Targeted therapy acts to sensitize stereotactic body radiotherapy for pulmonary oligometastases from colorectal cancer
Xiye Sun, Pei Shu, Yali Shen, Zhiping Li, Ning Liu, Ganlu Ouyang, Yuanling Tang, Meijuan Huang, Xin Wang

TL;DR
Adding targeted drugs like cetuximab or bevacizumab to radiotherapy improves survival and control of lung metastases in colorectal cancer patients.
Contribution
This study shows that combining targeted therapy with radiotherapy improves outcomes for pulmonary metastases from colorectal cancer.
Findings
Combining SBRT with cetuximab or bevacizumab significantly improved local control and survival rates.
Tumor size <2 cm and higher BED10 correlated with better local control.
All regimens were well tolerated, though targeted therapies increased toxicity.
Abstract
Stereotactic body radiation therapy (SBRT) is used to manage lung metastases arising from colorectal cancer (CRC), but its effectiveness is constrained by the radioresistance of CRCs. Here, we explored whether concurrent therapy with cetuximab or bevacizumab could improve the prognosis of CRC patients with pulmonary oligometastases. CRC patients with oligometastatic lung tumors (OLTs) treated with concurrent chemoradiotherapy from March 2011 to March 2023 were retrospectively analyzed. Treatment outcomes for local control rate (LCR), progression-free survival (PFS), overall survival (OS), and toxicities were assessed. Sixty-nine patients were included, with a median follow-up of 34 months. The 1-year LCRs for SBRT + chemotherapy, SBRT + chemotherapy + bevacizumab, and SBRT + chemotherapy + cetuximab were 63.3%, 96.2%, and 94.4%, respectively. Incorporating bevacizumab or cetuximab…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
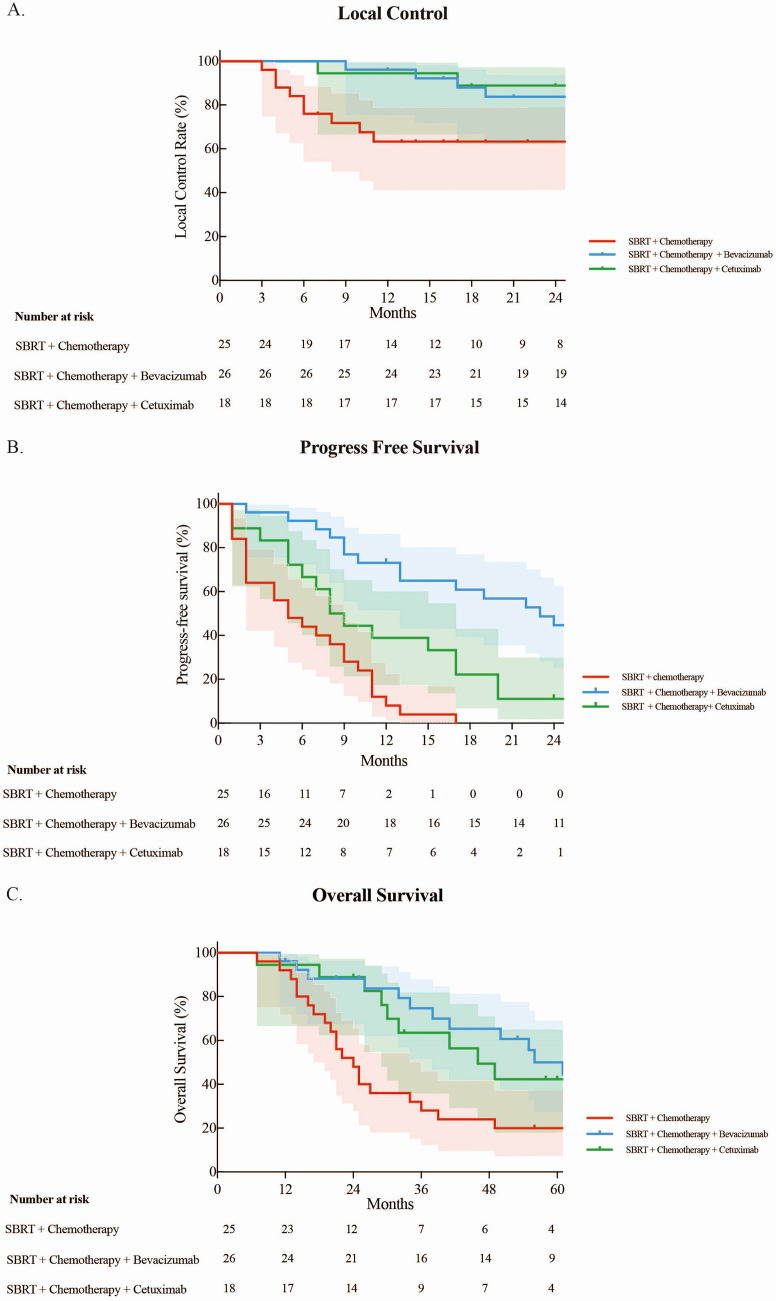 Figure 1
Figure 1| Baseline characteristics | All patients (n = 69) |
|---|---|
| Age (years) | |
| Median | 61 |
| Range | 40–87 |
| Gender, n (%) | |
| Male | 41 (59.4%) |
| Female | 28 (40.6%) |
| Primary site, n (%) | |
| Colon | 22 (31.9%) |
| Rectum | 47 (68.1%) |
| Previous site of metastases, n (%) | |
| Liver metastases | 27 (39.1%) |
