Polymyalgia Rheumatica Presenting as Fever of Unknown Origin
Hiroshi Shiba, Hiroki Ozawa, Masato Okada

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
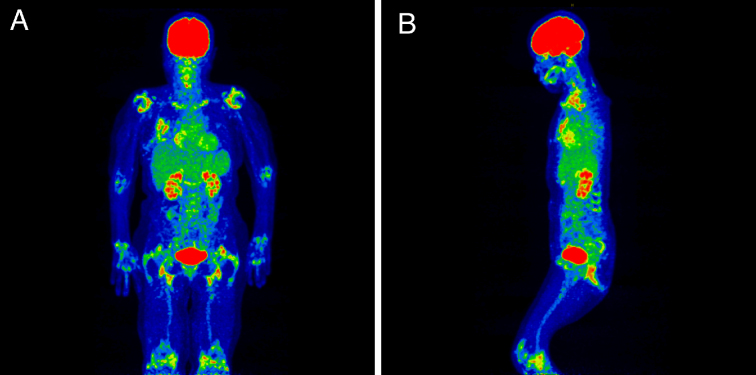 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Myeloproliferative Neoplasms: Diagnosis and Treatment · Systemic Sclerosis and Related Diseases
A 76-year-old woman presented with persistent low-grade fever. She was initially suspected of blood culture-negative infective endocarditis. She underwent an aortic valve replacement and antibiotic treatment. The resected mass was, however, non-infective Lambl’s excrescences. ^18^-fluorine-fluorodeoxyglucose positron emission tomography/computed tomography (^18^F-FDG-PET/CT) was performed to detect foci of infection. Instead, it revealed FDG uptake, including around the shoulders and hips, in the interspinous regions and adjacent to the ischial tuberosities (Figure 1). She was referred to the rheumatology department. Focused history-taking revealed bilateral thigh pain with morning stiffness. Physical examination showed edematous extremities and limited range of motion in the wrists and ankles. Ultrasonography identified bilateral biceps tenosynovitis and distal synovitis. Rheumatoid factor and anti-cyclic citrullinated peptide antibodies were negative. She was diagnosed with polymyalgia rheumatica (PMR). Lambl’s excrescences were considered a coincidental finding unrelated to PMR.
The use of ^18^F-FDG-PET/CT is currently supported in the diagnostic process of fever of unknown origin ^(1), (2)^. Furthermore, this modality has emerged as a gold standard investigation for PMR ^(3)^. Its combined pathognomonic PET/CT findings include FDG uptake in the periarticular regions of the shoulders and hips, in the interspinous regions, and adjacent to the ischial tuberosities ^(3)^. PET/CT also helps to identify coexistent vasculitis and exclude relevant differential diagnoses including clinically silent extra septic foci ^(3), (4)^.
Article Information
Conflicts of Interest
None
Author Contributions
HS acquired data and drafted the manuscript. HO and MO reviewed and supervised the manuscript.
Informed Consent
We have obtained informed consent for this manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wright WF, Kandiah S, Brady R, et al. Nuclear medicine imaging tools in fever of unknown origin: time for a revisit and appropriate use criteria. Clin Infect Dis. 2024;78(5):1148-53.38441140 10.1093/cid/ciae 115PMC 11093677 · doi ↗ · pubmed ↗
- 2Hess S, Noriega-Álvarez E, Leccisotti L, et al. EANM consensus document on the use of [18F]FDG PET/CT in fever and inflammation of unknown origin. Eur J Nucl Med Mol Imaging. 2024;51(9):2597-613.38676736 10.1007/s 00259-024-06732-8PMC 11224117 · doi ↗ · pubmed ↗
- 3Owen CE, Poon AMT, Liu B, et al. Characterising polymyalgia rheumatica on whole-body 18F-FDG PET/CT: an atlas. Rheumatol Adv Pract. 2024;8(1):rkae 003.38375531 10.1093/rap/rkae 003PMC 10876394 · doi ↗ · pubmed ↗
- 4Ghanem-Zoubi N. FDG PET/CT in cardiac infection: does it matter? A narrative review. Infect Dis Ther. 2022;11(5):1769-77.35913678 10.1007/s 40121-022-00679-9PMC 9617977 · doi ↗ · pubmed ↗