Vascularized Chin Fat Flap for Mandibular Reconstruction in Stable Scleroderma En Coup De Sabre: A Case Report and Review of Surgical Considerations
Yuki Odagiri, Naoki Matsuura, Edward H Ntege, Reiko Asato, Yusuke Shimizu

TL;DR
A new surgical technique using a vascularized chin fat flap is introduced to treat facial atrophy in a patient with stable scleroderma en coup de sabre.
Contribution
This is the first reported use of a vascularized chin fat flap for mandibular reconstruction in ECDS.
Findings
The patient showed sustained volume and facial symmetry six months post-surgery.
The flap preserved its vascular supply and resulted in excellent scar quality with no complications.
The technique offers a single-stage, minimally invasive alternative to existing methods.
Abstract
Scleroderma en coup de sabre (ECDS) is a rare form of linear scleroderma that typically causes progressive atrophy on the face, which can affect both appearance and function over time. Although various reconstructive strategies exist, the use of a vascularized chin fat flap (CFF) for mandibular soft tissue restoration has not been previously reported. We describe a 61-year-old woman with stable ECDS and anterior mandibular depression. After disease stabilization with methotrexate, a pedicled fat flap was harvested from the submental region and inset via a single incision while preserving its native vascular supply. At six months, the patient exhibited sustained volume, restored facial symmetry, excellent scar quality, and no complications. The CFF combines vascular reliability, anatomical compatibility, and minimal invasiveness. Its ability to achieve natural, long-lasting results in a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
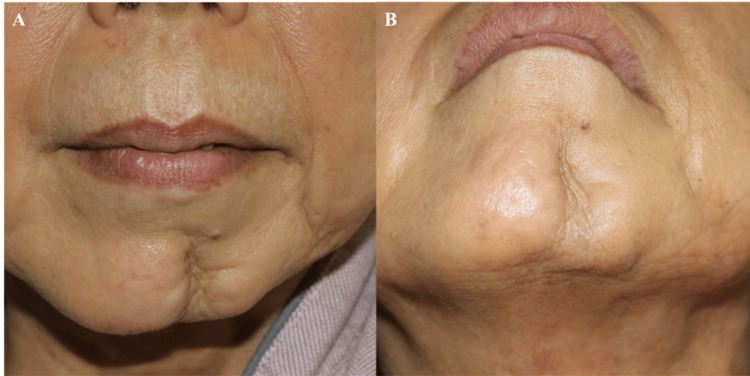 Figure 1
Figure 1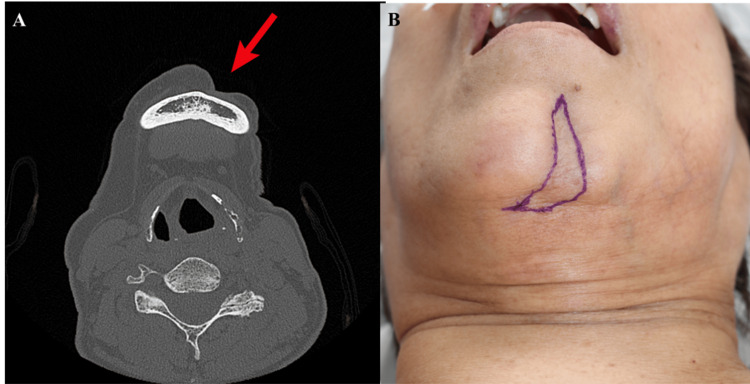 Figure 2
Figure 2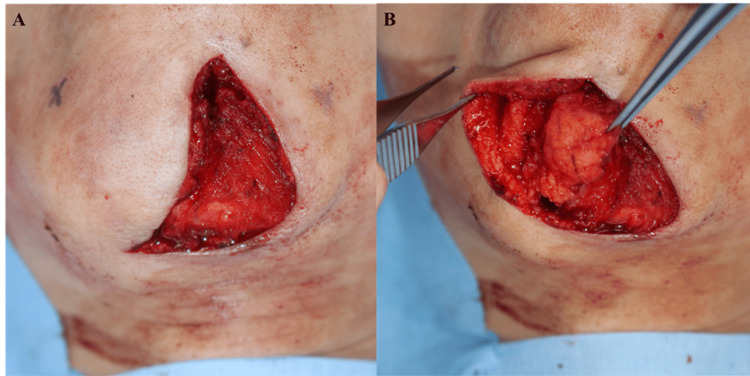 Figure 3
Figure 3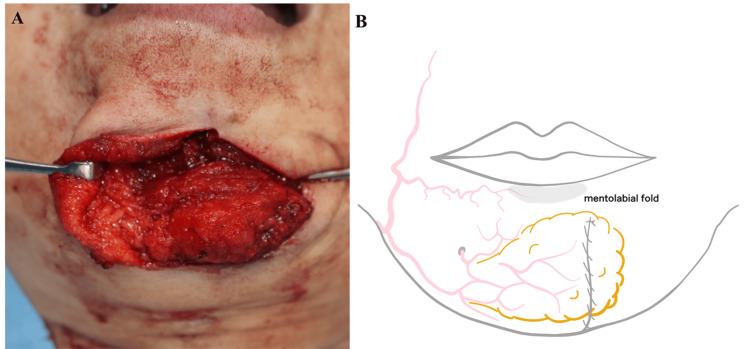 Figure 4
Figure 4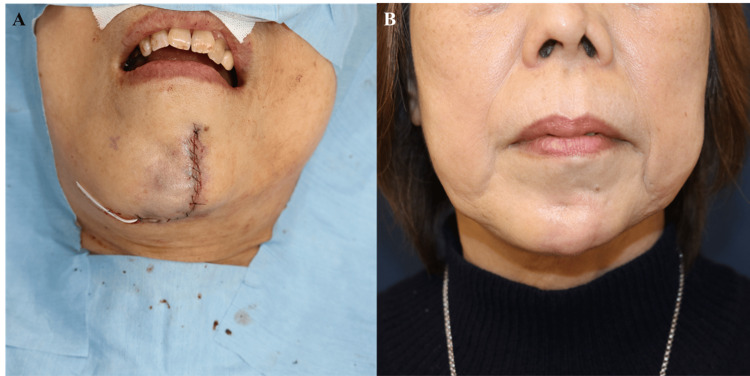 Figure 5
Figure 5 Figure 6
Figure 6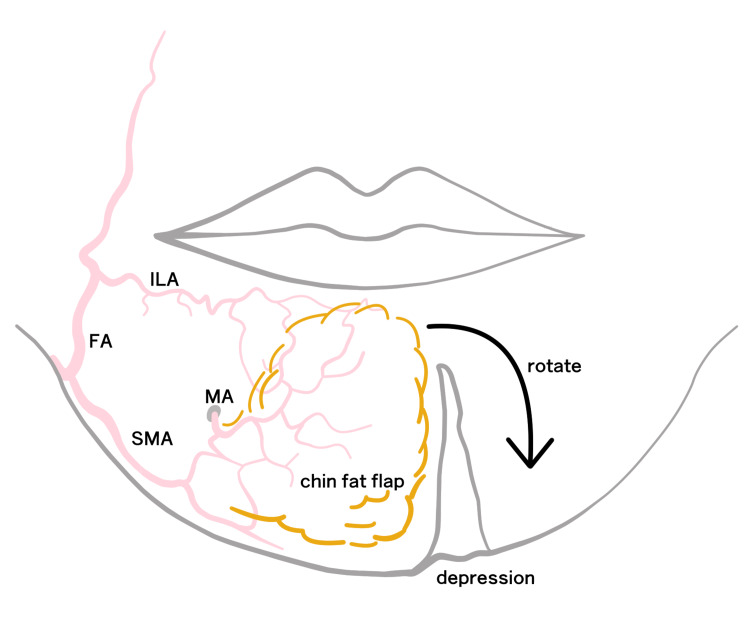 Figure 7
Figure 7| Method | Advantages | Disadvantages | Reference(s) |