| Other sites (lymph nodes) | 42 (60.9%) |
| Type of oligometastases | |
| Synchronous | 6 (8.7%) |
| Metachronous | 63 (91.3%) |
| Number of lesions per patient | |
| 1 lesion | 54 (78.3%) |
| 2 lesions | 13 (18.8%) |
| 3 lesions | 2 (2.9%) |
| Tumor size (cm) | |
| Median | 1.4 |
| Range | 0.3–5.0 |
| BED10 (Gy) | |
| Median | 105.6 |
| Range | 50.0-180.0 |
| Treatment, n (%) | |
| SBRT + chemotherapy | 25 (36.2%) |
| SBRT + chemotherapy + bevacizumab | 26 (37.7%) |
| SBRT + chemotherapy + cetuximab | 18 (26.1%) |
| Characteristics | SBRT + | SBRT+ chemotherapy + | SBRT + chemotherapy+ |
|
|---|---|---|---|---|
| Age | 0.046 | |||
| Median (range) | 67 (42–87) | 58 (47–75) | 58 (40–76) | |
| M ± SD | 65.0 ± 12.6 | 58.9 ± 7.6 | 57.9 ± 10.5 | |
| Gender | 0.46 | |||
| Male | 16 | 13 | 12 | |
| Female | 9 | 13 | 6 | |
| Tumor size (cm) | 0.45 | |||
| Median (range) | 1.5 (0.6-5.0) | 1.4 (0.3–3.8) | 1.2 (0.4-4.0) | |
| M ± SD | 1.7 ± 1.2 | 1.4 ± 0.8 | 1.4 ± 0.9 | |
| Primary site | 0.43 | |||
| Colon | 10 | 6 | 6 | |
| Rectum | 15 | 19 | 12 | |
| BED10 (Gy) | 0.59 | |||
| Median (range) | 105.6 (72.0-132.0) | 105.6 (60.0-132.0) | 105.6 (50.0-180.0) | |
| M ± SD | 106.9 ± 18.7 | 104.9 ± 23.6 | 112.4 ± 30.2 |
| Factors | Overall survival | Progression-free survival | Local control | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Hazard ratio | 95% CI |
| Hazard ratio | 95% CI |
| Hazard ratio | 95% CI |
| |
| Age (<60 vs. ≥60) | 0.70 | 0.39–1.25 | 0.23 | 0.87 | 0.53–1.43 | 0.58 | 0.94 | 0.48–1.83 | 0.86 |
| Gender (female vs. male) | 0.81 | 0.45–1.48 | 0.50 | 1.15 | 0.69–1.90 | 0.60 | 1.02 | 0.52–2.01 | 0.95 |
| Primary site (rectum vs. colon) |
| 0.25–0.84 |
| 0.81 | 0.47–1.38 | 0.43 | 0.69 | 0.34–1.39 | 0.29 |
| Treatment (chemotherapy vs. targeted therapy) |
| 1.48–4.76 |
|
| 2.16–7.08 |
| 1.99 | 0.99–3.40 | 0.05 |
| Tumor size (<2 vs. ≥2) | 0.52 | 0.27–1.02 | 0.06 | 0.57 | 0.31–1.02 | 0.06 |
| 0.14–0.58 |
|
| BED10 (<100 vs. ≥100) |
| 1.05–4.30 |
| 1.32 | 0.71–2.44 | 0.40 |
| 1.05–5.01 |
|
| ECOG PS | 0.52 | 0.26–1.03 | 0.06 |
| 0.27–0.82 |
| 0.55 | 0.26–1.18 | 0.13 |
