Frailty influences clinical outcomes in critical patients: a post hoc analysis of the PalMuSIC study
Ana Mestre, Rodrigo Afonso, André Ferreira-Simões, Iuri Correia, João Gonçalves Pereira

TL;DR
Frailty increases mortality in ICU patients, with longer stays worsening outcomes, especially for those who are frail.
Contribution
This study demonstrates that frailty significantly affects both hospital and 6-month mortality in ICU patients.
Findings
Frail patients had higher hospital and 6-month mortality rates compared to nonfrail patients.
Longer ICU stays were associated with worse long-term outcomes, particularly in frail patients.
Abstract
Frailty is a multidimensional syndrome characterized by diminished physiological reserve, increasing the risk of adverse outcomes, particularly in intensive care unit patients. The Clinical Frailty Scale, ranging from 1 (nonfrail) to 9 (terminally ill), is widely used to quantify frailty. This post hoc analysis of the Palliative Multicenter Study in Intensive Care (PalMuSIC) assesses the impact of frailty and clinical severity on short- and long-term outcomes. This subanalysis involved 23 Portuguese intensive care units and 335 patients. Patients admitted between March 1 and May 15, 2019, aged ≥ 18 years, and hospitalized for > 24 hours in the intensive care unit were eligible. The severity of illness was assessed using SAPS II, and frailty was assessed using the clinical frailty scale, which was recorded by a nurse and a doctor in charge. Patients were classified as frail (clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
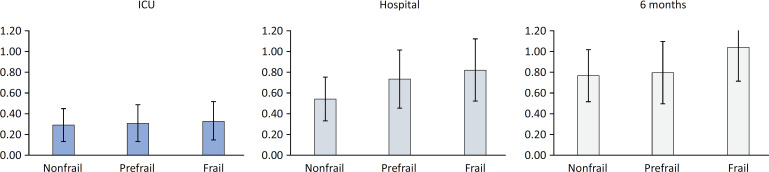 Figure 1
Figure 1| Total | Frail | Prefrail | Nonfrail | p value | |
|---|---|---|---|---|---|
| Patients | 335 | 77 (23.0) | 85 (25.4) | 173 (51.6) | |
| Male | 221 (66.0) | 52 (67.5) | 49 (57.6) | 120 (69.4) | 0.166 |
| Age | 63.2 ± 16.8 | 71.5 ± 12.8 | 68.4 ± 13.1 | 56.9 ± 17.5 | < 0.001 |
| ICU LOS | 5 [7] | 5 [8] | 5 [6.5] | 6 [9.5] | 0.765 |
| SAPS II | 41.8 ± 17.4 | 50.0 ± 17.4 | 45.7 ± 16.0 | 36.3 ± 16.1 | < 0.001 |
| Infection | 201 (60) | 46 (59.7) | 48 (56.5) | 107 (61.8) | 0.731 |
| IMV | 214 (63.9) | 50 (64.9) | 59 (69.4) | 105 (60.7) | 0.382 |
| NIV | 57 (17.0) | 15 (19.5) | 20 (23.5) | 22 (12.7) | 0.076 |
| RRT | 48 (14.3) | 17 (22.1) | 15 (17.6) | 16 (9.2) | 0.017 |
| Vasopressors | 185 (55.2) | 48 (62.3) | 50 (58.8) | 87 (50.3) | 0.155 |
| Previous hospital admission (3 months) | 75 (22.4) | 27 (35.1) | 18 (21.2) | 30 (17.3) | 0.08 |
| Hospital readmission (6 months) | 74 (28.9) | 22 (46.8) | 22 (36.1) | 30 (20.3) | < 0.001 |
| N | Hospital mortality | 6-month mortality | |
|---|---|---|---|
| Nonfrail | 173 | 24 (11.8) | 34 (15.6) |
| Prefrail | 85 | 24 (28.2) | 26 (30.6) |
| Frail | 77 | 30 (39.0) | 38 (49.4) |
| Hospital mortality | 6-month mortality | |||||
|---|---|---|---|---|---|---|
| Short stay (N = 172) | Long stay (N = 163) | OR (95%CI) | Short stay (N = 172) | Long stay (N = 163) | OR (95%CI) | |
| Nonfrail (N = 173) | 9 (10.3) | 12 (17.4) | 1.8 (0.8 - 4.4) | 13 (14.9) | 17 (24.4) | 1.8 (0.9 - 4.0) |
| Prefrail (N = 85) | 10 (20.8) | 11 (37.8) | 2.3 (0.9 - 6.1) | 11 (22.9) | 12 (40.5) | 2.3 (0.9 - 5.8) |
| Frail (N = 77) | 10 (27.0) | 20 (50.0) | 2.7 (1.0 - 7.0) | 13 (35.1) | 25 (62.5) | 3.1 (1.2 - 7.8) |
| p | p | p | p | |||
| Hospital mortality | p value | ||
|---|---|---|---|
| OR | 95%CI | ||
| Prefrail | 1.41 | 0.69 - 2.90 | 0.35 |
| Frail | 1.91 | 0.93 - 3.92 | 0.08 |
| 6-month mortality | |||
| ICU LOS | 1.02 | 1.00 - 1.04 | 0.023 |
| Prefrail | 1.05 | 0.54 - 2.07 | 0.883 |
| Frail | 2.14 | 1.11 - 4.11 | 0.023 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFrailty in Older Adults · Intensive Care Unit Cognitive Disorders · Cardiac, Anesthesia and Surgical Outcomes
INTRODUCTION
