A Stable Switch From Bictegravir/Emtricitabine/Tenofovir Alafenamide (B/FTC/TAF) to Dolutegravir/Lamivudine (DTG/3TC) in the Absence of Historical Resistance Records: Results From the Switch to Dovato in Patients Suppressed on Biktarvy (SOUND) Cohort
Jihad Slim, Paul Bellafiore, Masara Touza, James P Fallon, Rebecca A Borsi

TL;DR
This study shows that switching HIV patients from B/FTC/TAF to DTG/3TC is safe and effective, even without prior resistance records, and may help reduce weight.
Contribution
Demonstrates the safety and efficacy of switching to DTG/3TC in HIV patients without historical resistance data.
Findings
0% of participants had a viral load ≥50 c/mL at week 48 after switching regimens.
No participants discontinued due to safety concerns or lab abnormalities.
A significant decrease in weight was observed during the study period.
Abstract
Objective: This article aims to examine the safety and efficacy of switching from bictegravir/emtricitabine/tenofovir alafenamide (B/FTC/TAF) to dolutegravir and lamivudine (DTG/3TC) in the absence of prior resistance records. Design: Switch to Dovato in patients suppressed on Biktarvy (SOUND) is an open-label, single-arm, pilot study of adult people with HIV who were virologically suppressed (HIV-1 <50 copies/mL) on B/FTC/TAF for >24 weeks, and switched to DTG/3TC in the absence of available resistance records. Methods: The primary endpoint was the percentage of participants with HIV viral load (VL) ≥50 c/mL at week 48. Secondary endpoints at weeks 48 and 96 included the percentage of participants with HIV-VL <50 c/mL, incidence and severity of adverse events, laboratory abnormalities, change in baseline CD4 cell count, and retrospective proviral DNA resistance testing on banked…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
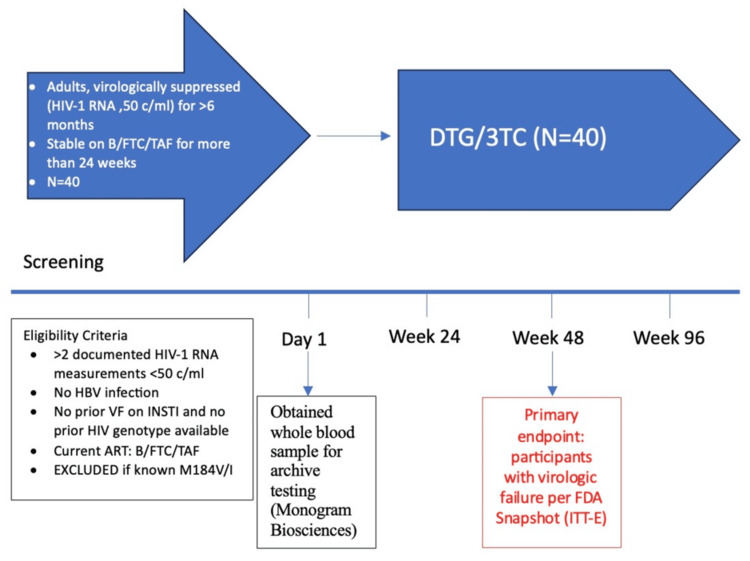 Figure 1
Figure 1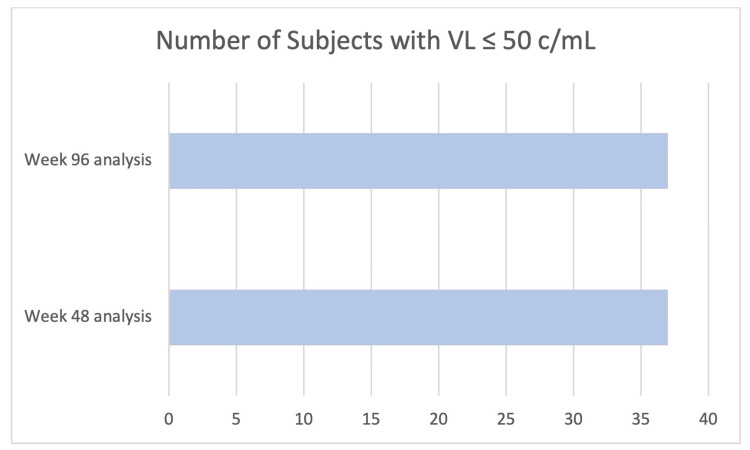 Figure 2
Figure 2| Characteristic | Values (n = 40) |
| Male, n (%) | 22 (55%) |
| Female, n (%) | 18 (45%) |
| Black, n (%) | 23 (57.5%) |
| Hispanic, n (%) | 12 (30%) |
| Caucasian, n (%) | 4 (10%) |
| Other, n (%) | 1 (2.5%) |
| Median age (range) | 58 years (27-81) |
| Mean weight (range) | 87.7 kg (46-131) |
| Median time on B/FTC/TAF (range) | 2.75 years (1-3.6) |
| Median time virologically suppressed prior to study entry (range) | 7.5 years (0.6-14.2) |
| Median time since HIV diagnosis (range) | 16.4 years (1.2-36) |
| Median number of ART regimens prior to enrollment (range) | 5 (1-14) |
| Median baseline CD4 count (range) | 681 cells/mm3 (372-1,044) |
| Median nadir CD4 count (range) | 364 cell/mm3 (13-734) |
| Proviral DNA testing, n (%) | |
| NRTI | 6 (19%) |
| M184I/V | 6 (19%) |
| INSTI | 2 (6%) |
| S147S/G | 1 (3%) |
| Q148Q/R | 1 (3%) |
| NNRTI | 8 (25%) |
| K103K/N | 6 (19%) |
| PI | 3 (9%) |
| D30D/N | 2 (6%) |
| N88S | 1 (3%) |
| N88N/S | 1 (3%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS drug development and treatment · HIV Research and Treatment · Hepatitis C virus research
Introduction
Current treatment guidelines for the treatment of HIV recommend two- or three-drug integrase strand transfer inhibitor (INSTI)-based therapy commonly prescribed at single-table regimens (STR) [1]. Potential advantages of using fewer drugs in an STR can be fewer drug-drug interactions, reduction in the risk of adverse events (AEs), polypharmacy, and a decrease in the cost of antiretroviral therapy (ART), all without compromising virologic suppression (VS) [2,3]. Previous studies have demonstrated that approved two-drug STRs are noninferior to three-drug STRs in terms of viral suppression for appropriate patients [4-7].