| Autologous fat grafting | Minimally invasive; repeatable; improves skin pliability | Unpredictable resorption; may require multiple sessions; inconsistent volume retention |
[ |
| HA filler | Office-based procedure; reversible; readily available | Temporary; risk of granuloma or foreign body reaction; unsuitable for atrophic skin |
[ |
| Botulinum toxin | Minimally invasive; useful for dynamic asymmetry | Temporary effect; no volumetric correction; possible adverse reactions |
[ |
| Alloplastic implants and bone cement | Durable; volume stable; effective in moderate defects | Risk of infection, extrusion, and foreign body reaction; poor tissue texture match |
[ |
| Tissue expander | Provides sufficient soft tissue volume; allows staged reconstruction | Requires two-stage surgery; risk of infection; patient discomfort |
[ |
| Free flaps/bone grafts | Suitable for large or complex defects; permanent correction | Highly invasive; requires surgical expertise; donor site morbidity |
[ |
| CFF | Autologous; vascularized; natural texture; single-stage, potentially under LA | Limited volume; unsuitable for distant or large defects; anatomical constraints | Present study |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Facial Surgery Techniques · Reconstructive Surgery and Microvascular Techniques · Dermatologic Treatments and Research
Introduction
Scleroderma en coup de sabre (ECDS) is a rare subtype of linear scleroderma characterized by linear, atrophic depressions affecting the face or scalp, typically along Blaschko’s lines [1]. With an estimated prevalence of 0.4-2.7 per 100,000 individuals, ECDS predominantly affects females (approximately 3:1 female-to-male ratio) and typically presents during childhood or adolescence, although adult-onset cases occur [2-4]. ECDS is thought to result from a localized autoimmune process that induces inflammatory fibrosis and microvascular dysfunction, leading to progressive atrophy of the skin, subcutaneous tissue, and occasionally bone [1,5].
