.815 |
| BMI (kg/m2) | 23.3 ± 4.0 | 23.9 ± 3.2 | 0.163 |
| Follow-up periods (months) | 22.8 ± 12.8 | 18.8 ± 8.2 | 0.201 |
| Sports participation | 21 (56.8%) | 17 (45.9%) | 0.283 |
| Preoperative SAFE-Q | |||
| Pain related | 66.5 ± 23.5 | 59.0 ± 25.8 | 0.249 |
| Physical functioning | 82.5 ± 19.0 | 81.2 ± 16.5 | 0.436 |
| Social functioning | 77.7 ± 26.5 | 71.0 ± 25.7 | 0.214 |
| Shoe related | 85.4 ± 18.4 | 76.7 ± 26.3 | 0.189 |
| General health | 75.6 ± 20.5 | 69.4 ± 24.8 | 0.324 |
| ATFL-only (37 ankles) | CFL repair (37 ankles) | P-value | |
| Preoperative TCA (degrees) | 5.8 ± 2.8 (95% CI: 4.8 to 6.7) | 5.7 ± 2.9 (95% CI, 4.7 to 6.6) | 0.622 |
| Postoperative TCA (degrees) | 5.6 ± 3.0 (95% CI: 4.6 to 6.6) | 5.6 ± 3.0 (95% CI, 4.6 to 6.6) | 0.869 |
| 95% CI of differences | -0.7 to 0.4 | -0.5 to 0.4 |
| ATFL-only (37 ankles) | CFL repair (37 ankles) | P-value | |
| Recurrent instability (ankles) | 13 (35.1%) | 11 (29.7%) | 0.619 |
| Revision surgery (ankles) | 2 (0.5%) | 0 (0%) | 0.493 |
| Complications (ankles) | 1 (0.3%) | 2 (0.5%) | 1 |
| Postoperative SAFE-Q | |||
| Pain related | 88.8 ± 16.8 | 90.4 ± 13.4 | 0.788 |
| Physical functioning | 95.0 ± 9.9 | 96.3 ± 5.6 | 0.980 |
| Social functioning | 96.4 ± 9.0 | 97.1 ± 4.9 | 0.423 |
| Shoe related | 93.2 ± 12.7 | 88.7 ± 15.6 | 0.283 |
| General health | 94.0 ± 13.9 | 93.7 ± 8.5 | 0.139 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFoot and Ankle Surgery · Tendon Structure and Treatment · Lower Extremity Biomechanics and Pathologies
Introduction
Ankle sprain is a predominant injury that usually heals with conservative treatment. However, approximately 20% of patients experience chronic lateral ankle instability (CLAI)[1]. Repetitive ankle sprain and chronic instability cause degenerative changes if not adequately treated [2]. Surgical intervention is indicated for patients with mechanical instability after nonoperative modality failure.
Only anterior talofibular ligament (ATFL) repair with open or arthroscopic modified Broström procedure for CLAI is a widely accepted procedure with good clinical outcomes [3,4]. However, hindfoot varus alignment is a popular risk factor for CLAI [5] and recurrent ankle instability after ATFL repair [6]. Furthermore, this malalignment results in poor clinical outcomes after arthroscopic ATFL repair [6]. Therefore, hindfoot varus alignment correction is crucial for CLAI [7]. Calcaneus osteotomy is a reliable procedure for hindfoot varus alignment correction [7], but it is more invasive than ligament repair. Conversely, calcaneofibular ligament (CFL) injury could induce subtalar instability [8], causing hindfoot varus alignment. Therefore, CFL repair is envisaged to correct the hindfoot varus alignment. However, no study assessed the effectiveness of CFL repair in hindfoot varus alignment correction and postoperative recurrent ankle instability reduction.
This study aimed to assess whether combining ATFL repair with CFL repair could achieve better correction of hindfoot varus alignment and postoperative ankle instability reduction compared to ATFL repair alone. It was considered valuable to compare these two surgical procedures because a recent study suggested that repairing only the ATFL without addressing the injured CFL results in persistent ankle instability [9]. Further, this study hypothesized that both ATFL and CFL repair could correct hindfoot varus alignment as well as calcaneus osteotomy and reduce postoperative ankle instability.
Materials and methods
Study population and study design
Patient records from 2018 to 2023 were analyzed, during which lateral ankle ligament repair for CLAI was performed on 245 ankles from 235 patients. Of this number, the retrospective study screened 108 ankles from 103 patients who exhibited hindfoot varus alignment. Hindfoot varus alignment is defined as a preoperative tibiocalcaneal angle (TCA) of 2.7 degrees or more (Figure 1), measured on long axial hindfoot alignment radiographs [10], which serves as the cut-off value for recurrent ankle instability after arthroscopic ATFL repair for CLAI [11]. TCA is the most commonly used measurement for hindfoot alignment [12]. The indication for surgery included persistent pain that did not respond to conservative treatment and signs of ankle instability on physical examination [13]. The physical examination for the ankle instability depends on assessing anterior drawer and talar tilt laxity, which were considered pathological when a “nonstop” was observed [13,14].