| Factors | Overall survival | Progression-free survival | Local control | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Hazard ratio | 95% CI |
| Hazard ratio | 95% CI |
| Hazard ratio | 95% CI |
| |
| Age (<60 vs. ≥60) | 0.88 | 0.45–1.72 | 0.72 | 0.93 | 0.51–1.68 | 0.80 | 0.85 | 0.40–1.81 | 0.67 |
| Gender (female vs. male) | 0.89 | 0.46–1.71 | 0.73 | 1.22 | 0.69–2.14 | 0.50 | 1.30 | 0.58–2.93 | 0.53 |
| Primary site (rectum vs. colon) | 0.63 | 0.33–1.21 | 0.16 | 1.09 | 0.60–1.98 | 0.77 | 1.41 | 0.61–3.22 | 0.42 |
| Treatment (chemotherapy vs. targeted therapy) |
| 1.07–3.92 |
|
| 1.96–6.89 |
| 1.91 | 0.90–4.07 | 0.09 |
| Tumor size (<2 vs. ≥2) | 0.70 | 0.33–1.49 | 0.35 |
| 0.26–0.97 |
|
| 0.12–0.66 |
|
| BED10 (<100 vs. ≥100) | 1.46 | 0.63–3.63 | 0.38 | 1.23 | 0.60–2.53 | 0.58 | 1.88 | 0.71–5.02 | 0.21 |
| ECOG PS | 0.70 | 0.33–1.50 | 0.36 | 0.62 | 0.33–1.17 | 0.14 | 0.75 | 0.33–1.72 | 0.50 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Advanced Radiotherapy Techniques · Lung Cancer Treatments and Mutations
Introduction
Colorectal cancer (CRC) ranks as the third main cause of death and the second leading cause of cancer-related deaths worldwide (1). The second most common site for metastases from CRC is the lung, detected in 10% to 20% of cases (2, 3). Surgery is the standard treatment for CRC patients with oligometastatic lung tumors (OLTs) (4). However, the median survival does not exceed 10 months without surgery, especially for patients where surgery is not an option (5–7). Stereotactic body radiation therapy (SBRT) has been reported to improve the local control of lung oligometastases from CRC, with a 1-year local control rate (LCR) ranging from 62% to 92% (8), which is suboptimal (9–11). Therefore, we and others in the field are exploring strategies to enhance the efficacy of SBRT. Our recent study demonstrated that an increased dose (60 Gy in 5 fractions) could lead to enhanced local recurrence-free survival in patients (12). However, limitations in normal tissue tolerance represent a confounder in achieving the desired radiation intensity during SBRT. Therefore, employing radiation sensitizers in conjunction with SBRT presents a viable strategic approach.