Although not life-threatening, ECDS can cause progressive atrophy of the skin, subcutaneous fat, and underlying bone, resulting in facial asymmetry and psychosocial distress. The condition typically progresses through an inflammatory phase lasting two to five years, followed by persistent residual deformities [6]. Up to 64% of patients develop osseous involvement, complicating reconstruction [5].
Medical therapy, particularly methotrexate, is the primary treatment to halt progression, demonstrating high efficacy when initiated early [7,8]. A minimum disease-free interval of six to 12 months is recommended before surgical intervention [9,10].
Reconstructive options for correcting soft tissue deficits in ECDS include autologous fat grafting, hyaluronic acid (HA) fillers, dermal-fat grafts, botulinum toxin, alloplastic implants, tissue expanders, and free flaps [8-12]. However, challenges persist due to unpredictable volume retention, multiple procedural requirements, and donor-site morbidity [5,8,9]. Reconstructive efforts in this population are further complicated by poor tissue pliability, compromised vascularity, increased fibrosis, and the potential risk of disease reactivation triggered by surgical manipulation [5,6]. The inherently thin and tethered overlying skin also complicates the achievement of natural contours and symmetry with conventional techniques [5].
Given these limitations, this report introduces the vascularized chin fat flap (CFF) as a novel, anatomically compatible, and minimally invasive reconstructive option for lower facial volume restoration in stable ECDS. Here, we describe the surgical approach and evaluate its position within current reconstructive strategies.
Case presentation
A 61-year-old woman presented with a longstanding, progressive linear depression extending from her forehead to the left anterior mandible. She had not received prior treatment and was diagnosed with ECDS at the age of 60. Following one year of methotrexate therapy (10 mg/week), the disease stabilized clinically, and she was subsequently referred to our Department of Plastic and Reconstructive Surgery at the University of the Ryukyus Hospital for correction of mandibular contour.