Two commonly used STRs are dolutegravir and lamivudine (DTG/3TC) and bictegravir/emtricitabine/tenofovir alafenamide (B/FTC/TAF). Potential barriers to using DTG/3TC include a patient's hepatitis B status and concerns about nucleoside reverse transcriptase inhibitor (NRTI) resistance, specifically the M184V mutation [8]. While this mutation is rare (about 1%) in people with HIV (PWH) naïve to treatment in the US, it is not uncommon to find it upon virologic failure (VF) in those on 3TC or FTC-containing regimens (as high as 80%) [9-11].
We were therefore interested in studying whether patients switching from B/FTC/TAF to DTG/3TC would maintain VS when prior resistance testing was not available.
Materials and methods
Switch to Dovato in patients suppressed on Biktarvy (SOUND) is an open-label, single-arm, pilot study of adult PWH who were virologically suppressed (HIV-1 <50 copies/mL) on B/FTC/TAF and switched to DTG/3TC in the absence of available resistance records. Participants were enrolled from March 2021 to March 2022. The Saint Michael’s Medical Center Institutional Review Board approved the study, and all participants provided written consent before screening.
Participants >18 years of age who were VS on B/FTC/TAF for >24 weeks and had no available resistance testing results were eligible. Participants who had VF in the past were eligible, provided they were VS at enrollment according to the above protocol. Major exclusion criteria were a positive hepatitis B surface antigen, creatinine clearance <30 mL/minute/1.73 m^2^, or severe hepatic impairment (alanine aminotransferase greater than five times the upper limit of normal).
A whole blood sample for archive testing (Monogram Biosciences, South San Francisco, CA) was drawn on Day 1 before dispensing DTG/3TC to the participant (Figure 1). Participants were assessed for safety and efficacy through a physician visit and laboratory tests at weeks 4 and 12, and every 12 weeks thereafter, up to week 96. Vital signs, weight, hematology panel, chemistry panel, HIV viral load (VL), and CD4 T-cell counts were performed at every scheduled study visit. A fasting lipid profile was performed on Day 1 and at weeks 24, 48, 72, and 96.
Open-label, single-center, single-arm pilot study designDTG: dolutegravir; 3TC: lamivudine; HBV: hepatitis B virus; VF: virologic failure; B/FTC/TAF: bictegravir, emtricitabine, and tenofovir alafenamide; ITT-E: intention to treat exposed; INSTI: integrase strand transfer inhibitor; ART: antiretroviral therapy
End points
The primary endpoint was the percentage of participants with an HIV-VL ≥50 copies/mL at week 48 using FDA intention-to-treat snapshot analysis. Secondary endpoints at weeks 48 and 96 included the percentage of participants with HIV-VL <50 copies/mL using FDA snapshot, incidence and severity of AEs, percentage of subjects who discontinued treatment due to AEs, laboratory abnormalities, change in baseline CD4 cell count, and retrospective proviral DNA testing on banked samples to compare virologic outcome for study participants (those with vs. without baseline M184I/V mutations). VF was defined as plasma HIV-1 ≥50 copies/mL confirmed by a retest plasma HIV-1 ≥200 copies/mL performed in three to four weeks.