Frailty is a complex and multidimensional syndrome characterized by diminished physiological reserve, increasing the risk of poor outcomes for patients.^(1)^ It is a condition of vulnerability that reduces the ability to adapt to an external insult or recover after acute illness. The size of the senior population is increasing worldwide, making frailty an increasing concern for healthcare systems. Although frailty is more prevalent in elderly individuals, it is not invariably associated with age and exists among all age groups. Frailty is common in patients admitted to the intensive care unit (ICU), and it is associated with worse outcomes.^(2)^
The Clinical Frailty Scale (CFS) is widely used in the ICU population to quantify frailty. It is a clinical judgment-based assessment tool consisting of a rating scale designed to assess frailty according to physical activity, functional status, chronic illness burden, and cognition. This score uses a scale that ranges from 1 to 9. Scores of 1 to 3 are considered nonfrail; a score of 4 is considered prefrail or vulnerable; scores of 5 to 8 are deemed frail; and a score of 9 indicates terminal illness.^(3)^ The prevalence of frailty in critically ill patients may be as high as 35%,^(4)^ dependent on the type of ICU. Frailty assessed by the CFS is strongly correlated with adverse outcomes.^(3,5)^ Preadmission frailty has been identified as a relevant risk factor in critically ill patients for ICU- and hospital-related mortality, as well as for prolonged ICU hospitalization.^(4,6)^
Clinical severity scores are largely available in the ICU setting and allow the evaluation of different populations’ severity and death probability as surrogates of the quality of care for benchmarketing purposes. Scoring systems, such as the commonly used Simplified Acute Physiology Score (SAPS) II, help to describe ICU populations and interpret outcome measures. The interactions among frailty, severity scores and outcomes are poorly understood.
This study is a post hoc analysis of a multicenter, prospective, observational study, the PALliative MUlticenter Study in Intensive Care (PalMuSIC).^(7)^ We aimed to assess the impact of the interaction between frailty and clinical severity on short- and long-term outcomes. We also wanted to address whether a prolonged ICU length of stay (LOS) may worsen the outcomes of the frail population due to their lower physiological reserve.
METHODS
This is a subanalysis of the PalMuSIC study. The study protocol has been published elsewhere.^(7)^ Briefly, PalMuSIC was a prospective, observational, multicenter study carried out to evaluate the prevalence of frailty in Portuguese ICUs and the use and adequacy of palliative care and invasive interventions.
The study was conducted in 23 Portuguese ICUs and included 335 patients. All patients admitted during a 15-day consecutive period, starting between 1st March and May 2019, aged ≥ 18 years and hospitalized for > 24 hours in the ICU, were considered eligible for inclusion. Written informed consent was obtained from all patients or their representatives.
The severity of illness at admission was assessed according to SAPS II, and frailty was assessed using the CFS. The CFS was independently recorded by the nurse and the doctor in charge. According to the average of these two assessments, all patients were classified as frail (CFS ≥ 5), prefrail (CFS = 4), or nonfrail (CFS < 4). We also asked the family member with the closest relationship to the patient to provide an assessment of the CFS. The ICU and hospital LOSs were calculated, along with the need for organ support (noninvasive or invasive mechanical ventilation, renal replacement therapy, or vasopressors). Infection upon admission or acquired in the ICU was also recorded. Mortality was evaluated at discharge from the hospital and at 6 months after discharge.
