Bilateral Mandibular Condylar Fractures
Koji Tajima

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
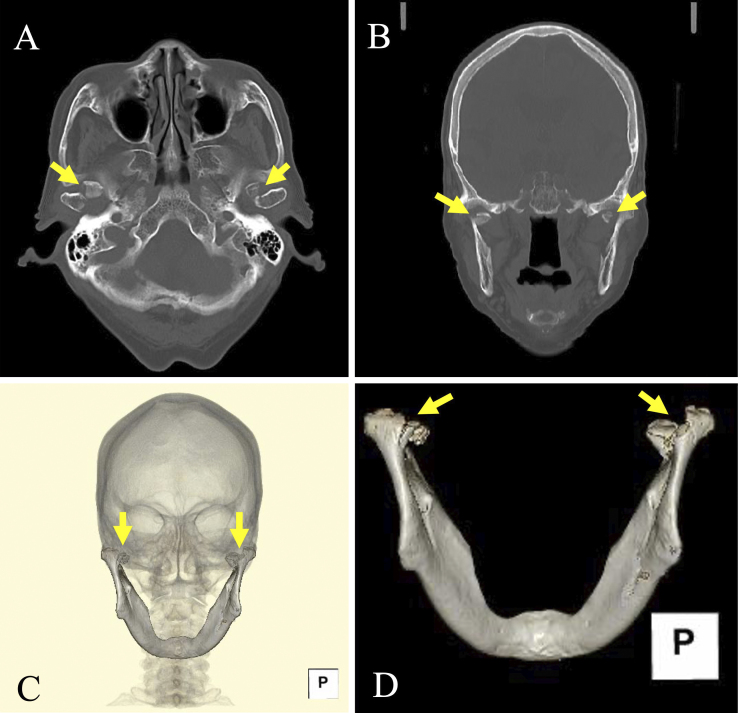 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Trauma and Fracture Management · Facial Nerve Paralysis Treatment and Research · Temporomandibular Joint Disorders
A 95-year-old woman presented with facial injuries after a fall from her car. Her denture was broken. Lacerations on her chin and lower lip were identified and sutured.
Subsequently, the patient reported pain around the right temporomandibular joint. Although there was no wound, mild tenderness was noted at the joint, with no restriction in mouth opening. Computed tomography revealed bilateral mandibular condylar fractures (MCFs) (Figure 1).
Kannari et al. ^(1)^ reported that 20% of mandibular fractures were undiagnosed at the first healthcare visit, with an average delay of 11.3 days to diagnosis. Pain is the most common symptom of MCF, reported in 78.5% of cases ^(1)^.
Limited mouth opening was observed in 43.0% of patients with mandibular fractures ^(1)^. Pain during mouth opening can also contribute to restricted movement ^(2)^.
In patients who are edentulous, the interridge distance between the upper and lower gums should be measured. However, this measurement may be overestimated owing to the absence of incisors compared with patients who are dentulous. The cut-off value for the limitation of mouth opening is 35 mm in patients who are dentulous and 40 mm in those who are edentulous ^(3)^.
In this case, the broken denture suggested that significant pressure was exerted on the mandible. Even when symptoms are subtle, imaging studies should be performed if strong force has been applied. Evaluating facial X-rays for fractures can be challenging for primary care clinicians; therefore, computed tomography should be considered during the initial consultation.
Clinicians should, therefore, attend to painless and bilateral MCFs in patients with facial injuries, particularly in older individuals.
Article Information
Conflicts of Interest
None
Acknowledgement
The author thanks the patient for their kind cooperation.
Author Contributions
KT: Conception and design of the study, acquisition of data, drafting the article, and final approval of the version to be submitted.
Approval by Institutional Review Board (IRB)
IRB approval was not required in this study.
Informed Consent
Written consent has been obtained from the patient to publish the information, including the photographs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kannari L, Marttila E, Thorén H, et al. Mandibular fractures in aged patients - challenges in diagnosis. Dent Traumatol. 2022;38(6):487-94.35950946 10.1111/edt.12778 PMC 9804783 · doi ↗ · pubmed ↗
- 2Inchingolo F, Patano A, Inchingolo AM, et al. Analysis of mandibular muscle variations following condylar fractures: a systematic review. J Clin Med. 2023;12(18):5925.37762866 10.3390/jcm 12185925 PMC 10532393 · doi ↗ · pubmed ↗
- 3van der Geer SJ, van Rijn PV, Kamstra JI, et al. Criterion for trismus in head and neck cancer patients: a verification study. Support Care Cancer. 2019;27(3):1129-37.30109487 10.1007/s 00520-018-4402-z PMC 6373229 · doi ↗ · pubmed ↗