Statistics
Participants who received at least one dose of DTG/3TC were included in the primary and secondary analyses. Basic descriptive statistics were used to analyze the demographic and baseline characteristics. AEs, significant AEs (SAEs), withdrawals, and virologic response were summarized.
Results
Efficacy
Of the 40 individuals enrolled who switched to DTG/3TC, 0 (0%) had a VL ≥50 c/mL at week 48; 37 (93%) remained virologically suppressed (HIV-1 RNA <50 c/mL) at the same time point. Three participants withdrew through week 48 and were virologically suppressed at the time of discontinuation. One participant withdrew due to becoming pregnant, and two withdrew due to a preference for B/FTC/TAF. At week 96, all 37 participants maintained VS (HIV-1 RNA <50 c/mL), with no new discontinuations since the 48-week analysis (Figure 2).
Results for secondary endpointsVL: viral load
Resistance
Forty participants had baseline samples drawn; however, 32 were available for retrospective proviral DNA resistance testing. Three patients withdrew from the study, two sample tubes cracked during transport, two samples could not be located, and one sample could not be analyzed. Six (19%) had NRTI resistance-associated mutations (RAMs), all of which harbored the M184I/V mutation. Two (6%) participants had INSTI RAMs at baseline (S147S/G and Q148Q/R), conferring resistance to raltegravir or elvitegravir; nonnucleoside reverse transcriptase inhibitor and protease inhibitor RAMs were observed in eight (25%) and three (9%) participants (Table 1). Mutations were not mutually exclusive.
Safety
No participants discontinued due to laboratory abnormalities or safety-related concerns. Median change from baseline in CD4+ cell count at week 96 was 38 cells/mm^3^. Thirty-four participants experienced one or more AEs while on treatment with DTG/3TC for a total of 81 events, none of which were Grade 3 or 4. The most common AEs included fatigue, headache, fever, viral illness, upper respiratory infection, abdominal pain, joint pain, muscle pain, and loose stool. Five participants accounted for a total of six SAEs. SAEs reported were endometrial cancer, symptomatic anemia, hiatal hernia, pulmonary nodule, acute pyelonephritis, and dizziness. The glomerular filtration rate, creatinine, and fasting lipid profiles remained stable for over 96 weeks. Weight loss was observed at weeks 48 and 96, with an average decrease in weight of 3.3 kg from baseline (range: -24 to +6 kg) in post hoc analysis.
Discussion
In this pilot trial, DTG/3TC was effective, with no PWH having an HIV-1 RNA ≥50 copies/mL at week 48 in the setting of unknown resistance. Furthermore, VS was maintained at the secondary endpoint, week 96. The presence of archived resistance, including M184I/V, did not affect viral suppression or lead to VF. Additionally, after two years of follow-up, no cases of treatment-emergent INSTI resistance were reported.
Several studies have demonstrated the efficacy of switching to DTG/3TC from a stable ART regimen through 48 weeks [12]. In the DYAD study, participants were randomized to either stay on B/FTC/TAF or switch to DTG/3TC; it was found that DTG/3TC was noninferior through 48 weeks [3]. The PASO DOBLE study also demonstrated noninferiority of DTG/3TC compared to B/FTC/TAF when switching from a stable regimen [13]. Our study, although smaller than the previously mentioned studies, provides efficacy data for DTG/3TC through 96 weeks.
Despite evidence supporting the efficacy of DTG/3TC, concerns about VF due to resistance remain. Some studies have reported efficacy data even in the absence of baseline resistance testing. In the DYAD study, for example, 44% of participants who were virologically suppressed on B/FTC/TAF and were switched to DTG/3TC had no genotype available at baseline, and DTG/3TC still performed well [3]. Of note, one case of M184M/I together with an INSTI secondary mutation (G140G/S, treatment-emergence unknown) was reported in the B/FTC/TAF arm [3]. In the SOLAR-3D trial, 100 participants, 50 with known MI84I/V and 50 without resistance testing at baseline, were evaluated for the efficacy of DTG/3TC at 48 weeks and found no cases of VF [4]. A meta-analysis investigating a stable switch to DTG/3TC in the presence of preexisting M184I/V mutations demonstrated that switching to DTG/3TC was effective in maintaining VS in patients with archived M184I/V mutations and found no cases of treatment-emergent INSTI resistance, even in the presence of historical or current M184V/I mutations, which is aligned to the results we report here [14].