Prior research suggests that cetuximab and bevacizumab enhance radiosensitivity. In advanced head and neck cancer, combining cetuximab with radiotherapy significantly improved local control and survival (13, 14). Preclinical studies support this, showing that cetuximab enhances radiotherapy efficacy in CRC cells by inhibiting DNA repair (15, 16). Similarly, anti-Vascular Endothelial Growth Factor therapy has demonstrated radiosensitizing effects in preclinical models (17). In CRC patients with lung oligometastases, bevacizumab increased complete response rates by 21% following stereotactic ablative radiotherapy (18).
Currently, there is limited evidence for SBRT-based combination chemotherapy with targeted therapy including cetuximab or bevacizumab to manage CRC patients. Here, we reported a retrospective study to investigate whether bevacizumab or cetuximab could improve the radiotherapy sensitivity of CRC patients with OLTs.
Materials and methods
Patient characteristics
The CRC patients with OLTs who were treated with SBRT-based combination therapy in West China Hospital, Sichuan University, between March 2011 and March 2023, were evaluated. The selection criteria were as follows: age ≥ 18 years, the primary tumor was colorectal adenocarcinoma, the primary tumor had been surgically removed, OLTs arose postoperatively from CRC, distant metastasis to ≤2 organs (lung alone or lung combined with liver, lymph nodes, etc.), total metastasis number ≤5, and maximal tumor diameter ≤5 cm. The lung metastases were medically inoperable, and extra-lung tumor sites were controlled, with Eastern Cooperative Oncology Group performance score (ECOG-PS) ≤1. Response assessment adhered to the Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 guidelines. CT scans were employed to appraise the irradiation target area, given that the challenges in discerning between recurrence and pseudoprogression following SBRT, the integration of FDG-PET, and the utilization of pathological biopsy, whenever feasible, contributed to a more nuanced and thorough evaluation. The pulmonary toxicity evaluation was based on Common Terminology Criteria for Adverse Events (CTCAE) 5.0 standards (19, 20).
SBRT technique
All patients received SBRT for pulmonary oligometastases. For those whose respiratory movement (measured using IGRT motion view or Image-Guided Radiation Therapy with Four-Dimensional Cone-Beam Computed Tomography) was greater than 1 cm in the head–foot direction, active breath control (ABC) was used to control such movement. For respiratory movements less than 1 cm, four-dimensional CT (4DCT) was used to control respiratory movements. Gross tumor volume (GTV) was delineated using CT lung windows. The internal target volume (ITV) consisted of the union of 10 GTV contours of 4D breathing phases. The clinical target volume (CTV) corresponded to the ITV. The planning target volume (PTV) was defined as the ITV, the upper and lower sides were expanded by 10 mm, and the surrounding sides were expanded by 5 mm. Radiotherapy doses were administered depending on the size and location of the tumor. The radiotherapy dosage was determined based on the physician’s expertise, with the prescribed dose to the PTV ranging from 35 to 60 Gy in 3 to 10 fractions, three times per week. The PTV encompassed 80% of the isodose volume (ranging from 60% to 90%). To meet target dose criteria, more than 95% of the PTV must be covered, with 99% of the PTV receiving a prescribed radiation dose of at least 90% of the total. If the dose exceeds 105%, it should fall within the PTV range.
Chemotherapy and targeted therapy
All the patients received concurrent chemoradiotherapy. Chemotherapy regimens included mFOLFOX6, FOLFIRI, and XELOX. During concurrent radiotherapy, chemotherapy was administered as planned, but the dose of chemotherapy could be properly adjusted based on the patient’s condition and tolerance (70%–80% of the usual dose could be administered). Before initiating cetuximab treatment, all patients underwent genetic testing. Those with RAS wild type could proceed with cetuximab with a dose of 500 mg/m^2^ every 2 weeks. The number of cetuximab administrations varied between two and four– times, depending on the radiotherapy dose group. The bevacizumab dose was 5 mg/kg every 2 weeks (mFOLFOX6/FOLFIRI-based regimens) or 7.5 mg/kg every 3 weeks (XELOX-based regimens). After synchronous treatment, maintenance therapy was tailored by the attending physician based on the patient’s condition.