Clinical examination revealed a sharply demarcated atrophic depression measuring approximately 8 cm in length and 1-2 cm in width, with a depth ranging from 3 to 8 mm. Digital analysis estimated an affected surface area of approximately 14 cm². Quantitative analysis of the CT scan data demonstrated a 32% soft tissue volume deficit on the affected side compared to the contralateral side. Although CT scan is not traditionally the first-line modality for superficial soft tissue assessment, it allowed reliable volumetric comparison of subcutaneous tissue depth in this case. This objective measurement was instrumental in determining the required dimensions for the planned reconstruction. While dedicated virtual surgical planning software was not utilized, standardized photographic analysis and CT-based volumetric comparison guided our flap design. The overlying skin appeared thin and tethered (Figure 1A, 1B).
Preoperative views(A) Frontal view showing a depressed lesion on the left anterior mandible. (B) Oblique view demonstrating a linear depression toward the submandibular region.
CT imaging confirmed soft tissue atrophy without underlying bony involvement (Figure 2A).
Preoperative imaging and planning(A) Axial CT showing soft tissue atrophy without bony involvement. (B) Skin marking, outlining scar excision, and flap design.
Based on the characteristic linear depression along Blaschko’s lines, confirmatory CT findings of isolated soft tissue atrophy, and clinical stabilization after one year of methotrexate therapy, the diagnosis of ECDS was firmly established. Differential diagnoses methodically excluded included Parry-Romberg syndrome (PRS, due to lack of deeper tissue and neurological involvement), traumatic or postsurgical scarring (ruled out by clinical history and lesion progression), linear morphea without craniofacial involvement (dismissed based on strictly facial localization), post-radiation atrophy (excluded by absence of radiation history), and hemifacial microsomia (eliminated given the clearly acquired and progressive presentation). This comprehensive diagnostic evaluation confirmed stable ECDS, thus providing a solid foundation for the subsequent reconstructive approach.
Preoperative markings were made to guide scar excision and flap design (Figure 2B).
Under general anesthesia (GA), a 7.2 cm incision was made along the mentolabial fold to excise the scar and release adhesions (Figure 3A). Given the moderate volume deficit, local tissue availability, and patient preference for minimal morbidity, a pedicled fat flap measuring 5.3 cm × 3.2 cm × 1.8 cm (approximately 30.5 cm³) was harvested from the right submental region through the same incision. Dissection was performed in a submuscular plane, carefully preserving the mentalis and depressor muscles. The vascular pedicle, approximately 1.2 cm wide, included branches from the facial, submental, and mental arteries (Figure 3B).
Intraoperative flap harvest(A) Scar excision and exposure of atrophic tissue. (B) Elevation of the CFF with preserved lateral pedicle.CFF, chin fat flap
The flap was rotated superomedially approximately 70° and secured to the periosteum using five 4-0 PDS sutures (Figure 4A). The flap contour was aligned with the mentolabial groove to ensure natural aesthetic restoration (Figure 4B).
Flap insetting and design(A) Rotation and insetting of the flap into the defect. (B) Flap design aligned with the mentolabial groove.
Closure was performed in layers using 5-0 Vicryl and 6-0 nylon sutures. A closed-suction drain placed intraoperatively was removed on postoperative day 2, with a total drainage of 22 mL (Figure 5A).
Wound closure and early result(A) Layered closure over the drain without tension. (B) Six-month postoperative frontal view showing contour restoration.
Prophylactic cefazolin (1 g IV) was administered intraoperatively to minimize infection risk, followed by oral cephalexin (500 mg four times daily for five days). The patient was advised to limit strenuous activity and excessive facial movement for two weeks. Sutures were removed on postoperative day 7, and gentle massage was initiated at three weeks.
At six months postoperatively, the flap remained volumetrically stable. Caliper measurements demonstrated correction within 1 mm of the contralateral side, and three-dimensional photographic analysis confirmed a 91% restoration of the preoperative volume deficit. The patient reported high satisfaction, rating her outcome as 9/10 on a visual analogue scale. The Patient and Observer Scar Assessment Scale (POSAS) yielded excellent scar quality scores of 12/60 (patient assessment) and 9/60 (observer assessment). No complications were observed (Figure 5B, Figure 6). Given the limited existing data on long-term outcomes of CFF reconstruction in ECDS, annual follow-up visits were scheduled to assess sustained flap viability and aesthetic stability.