Outcomes
We developed a multivariable model to identify risk factors independently associated with hospital mortality and 6-month all-cause mortality. To assess the interaction between a prolonged ICU LOS and frailty, we further divided our population into short and long ICU LOSs according to the median ICU LOS (5 days).
Statistics
The data are summarized as the means ± standard deviations or medians [25 - 75% interquartile ranges (IQRs)] according to the data distribution. Categorical variables are described as N (%). The chi-square test was used to compare categorical variables, while continuous variables were evaluated with Student's t test or the Kruskal—Wallis test, according to the data distribution. Multiple comparisons of variance were assessed with ANOVAs. Odds ratios (ORs) with 95% confidence intervals (95%CIs) were computed. We developed a multivariable model that included comorbidities, the SAPS II score, frailty status and ICU LOS to assess factors independently associated with hospital mortality and 6-month all-cause mortality. The univariate associations of clinically significant variables were assessed for model development. To ensure the inclusion of all clinically significant variables in the model, a p value as high as 0.2 was used for selection. Moreover, if an excluded variable was considered to have a possible influence on the outcome, it was also included in the model. Correlations between all included variables were checked. We arbitrarily used r < 0.3 as a low enough threshold to decrease the risk of significant multicollinearity. For variables that were correlated, the one that was considered more likely to be related to the outcome was selected. Model fit was assessed with the Hosmer—Lemeshow goodness-of-fit test. Statistical analysis was performed using IBM SPSS Statistics v.29.0 (IBM, Somers, NY, USA). All statistics were 2-tailed, and the significance level was p < 0.05.
RESULTS
Demographics
A total of 335 patients were included. The mean age was 63.2 ± 16.8 years, and 66% were male. The mean SAPS II value was 41.8 ± 17.4. The general characteristics of the patients are shown in table 1.
Frailty was observed in 23.0% of patients. Frail, prefrail, and nonfrail patients were significantly different in terms of age and SAPS II score (Table 1).
Mortality and standardized mortality ratio
Frail patients had higher in-hospital mortality rates (39.0% versus 28.2% versus 11.8%; p < 0.001). All-cause mortality after 6 months of follow-up was also significantly greater in frail patients (49.4% versus 30.6% versus 15.6%, p < 0.001) (Table 2).
In addition, frail patients who survived until hospital discharge often needed hospital readmission in the first 6 months, and this number was significantly higher than that of nonfrail patients (Table 1).
In figure 1, we present the standardized mortality ratio (with 95%CI), which was calculated as the ratio between the observed mortality and the SAPS II score-predicted mortality on admission to the ICU. Frailty seemed to impact the standardized mortality ratio, revealing the importance of the case mix on the outcomes.
Standardized mortality ratios, with 95% confidence intervals, calculated at intensive care unit discharge, hospital discharge, and after 6 months of follow-up, revealing the potential influence of frailty on mortality.
Relationship between mortality and time in the intensive care unit
We divided the studied population into two different groups according to the median ICU LOS (5 days): long ICU stay (n = 163, 40 frail) and short ICU stay (n = 172, 37 frail). Significant differences between the two groups were noted: in patients with shorter ICU LOSs, mortality was consistently lower in the hospital and after 6 months of follow-up (Table 3).
However, this difference was more striking in frail patients (Table 3). The ORs for both hospital mortality and 6-month mortality increased from nonfrail to prefrail to frail patients.
Variables associated with mortality
Our multivariable models revealed that the SAPS II score was associated not only with in-hospital mortality but also with 6-month all-cause mortality. The only comorbidity also associated with mortality in our models was heart failure. Curiously, both frailty and ICU LOS were associated with 6-month mortality but not with hospital mortality (Table 4).
DISCUSSION
In this study, we aimed to analyze the relationships between frailty and ICU, hospital, and 6-month mortality. Additionally, we explored the relationship between the ICU LOS and mortality.
Frail patients were significantly older and had higher SAPS II scores, but few differences were observed in patients who needed organ support therapies. Mortality increased with frailty, either ICU, hospital, or 6-month mortality, even after adjusting for severity scores. These differences were especially pronounced in patients with long ICU stays. In addition, the need for hospital readmission in those discharged was much more common in frail patients.