Follow-up
Efficacy evaluations were conducted 1 month after the end of radiotherapy and every 3–4 cycles during chemotherapy thereafter. After the treatment, follow-up and efficacy evaluations were typically conducted according to the requirements of the physician in charge. The evaluations were performed at least once every 3 to 6 months.
Statistical analysis
Local control duration was measured from SBRT initiation to local progression. Overall survival (OS) duration was calculated from SBRT start to death. Progression-free survival (PFS) duration was calculated from the commencement of SBRT to tumor progression or death. LCR, PFS, and OS were all calculated using the Kaplan–Meier analyses. The results of subgroups were compared using the log-rank or Gehan–Breslow–Wilcoxon test. Univariate and multivariate Cox regression analyses were used to calculate the influence of variables on OS, PFS, and LCR. All statistical tests were two-sided. Values of p-value <0.05 were indicated as statistically significant. SPSS 20 (IBM Corporation, Armonk, NY, USA) and Prism 9 (GraphPad Software, San Diego, CA, USA) were used for statistical analyses.
Results
Patient characteristics
There were 86 lung oligometastases in 69 patients (41 men and 28 women) included. The median age was 61 (40–87). The number of lung oligometastases treated per patient ranged from one to three. Among the patients, 22 patients with OLTs originated from the colon, while others from the rectum. Before receiving SBRT, 27 patients had undergone treatments for liver metastases. Among them, 13 patients successfully underwent radical resection of liver metastases with no observed recurrence. Additionally, three patients underwent radiofrequency ablation, another three received local SBRT, and eight underwent systemic chemotherapy. All liver lesions were under stable control.
The treatment regimens administered were as follows: SBRT + chemotherapy for 25 patients, SBRT + chemotherapy + bevacizumab for 26 patients, and SBRT + chemotherapy + cetuximab for 18 patients. The median tumor size of OLTs was 1.4 cm (0.3–5.0 cm), and the median biologically effective dose (BED_10_) of SBRT was 105.6 Gy (range, 50.0–180.0 Gy). Table 1 shows the characteristics of the patients. Table 2 reveals the baseline characteristics of each patient group.
Local control
The median follow-up period after SBRT for OLTs from CRC was 34 months. The 1- and 2-year LCRs were 84.0% and 77.4%, respectively. Patients treated with bevacizumab or cetuximab had better local control (p < 0.05). The 1– and 2-year LCRs for the SBRT + chemotherapy arm, SBRT + chemotherapy + bevacizumab arm, and SBRT + chemotherapy + cetuximab arm were 63.3% vs. 96.2% vs. 94.4%, and 63.3% vs. 83.8% vs. 88.9%, respectively (Figure 1A). The 1- and 2-year LCRs for patients with one, two, and three lung lesions treated simultaneously were 81.4% vs. 92.3% vs. 50.0%, and 74.8% vs. 84.6% vs. 50.0%, respectively (p > 0.05).
(A) Local control rate. (B) Progression-free survival. (C) Overall survival of three groups.
Progression-free survival
The median PFS for all included patients was 10 months, with the 1-, 3-, and 5-year PFS rates being 40.6%, 14.7%, and 10.7%, respectively. The median PFS rates for the SBRT + chemotherapy arm, SBRT + chemotherapy + bevacizumab arm, and SBRT + chemotherapy + cetuximab arm were 5, 23, and 8 months, respectively. Patients treated with targeted therapy had longer PFS compared with those treated with chemotherapy (p < 0.05). The 1-year PFS rates were 8.0%, 73.1%, and 38.9% for the SBRT + chemotherapy arm, SBRT + chemotherapy + bevacizumab arm, and SBRT + chemotherapy + cetuximab arm, respectively. All SBRT + chemotherapy patients experienced progression within 2 years. The 2-year PFS rates were 44.7% and 11.1%, respectively, in the SBRT + chemotherapy + bevacizumab arm and SBRT + chemotherapy + cetuximab arm (Figure 1B).