Six-month postoperative oblique view confirming volume maintenance and symmetry
Discussion
This case demonstrates the feasibility and favorable outcomes achievable through the use of a vascularized CFF for mandibular contour restoration in a patient with stable ECDS. Although various reconstructive methods have been described to address soft tissue atrophy in ECDS, each carries trade-offs related to invasiveness, durability, and predictability. To our knowledge, this is the first report describing the application of a pedicled CFF specifically for this indication.
Autologous fat grafting remains the most commonly employed technique due to its simplicity, repeatability, and tissue compatibility. However, unpredictable graft resorption often necessitates multiple procedures to achieve satisfactory symmetry [8,9]. Dermal fillers, such as HA, represent minimally invasive alternatives offering immediate aesthetic results; however, their temporary nature and risk of foreign-body granulomatous reactions limit their long-term utility [10,11]. Botulinum toxin can effectively address dynamic asymmetry but provides no volumetric restoration [5].
More invasive methods, including tissue expansion, free flaps, and bone grafting, can adequately correct larger or more complex deformities but are technically demanding and carry significant risks of morbidity [13,14]. Alloplastic implants and bone cement offer durable structural solutions but pose substantial risks of infection, extrusion, and aesthetic mismatch [12]. A recent review of 39 ECDS patients reported that autologous fat grafting was utilized in 41% of cases, surgical reconstruction in 18%, and implants in 10% [5]. This discussion integrates established methods with recent clinical reports, such as patient-level outcomes detailed by Skorochod et al. [6] and the combined fat graft and demineralized bone matrix series presented by Menkü Özdemir et al. [8], thus positioning the CFF within contemporary reconstructive approaches. A comparative summary of these techniques is outlined in Table 1.
The CFF occupies a unique intermediate position, combining the advantages of minimal invasiveness and durability. As a pedicled, vascularized flap harvested from adjacent adipose tissue, it provides reliable perfusion, anatomical compatibility, and minimal donor-site morbidity, all achievable through a single-stage procedure. The concept of utilizing local submental fat tissue for chin augmentation was first described by Robertson in 1965, who developed a double CFF with preserved blood supply for chin enhancement [15]. Later, Hamra expanded on techniques for addressing the aging chin through mentalis-periosteal flap advancement [16]. Our application adapts these foundational concepts specifically for facial volume restoration in ECDS, preserving the key principle of vascular integrity while tailoring the approach to address the unique challenges of localized scleroderma.
The submental region is richly vascularized by branches of the facial artery, specifically the submental and mental arteries (Figure 7) [17]. In our patient, the flap was elevated within a submuscular plane, carefully preserving facial musculature. It was inset without tension and securely anchored to the periosteum. At six months postoperatively, the flap demonstrated stable volume retention with 91% restoration confirmed by three-dimensional photographic analysis, and patient satisfaction was excellent.
Schematic illustration of flap perfusion anatomyThe submental region receives blood supply from the FA and its branches: SMA, ILA, and MA. The lateral pedicle preserves vascular continuity during CFF elevation.CFF, chin fat flap; FA, facial artery; ILA, inferior labial artery; MA, mental artery; SMA, submental artery
Compared to fat grafting, the inherent vascularity of the CFF may reduce resorption and enhance long-term volume retention. Unlike free flap procedures, the CFF eliminates the need for microsurgical expertise and significantly shortens operative time. Moreover, aligning the flap with the natural mentolabial groove resulted in inconspicuous scarring and a harmonious aesthetic transition, validated by favorable POSAS scores. Although additional contouring procedures such as autologous fat grafting, HA, or dermal fillers were not indicated at this stage due to the excellent initial results and sustained volume retention, these adjunctive treatments were discussed with the patient preoperatively and at follow-up visits as options should residual or future contour discrepancies emerge. The reliable vascularization of the CFF provided distinct advantages over fat grafting alone, particularly in maintaining stable volume and reducing the need for repeated interventions.