Another important finding from this trial is the trend toward a decrease in weight from baseline. At two years, participants decreased their weight by 7.1 lbs (3.2 kg) without using other weight loss modalities. Since this was a single-arm study, we do not have a comparative arm; however, it is consistent with the PASO DOBLE study, which shows significantly less weight gain in suppressed PWH switching to DTG/3TC compared to switching to B/FTC/TAF. A similar finding was reported in the DRAGON study, which compared weight changes in treatment-naive Asian PWH who initiated either DTG/3TC or B/FTC/TAF [15]. The difference in the adjusted mean weight from baseline to week 48 in the DTG/3TC group was smaller than that observed in the B/FTC/TAF group; this finding is consistent with the results reported here [15]. In the previously mentioned DYAD study, there was no significant weight difference between those who switched to DTG/3TC compared to those who continued on B/FTC/TAF at 48 weeks. However, this could be due to the presence of a colocated weight loss health center.
The strengths of the SOUND study include its high percentage of Black (55%) and female (45%) participants, which adds to the diversity of the study population. Additionally, the study provides valuable data on the prevalence of RAMs and their impact on treatment outcomes. However, the study's limitations include its single-center, nonrandomized, single-arm design, which may limit the generalizability of the findings.
Conclusions
In summary, the SOUND study supports the efficacy and safety of switching to DTG/3TC for people living with HIV-1 who are virologically suppressed on B/FTC/TAF with unknown resistance history. It also supports other studies' data, suggesting less weight gain with DTG/3TC compared to B/FTC/TAF. The study's findings are consistent with other real-world and interventional trials, providing additional evidence for the use of DTG/3TC in diverse populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Single tablet HIV regimens facilitate virologic suppression and retention in care among treatment naïve patients AIDS Care Hemmige V Flash CA Carter J Giordano TP Zerai T 101710243020182947832910.1080/09540121.2018.1442554 PMC 6094383 · doi ↗ · pubmed ↗
- 2The cost-effectiveness and budget impact of 2-drug dolutegravir-lamivudine regimens for the treatment of HIV infection in the United States Clin Infect Dis Girouard MP Sax PE Parker RA 7847916220162665805310.1093/cid/civ 981PMC 4772845 · doi ↗ · pubmed ↗
- 31603. Efficacy, safety and tolerability of switching to dolutegravir/lamivudine in virologically suppressed adults living with HIV on bictegravir/emtricitabine/tenofovir alafenamide -the DYAD study Open Forum Infect Dis Rolle CP Castano J Nguyen V Hinestrosa F De Jesus E 010202310.1093/ofid/ofae 560PMC 1148200839416993 · doi ↗ · pubmed ↗
- 4No confirmed virological failures (CVF) for 144 weeks when switching 2-/3-/4-drug ART to DTG/3TC in heavily treatment-experienced PLWHA with prior M 184V/I and multiple virological failures in the prospective SOLAR-3D study International AIDS Society Conference 10 2024 Blick G. Cerreta-Dial E. Mancini G. 2024 https://www.natap.org/2024/IAS/IAS_01.htm
- 5Impact of the M 184V resistance mutation on virological efficacy and durability of lamivudine-based dual antiretroviral regimens as maintenance therapy in individuals with suppressed HIV-1 RNA: a cohort study Open Forum Infect Dis Gagliardini R Ciccullo A Borghetti A 05201810.1093/ofid/ofy 113PMC 601642229977967 · doi ↗ · pubmed ↗
- 6Efficacy and tolerability of lamivudine plus dolutegravir as a switch strategy in a multicentre cohort of patients with suppressed HIV-1 replication. [Online ahead of print]HIV Med Borghetti A Baldin G Lombardi F 201810.1111/hiv.1261129573320 · doi ↗ · pubmed ↗
- 7Durable efficacy of dolutegravir plus lamivudine in antiretroviral treatment-naive adults with HIV-1 infection: 96-week results from the GEMINI-1 and GEMINI-2 randomized clinical trials: erratum J Acquir Immune Defic Syndr 084202010.1097/QAI.0000000000002275 PMC 704372931834000 · doi ↗ · pubmed ↗
- 8Dovato 10 2024 2019 https://gskpro.com/content/dam/global/hcpportal/en_US/Prescribing_Information/Dovato/pdf/DOVATO-PI-PIL.PDF