Overall survival
The median OS for all 69 patients was 41 months with the 1-, 3-, and 5-year OS rates of 94.2%, 54.1%, and 37.0%, respectively. The median OS rates for the SBRT + chemotherapy arm, SBRT + chemotherapy + bevacizumab arm, and SBRT + chemotherapy + cetuximab arm were 24, 61, and 46 months, respectively. Patients treated with targeted drugs had longer survival compared with chemotherapy (p < 0.05). The 1-, 3-, and 5-year OS rates for the arms receiving SBRT + chemotherapy, SBRT + chemotherapy + bevacizumab, and SBRT + chemotherapy + cetuximab were as follows: 92.0% vs. 96.2% vs. 94.4%, 28.0% vs. 74.7% vs. 63.5%, and 20.0% vs. 50.0% vs. 42.3%, respectively (Figure 1C).
Factors affecting the treatment outcomes
In our comprehensive univariate analysis (Table 3), we analyzed the influence of various factors, including age, gender, primary tumor site, tumor size, BED_10_ value, ECOG-PS score, and treatment on OS, PFS, and LCRs. We observed that tumor size <2 cm and BED_10_ ≥ 100 Gy were correlated with improved local control (p < 0.05), and other factors had no relevant statistical significance. For BED_10_ ≥ 100 Gy, the primary site was the rectum, and patients under targeted therapy of bevacizumab or cetuximab were associated with improved OS (p < 0.05). Moreover, patients under targeted therapy of bevacizumab or cetuximab and ECOG-PS = 0 were linked to prolonged PFS (p < 0.05).
In our comprehensive multivariate analysis (Table 4), we identified that tumor size <2 cm was associated with better local control (p < 0.05). The remaining factors analyzed were not statistically relevant. Patients under targeted therapy were linked to prolonged OS (p < 0.05). Furthermore, there exhibited significant associations with improved PFS (p < 0.05): tumor size <2 cm and patients undergoing targeted therapy.
Toxicity
No instances of grade 4 or 5 radiation pneumonitis were observed, and there were no other toxicities reported at or above grade 4. Notably, patients in the SBRT + chemotherapy arm exhibited the lowest incidence of AEs.
The incidence rates of grade 2–3 radiation pneumonitis were 8% (2/25) in the SBRT + chemotherapy arm compared to 19.2% (5/26) in the SBRT + chemotherapy + bevacizumab arm. In the SBRT + chemotherapy + cetuximab arm, 16.7% (3/18) patients experienced grade 2–3 radiation pneumonitis.
Patients on targeted therapies exhibited elevated rates of hematologic toxicities (p < 0.05). The hematological toxicity rates in the SBRT + chemotherapy arm, SBRT + chemotherapy + bevacizumab arm, and SBRT + chemotherapy + bevacizumab arm were 4% (1/25), 38.5% (10/26), and 38.9% (7/18), respectively. Grade 2 toxicity occurred in one patient in the SBRT + chemotherapy arm. Grade 3 occurred in one patient, grade 2 in six patients, and grade 1 in three patients in the SBRT + chemotherapy + bevacizumab arm. In the SBRT + chemotherapy + cetuximab arm, four patients had grade 1, and two had grade 2 toxicity. Furthermore, three patients treated with SBRT + chemotherapy + cetuximab presented grade 1–2 rash.
Discussion
Current evidence indicates that SBRT is effective in managing oligometastases from CRC (21, 22). It is recognized that OLTs originating from CRC are connected with decreased PFS (23), and such tumors exhibit lower radiosensitivity than other subtypes, possibly due to increased hypoxia and extensive micro-invasion (24–26). To enhance SBRT’s performance as a treatment option for OLTs from CRCs, we explored the use of radiotherapy sensitizers in a retrospective study. By combining cetuximab or bevacizumab with SBRT-based chemoradiotherapy, we aimed to improve local control and survival outcomes.