The tibiocalcaneal angle is the angle between the tibial axis and the calcaneal axis (defined as a line parallel to the lateral calcaneal wall).
This study excluded 34 patients (32 ankles) because of a short (<1 year) follow-up period (18 ankles from 17 patients), ankle osteoarthritis, stage 2 or more following the Takakura classification [15] (nine ankles from eight patients), foot and ankle surgery history (five ankles from five patients), and neuromuscular disorders (two ankles from two patients).
Ultimately, this study included 74 ankles from 71 patients. Of this number, arthroscopic ATFL repair was performed on 37 ankles from 36 patients between 2018 and 2021 (ATFL-only group), whereas open repairs for both the ATFL and CFL were conducted on 37 ankles from 35 patients between 2021 and 2023 (CFL-repair group), due to the high rate of recurrent ankle instability associated with arthroscopic ATFL repair in cases of hindfoot varus alignment [6].
Surgical procedure
A single orthopedic surgeon performed all the surgeries. The surgeon conducted an arthroscopic examination using a 2.7-mm, 30-degree arthroscope. The medial midline portal was used for a viewing portal [16], and the accessory anterolateral (acAL) portal was used for a working portal. Arthroscopic ATFL repair was performed following the previously described procedure [11]. In brief, a suture anchor was placed at the inferior edge of the anteroinferior tibiofibular ligament (AITFL) via the acAL portal [17]. One limb of the suture anchor penetrated the inferior bundle of the ATFL. The ATFL was then reattached to the footprint using the modified lasso loop stitch technique (Figure 2)[16].
Details of arthroscopic ATFL repairAn 18-G hollow needle with a 1–0 nylon thread was inserted through the fibula tip to penetrate the inferior bundle of the anterior talofibular ligament after placing a suture anchor at the inferior edge of the anteroinferior tibiofibular ligament. The nylon loop was retrieved via the accessory anterolateral portal. One limb of the suture anchor was then passed through the nylon loop (A), and the opposite end of the nylon loop was pulled out percutaneously (B). Subcutaneous passage of the suture loop through the accessory anterolateral portal was facilitated (C). The loop was twisted to lead thread B, and the loop was then twisted again to lead thread A (D). Thread A was pulled lightly while thread B was pulled tightly to reattach the footprint of the lateral ankle ligament. Finally, a square knot and a granny knot were made twice with a knot pusher (E).ATFL: anterior talofibular ligament
Open repair of both the ATFL and CFL was performed with a 2 cm-long skin incision along the anterior border of the fibula and centered on the obscure tubercle (OT)[17]. The capsule-ligament complex was incised from just distal to the AITFL attachment to the posterior edge of the CFL, along the anterior border of the lateral malleolus without capsule and ligament separation [18]. DEX Knotless FiberTak® suture anchor (Arthrex, Naples, FL, USA) was then inserted into the superior edge of the ATFL attachment, OT, and the posterior edge of the CFL attachment (Figure 3A). This suture anchor consisted of one suture string and two passing strings, which enabled ligament repair without knots. A suture string that was inserted in the posterior edge of the CFL attachment was threaded CFL and capsule complex and passed into the small circle of a passing string inserted in OT. Afterward, a suture string that was inserted in the OT was threaded ATFL and capsule complex and passed into the small circle of a passing string inserted in the superior edge of the ATFL attachment (Figure 3B). The other passing string was drawn to attach the ATFL and CFL to the lateral malleolus (Figure 3C).
Details of open ATFL and CFL repairDEX Knotless FiberTak® suture anchor (Arthrex, Naples, FL, USA) was inserted into the superior edge of the ATFL attachment, OT, and the posterior edge of the CFL attachment (A). A suture string that was inserted in the posterior edge of the CFL attachment was threaded CFL and capsule complex and passed into the small circle of a passing string inserted in OT. A suture string that was inserted in the OT was threaded ATFL and capsule complex and passed into the small circle of a passing string inserted in the superior edge of the ATFL attachment (B). The other passing string was drawn to attach the ATFL and CFL to the lateral malleolus (Figure 3C).ATFL: anterior talofibular ligament; CFL : calcaneofibular ligament; OT: obscure tubercle
All patients were allowed full weight-bearing from day one postoperatively with cast immobilization (until 2022) or ankle brace (from 2023). Because the maximum stress force on the ATFL is only 11.3 N during the stance phase of gait, rigid cast immobilization was considered unnecessary [19]. The cast was removed for one week postoperatively. An ankle brace was used for five weeks after surgery. The patients performed exercises with a physical therapist after wearing the ankle brace to restore muscle strength and motion range. They were also allowed to resume full sports activities once they demonstrated normal ankle function during sport-specific drills at least 5 weeks after surgery.