While this is a single case report and therefore has limited statistical generalizability, we incorporated objective and semi-objective assessments where appropriate. These included caliper-based thickness comparison, validated scar scoring using POSAS, and a patient-reported visual analogue scale rating for satisfaction. Future studies may benefit from incorporating additional tools such as magnetic resonance imaging for volumetric monitoring and the Facial Appearance-Related Psychosocial Impact Questionnaire (FACE-Q) to standardize patient-reported aesthetic and quality-of-life outcomes.
PRS, which shares overlapping clinical characteristics with ECDS, has been similarly addressed using local volume augmentation techniques [18]. Despite differences in etiology, both conditions may benefit substantially from autologous, vascularized soft tissue reconstruction.
While the procedure was performed under GA in this study, the limited operative field and minimal dissection suggest it could alternatively be performed under local anesthesia (LA) with appropriate nerve blocks, potentially offering reduced recovery time and hospital stay for suitable candidates.
This approach is best suited for moderate-volume defects in patients with adequate submental adiposity. However, it may be inappropriate for cases with extensive or multi-zone facial atrophy. Short-term results were favorable, but the absence of longer-term follow-up and the limitation of this single-case report restrict the generalizability of the findings. Further studies involving larger cohorts and prolonged observation periods are necessary to validate the technique’s durability, refine patient selection criteria, and assess long-term aesthetic and functional outcomes.
Conclusions
This case demonstrates the clinical utility of the vascularized CFF as an effective and underutilized option for mandibular soft tissue reconstruction in stable ECDS. The single-incision technique enables reliable volume restoration using adjacent, vascularized tissue, minimizing morbidity and eliminating the need for implants or microsurgery. Our patient achieved over 90% volumetric restoration, excellent scar quality, and high satisfaction at six months.
The CFF is best suited for moderate-volume defects in patients with adequate submental fat and may be feasible under LA. While early outcomes are promising, further studies with larger cohorts and longer follow-up are necessary to confirm durability and define optimal indications. This report supports the CFF as a valuable addition to the reconstructive armamentarium for facial atrophy in ECDS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Localized scleroderma: clinical spectrum and therapeutic update An Bras Dermatol Careta MF Romiti R 627390201510.1590/abd 1806-4841.20152890 PMC 432370025672301 · doi ↗ · pubmed ↗
- 2Progressive hemifacial atrophy and linear scleroderma en coup de sabre: a spectrum of the same disease?Front Med (Lausanne) Khamaganova I 258420172944572610.3389/fmed.2017.00258 PMC 5798413 · doi ↗ · pubmed ↗
- 3Clinical characteristics and comorbidities of patients with localized scleroderma: a retrospective study of 78 patients Exp Ther Med Mititelu M Badea I Danciu M Dobre M 969222021
- 4Pediatric morphea (localized scleroderma): review of 136 patients J Am Acad Dermatol Christen-Zaech S Hakim MD Afsar FS Paller AS 3853965920081857176910.1016/j.jaad.2008.05.005 · doi ↗ · pubmed ↗
- 5Therapeutic and reconstructive management options in scleroderma (morphea) en coup de sabre in children and adults. A systematic literature review J Clin Med Ulc E Rudnicka L Waśkiel-Burnat A Warszawik-Hendzel O Niemczyk A Olszewska M 45171020213464053310.3390/jcm 10194517 PMC 8509267 · doi ↗ · pubmed ↗
- 6Management options for linear scleroderma (“en coup de sabre”)Dermatol Surg Skorochod R Nesher G Gronovich Y 103810454820223598500910.1097/DSS.0000000000003539 · doi ↗ · pubmed ↗
- 7Evaluation and treatment of pediatric localized scleroderma: pearls and updates Curr Treat Options in Rheum Glaser D Torok KS 12072021
- 8Treatment of en coup de sabre deformity with fat grafting and demineralized bone matrix: a case series J Plast Reconstr Aesthet Surg Menkü Özdemir FD Üstün GG Vargelİ Özgür FF 335333607420213441712610.1016/j.bjps.2021.05.038 · doi ↗ · pubmed ↗