We found that the addition of bevacizumab or cetuximab to SBRT-based concurrent chemoradiotherapy led to prolonged OS and PFS and improved local tumor control. In certain patients, local lesions remained stable or even regressed for a duration exceeding 2 years, with LCR at 1 year surpassing 90%. While clinical data for cetuximab or bevacizumab treatment in the context of CRC are limited, our findings align with those of previous studies (14, 27, 28). Cetuximab triggered DNA damage and hampered CRC cell proliferation in vitro and reduced tumor growth in mouse models, ultimately increasing the radiosensitivity of CRC cell lines (15, 16). Prior studies have also demonstrated that bevacizumab combined with chemoradiotherapy could improve survival in mCRC: metastatic colorectal cancer cases (29–32). Anti-VEGF therapy exhibited radiosensitizing properties in both tumor cell lines and mouse models (17). This phenomenon may be attributed to radiotherapy, triggering a vascular rebound effect, thereby inducing the growth of new blood vessels. This, in turn, results in tissue hypoxia and promotes the heightened expression of VEGF with downstream effects on cell signaling (33–35). In this study, cetuximab exhibited a shorter PFS compared to bevacizumab. We found that liver metastasis occurred early in 44.44% of patients post-treatment with SBRT + chemotherapy + cetuximab, whereas only 15.38% of patients receiving SBRT + chemotherapy + bevacizumab group experienced liver metastasis after treatment. Our data draw a potential link between bevacizumab treatment, tumor angiogenesis inhibition, and reduced early liver metastasis incidence. Our current findings from a limited sample size warrant future validation through large-scale studies.
In our comprehensive univariate analysis, BED_10_ ≥ 100 Gy was associated with improved OS and better local control. Patients under targeted therapy showed improved OS and PFS, and tumor size <2 cm was linked to better local control. These findings aligned with prior research outcomes, as multiple studies have consistently indicated that a higher BED_10_ was linked to improved local control and enhanced survival in cases of mCRC with lung oligometastases (8, 36, 37). Yu et al. found that BED_10_ ≥ 100 Gy was more effective than BED_10_ < 100 Gy in patients with OM-CRC: oligometastatic colorectal cancer in terms of 1-year local control (94.4% vs. 63.2%, p = 0.022) and 1-year OS (100% vs. 73.4%, p = 0.028) (37). Alongi et al. also reported an excellent 2-year local PFS rate of 80% for colorectal metastases treated with a median BED_10_ of 105 Gy (38). Another study also confirmed that the 2-year cumulative local treatment failure rate for colorectal metastases treated with BED_10_ < 100 Gy was significantly higher than that for colorectal metastases treated with BED_10_ ≥ 100 Gy at 62.5% and 16.7%, respectively (p < 0.08) (39). Researchers found that lung metastases from CRC were radioresistant, resulting in high recurrence rates after SBRT. Hence, to improve local tumor control, they recommend dose escalation with BED_10_ > 100 Gy (36, 40). Our earlier investigation revealed that OLTs treated with higher doses (BED_10_ = 132 Gy) exhibited superior local control rates compared to those treated with lower doses (BED_10_ ≤ 105.6 Gy) (12). In this study, the targeted agent functioned as a sensitizer, enhancing local control even at doses of BED_10_ ≥ 100 Gy. Prior studies have highlighted the significance of tumor size before SBRT as a prognostic factor. Patients with larger lung metastases demonstrated poorer local control (41, 42). Both the univariate and multivariate analyses in this study revealed that, in comparison to patients with tumors ≥2 cm, those with tumor size <2 cm exhibited improved local control. This is consistent with previous findings. For larger tumors with a higher chance of hidden distant spread, a higher radiation dose may be necessary for effective control (43). We also investigated the relationship between the number of lung lesions treated simultaneously and local control rates. However, due to the inconsistency in the systemic treatment regimens among the groups, baseline heterogeneity, and the small sample size, we were unable to draw definitive conclusions from this statistical result. In future studies, we plan to increase the sample size, standardize patient baseline characteristics, and conduct a more in-depth investigation of this issue. Our univariate analysis revealed patients with better performance status had longer PFS, which was consistent with the results of Ji et al. (5).