Evaluation
Long axial hindfoot alignment radiographs were taken preoperatively and 1 year postoperatively [10]. The TCA, which is the angle between the tibial and calcaneal axes (defined as a line parallel to the lateral calcaneal wall), was measured (Figure 1) [12,20]. The adequate reliability of this measurement has already been demonstrated [6]. Positive TCA values indicate hindfoot varus. Furthermore, the flexibility of hindfoot varus alignment was evaluated by two orthopedic surgeons using the Coleman block test, and the interobserver reproducibility of this test was assessed.
The primary outcome includes recurrent ankle instability. During their latest visit, patients were confirmed if their operated ankle had been resprained postoperatively. Patients who experienced resprain of their operated ankle were diagnosed with recurrent ankle instability [6,11,13]. The Self-Administered Foot Evaluation Questionnaire (SAFE-Q) was used to assess secondary outcomes preoperatively and at the latest visit [21,22].
Statistical analysis
Statistical analysis was conducted with JMP Pro version 17.0 software (SAS Institute, Cary, NC, USA). Differences between the two groups were assessed with Fisher’s exact probability test and the Mann-Whitney U test for categorical and continuous variables, respectively. P-values of less than 0.05 indicated statistical significance.
Results
There were no significant differences in patients’ demographics and preoperative SAFE-Q scores between the two groups (Table 1).
The mean pre- and postoperative TCAs were 5.8 ± 2.8 degrees (95% confidence interval (CI), 4.8 to 6.7) and 5.6 ± 3.0 degrees (95% CI, 4.6 to 6.6) in ATFL-only group and 5.7 ± 2.9 degrees (95% CI, 4.7 to 6.6) and 5.6 ± 3.0 degrees (95% CI, 4.6 to 6.6) in the CFL-repair group, respectively. The 95% CI for the differences between pre- and postoperative TCA was −0.7° to 0.4° in the ATFL-only group and −0.5° to 0.4° in the CFL-repair group, which were similar to the measurement error when the same examiner measured TCA twice (−0.5°−0.4°) (Table 2). The interobserver reproducibility of hindfoot flexibility assessment using the Coleman block test was limited to 0.29.
Further, no marked differences were found in postoperative recurrent ankle instability and SAFE-Q scores between the two groups. Two patients in the ATFL-only group underwent revision surgery for recurrent ankle instability, and no patients in the CFL-repair group underwent revision surgery. Wound infection occurred in one patient in the ATFL-only group and two patients in the CFL-repair group. Other surgical complications, such as nerve injury, vascular injury, and tendon injury, did not occur (Table 3).
*Table 3: Comparison of postoperative outcomes between the two groupsATFL: anterior talofibular ligament; CFL: calcaneofibular ligament; SAFE-Q: The self-administered foot evaluation questionnaireValues are mean ± standard deviation.P <0.05
Discussion
The overarching finding in this study was that combining open repair of both the ATFL and CFL did not achieve better correction of the hindfoot varus alignment or a lower rate of recurrent ankle instability compared to ATFL-only repair. To the best of our knowledge, this is the first study that assessed whether repair of both the ATFL and CFL for CLAI could correct hindfoot varus alignment.
Hindfoot varus alignment increases the ankle varus moment during weight-bearing, which promotes stress on the lateral ankle ligament [5]. In particular, CFL injury causes subtalar instability [8] and may induce hindfoot varus alignment. Therefore, it was hypothesized that CFL repair corrects hindfoot varus alignment; however, this hypothesis was not supported. Several reasons may explain why CFL repair could not correct hindfoot varus alignment in this study. First, the effect of the interosseous talocalcaneal and cervical ligaments that work together to stabilize the subtalar joint [23,24] was not considered. Second, CFL repair could not correct rigid hindfoot varus alignment. However, the flexibility of hindfoot varus alignment in this study was unclear. The interobserver reproducibility of hindfoot flexibility assessment using the Coleman block test was limited to 0.29 in this study, likely because the patients had slight hindfoot varus, making accurate evaluation difficult. Third, hindfoot varus deformity was not solely due to ligament-related instability but also resulted from various bone and joint deformities in the foot and ankle.
Long-term follow-up studies of ATFL repair without CFL repair demonstrated good clinical outcomes [25], but an increasing number of articles have focused on the importance of CFL. A biomechanical study observed persistent ankle instability only when the ATFL was repaired without addressing the injured CFL [9], and only ATFL repair without addressing the injured CFL did not correct a normal strain pattern of the CFL [26]. Furthermore, repairing only the ATFL while neglecting a CFL injury may cause recurrent instability [27]. However, the present study could not demonstrate the effectiveness of CFL repair for hindfoot varus alignment. This result was attributed to the residual hindfoot varus alignment after CFL repair.