Here, we found that cetuximab or bevacizumab treatment showed slightly higher rates of hematologic toxicity in this research, consistent with previous studies in CRC and recurrent malignant glioma (18, 44, 45). However, relevant studies in colorectal cancer are currently very limited, and further research with larger sample sizes is needed. The combination of radiotherapy with bevacizumab or cetuximab showed a trend toward increased radiation pneumonitis, although this finding was not statistically significant. Further validation with a larger sample size will substantiate this observation. Moreover, previous studies also reported that bevacizumab treatment could be linked to the inhibition of the repair of damaged lung endothelial tissues and the recruitment of inflammatory factors (46). Also, cetuximab was found to cause rash due to its involvement in releasing pro-inflammatory chemokines and attracting T-cell and neutrophil infiltration (47). Nevertheless, in our current study, we found that the overall toxicity of combination therapy was tolerable.
This single-center retrospective study has several limitations, including the small patient cohort and retrospective design. Due to the retrospective nature of the research, its validity is inherently limited. The study included all eligible patients between March 2011 and March 2023, ensuring comprehensive inclusion to minimize selection bias as much as possible. Many patients were in the advanced stages of CRC, and the majority had undergone multiple lines of treatment before receiving SBRT + chemotherapy, which inevitably affected the efficacy of SBRT. Limited insurance coverage for some patients meant they lacked access to genetic testing and chemotherapy with cetuximab/bevacizumab. Our current findings should be validated in larger, preferably prospective studies. Additionally, screening for predictive biomarkers is recommended when combining anti-angiogenic drugs for more precise treatment.
Conclusion
This single-site study shows that a combination of SBRT-based concurrent chemoradiotherapy with bevacizumab or cetuximab is effective for treating pulmonary oligometastases from CRC. Retrospective analyses consistently showed improved LCR, PFS, and OS with cetuximab or bevacizumab.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660 33538338 · doi ↗ · pubmed ↗
- 2Shin AE Giancotti FG Rustgi AK. Metastatic colorectal cancer: mechanisms and emerging therapeutics. Trends Pharmacol Sci. (2023) 44:222–36. doi: 10.1016/j.tips.2023.01.003 PMC 1036588836828759 · doi ↗ · pubmed ↗
- 3Penna C Nordlinger B. Colorectal metastasis (liver and lung). Surg Clin North Am. (2002) 82:1075–90. doi: 10.1016/s 0039-6109(02)00051-8 12507210 · doi ↗ · pubmed ↗
- 4Pastorino U Buyse M Friedel G Ginsberg RJ Girard P Goldstraw P. Long-term results of lung metastasectomy: prognostic analyses based on 5206 cases. J Thorac Cardiovasc Surg. (1997) 113:37–49. doi: 10.1016/s 0022-5223(97)70397-0 9011700 · doi ↗ · pubmed ↗
- 5Ji X Zhao Y Zhu X Shen Z Li A Chen C. Outcomes of stereotactic body radiotherapy for metastatic colorectal cancer with oligometastases, oligoprogression, or local control of dominant tumors. Front Oncol. (2020) 10:595781. doi: 10.3389/fonc.2020.595781 33585211 PMC 7878536 · doi ↗ · pubmed ↗
- 6Navarria P De Rose F Ascolese AM. SBRT for lung oligometastases: Who is the perfect candidate? Rep Pract Oncol Radiother. (2015) 20:446–53. doi: 10.1016/j.rpor.2014.11.005 PMC 466135026696785 · doi ↗ · pubmed ↗
- 7Simmonds PC. Palliative chemotherapy for advanced colorectal cancer: systematic review and meta-analysis. Colorectal Cancer Collaborative Group. Bmj. (2000) 321:531–5. doi: 10.1136/bmj.321.7260.531 PMC 2746610968812 · doi ↗ · pubmed ↗
- 8Kobiela J Spychalski P Marvaso G Ciardo D Dell'Acqua V Kraja F. Ablative stereotactic radiotherapy for oligometastatic colorectal cancer: Systematic review. Crit Rev Oncol Hematol. (2018) 129:91–101. doi: 10.1016/j.critrevonc.2018.06.005 30097241 · doi ↗ · pubmed ↗