Hindfoot varus alignment is a popular risk factor for CLAI [5] and recurrent ankle instability after ATFL repair [6]. CFL repair could not correct hindfoot varus alignment; thus, surgeons should consider calcaneal osteotomy if the surgery is aimed at correcting hindfoot varus alignment [7]. However, this study showed good SAFE-Q scores regardless of residual hindfoot varus alignment. Therefore, calcaneal osteotomy might not be necessary for primary surgery but could be required for revision surgery. Moreover, because this study could not determine the cut-off value of TCA to require calcaneus osteotomy, further investigation was needed.
This research has several limitations. First, stress radiography was not assessed. This procedure was deemed unnecessary to evaluate the laxity of CLAI because of its high false-negative rate [28] and because most surgeons do not commonly depend on it [29]. Second, the condition of the lateral ankle ligaments was not assessed. The evaluation of CFL injuries is particularly important because this study primarily aimed to evaluate the effectiveness of CFL repair. However, accurate diagnostic methods and classification of chronic CFL injuries have not been established [30]. If CFL repair was performed based on an accurate diagnosis of CFL injury, different outcomes might be observed. Third, hindfoot flexibility could not be evaluated, as the patients in this study had slight hindfoot varus, making it very difficult to assess hindfoot flexibility using the Coleman block test. Fourth, this study had a relatively small case series. Additional power may have affected the statistical significance of our outcome variables. Furthermore, this study only recorded short-term outcomes. Longer follow-up periods were necessary to assess long-term functional and degenerative outcomes.
Conclusions
The effectiveness of combining ATFL and CFL repair for CLAI with hindfoot varus alignment was assessed. Combining ATFL and CFL repair could not correct hindfoot varus alignment, and this procedure for CLAI with hindfoot varus alignment was not more effective in reducing recurrent ankle instability than ATFL repair alone. These results indicated that surgeons should consider calcaneus osteotomy to correct hindfoot varus alignment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical outcomes of open versus arthroscopic Broström procedure for lateral ankle instability: A meta-analysis J Foot Ankle Surg Moorthy V Sayampanathan AA Yeo NE Tay KS 577584602021 https://doi.org/10.1053/j.jfas.2020.10.001.3350971210.1053/j.jfas.2020.10.001 · doi ↗ · pubmed ↗
- 2The relationship between calcaneofibular ligament injury and ankle osteoarthritis progression: A comprehensive analysis of stress distribution and osteophyte formation in the subtalar joint Foot Ankle Int Sakurai S Nakasa T Ikuta Y 870878452024 https://doi.org/10.1177/10711007241245363.3864720510.1177/10711007241245363 · doi ↗ · pubmed ↗
- 3Open Broström-Gould repair vs arthroscopic anatomical repair of the anterior talofibular ligament for chronic lateral ankle instability Foot Ankle Int Zeng G Hu X Liu W Qiu X Yang T Li C Song W 4449412020 https://doi.org/10.1177/1071100719875964.3153556310.1177/1071100719875964 · doi ↗ · pubmed ↗
- 4Twenty-six-year results after Broström procedure for chronic lateral ankle instability Am J Sports Med Bell SJ Mologne TS Sitler DF Cox JS 9759783420061639993510.1177/0363546505282616 · doi ↗ · pubmed ↗
- 5Relationship between chronic lateral ankle instability and hindfoot varus using weight-bearing cone beam computed tomography Foot Ankle Int Lintz F Bernasconi A Baschet L Fernando C Mehdi N de Cesar Netto C 11751181402019 https://doi.org/10.1177/1071100719858309.3125304510.1177/1071100719858309 · doi ↗ · pubmed ↗
- 6Hindfoot alignment and ankle stability following arthroscopic lateral ankle ligament repair Foot Ankle Int Yoshimoto K Noguchi M Maruki H Tominaga A Okazaki K 8728784420233739199710.1177/10711007231181123 · doi ↗ · pubmed ↗
- 7Idiopathic cavovarus and lateral ankle instability: Recognition and treatment implications relating to ankle arthritis Foot Ankle Int Fortin PT Guettler J Manoli A 2nd 10311037232002 https://doi.org/10.1177/107110070202301111.1244940910.1177/107110070202301111 · doi ↗ · pubmed ↗
- 8Subtalar arthrography in recurrent instability of the ankle Clin Orthop Relat Res Sugimoto K Takakura Y Samoto N Nakayama S Tanaka Y 169176394200210.1097/00003086-200201000-0002011795729 · doi ↗ · pubmed ↗