An association between frailty and hospital mortality has been reported in previous studies.^(8,9)^ In our study, frailty was independently associated with 6-month all-cause mortality. Frailty represents a dimension of the patient evaluation that escapes from the severity scores traditionally used in the ICU; therefore, it could complement the SAPS II in assessing patient prognosis.^(10)^
Critical illness is associated with significant disturbances in the homeostasis of each patient, persistent inflammation, and sequelae of dysfunction after hospital discharge.^(11,12)^ Additionally, all invasive interventions during intensive care hospitalization can contribute to patient deterioration, resulting in a predictable negative long-term impact,^(13)^ which is primarily time dependent.^(14)^ Therefore, patients with lower functional reserves, including frail patients, are less tolerant of the persistence of the disease and prolonged hospitalization. This may even be more pronounced in critically ill septic patients.^(15,16)^ In addition, some patients may already present an underrecognized end-of-life trajectory that becomes apparent only during their critical illness.^(17,18)^ We have previously shown^(7)^ that frail patients were commonly treated with invasive organ support therapy and subsequently, provided a DNR order.
Accordingly, an interaction between LOS in the ICU and frailty could be expected. Our study revealed that frailty and longer durations in the ICU were independently associated with long-term mortality but not hospital mortality (Table 4). This finding attests to the potential interaction between frailty and a long ICU stay that influences the risk of a poor outcome.^(19)^ In a recently published study of patients with an ICU LOS ≥ 7 days, frailty strongly influenced 6-month mortality and quality of life.^(19)^ These findings align with our data and those of other previously published studies,^(2,6,20)^ suggesting an independent impact of frailty on outcomes. Our study stands out for its unique analysis of the relationships among frailty, ICU LOS and mortality, revealing that this association is not as evident in patients with a short ICU stay. Not only did patients with longer ICU stays have higher 6-month mortality rates than those with shorter ICU durations, but this difference between long and short ICU LOSs was more pronounced in frail patients: OR (95% CI) for frail patients 3.1 (1.2 - 7.8) versus for nonfrail patients 1.8 (0.9 - 4.0).
Our study has several limitations, mostly due to its relatively small sample size, which limits our conclusions. In addition, we did not address end-of-life decisions after ICU discharge or measure quality of life after hospital discharge, which may have influenced our results.
CONCLUSION
Frailty may influence patient outcomes in the intensive care unit, including short- and long-term mortality. In our cohort, a prolonged intensive care unit length of stay was associated with a worse long-term outcome, especially in frail patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferrante LE Szczeklik W Frailty is crucial in FORECAS Ting outcomes in critical care Intensive Care Med 2024507111911223895392810.1007/s 00134-024-07518-0PMC 11556853 · doi ↗ · pubmed ↗
- 2Muscedere J Waters B Varambally A Bagshaw SM Boyd JG Maslove D The impact of frailty on intensive care unit outcomes: a systematic review and meta-analysis Intensive Care Med 2017438110511222867689610.1007/s 00134-017-4867-0PMC 5501903 · doi ↗ · pubmed ↗
- 3De Biasio JC Mittel AM Mueller AL Ferrante LE Kim DH Shaefi S Frailty in critical care medicine: a review Anesth Analg 20201306146214733238433610.1213/ANE.0000000000004665 PMC 7426653 · doi ↗ · pubmed ↗
- 4Bruno RR Wernly B Bagshaw SM van den Boogaard M Darvall JN De Geer L The Clinical Frailty Scale for mortality prediction of old acutely admitted intensive care patients: a meta-analysis of individual patient-level data Ann Intensive Care 202313137373713379610.1186/s 13613-023-01132-x PMC 10155148 · doi ↗ · pubmed ↗
- 5Hope AA Hsieh SJ Petti A Hurtado-Sbordoni M Verghese J Gong MN Assessing the usefulness and validity of frailty markers in critically ill adults Ann Am Thorac Soc 20171469529592835858410.1513/Annals ATS.201607-538OCPMC 5566304 · doi ↗ · pubmed ↗
- 6Darvall JN Greentree K Braat MS Story DA Lim WK Contributors to frailty in critical illness: multi-dimensional analysis of the Clinical Frailty Scale J Crit Care 2019521931993109610010.1016/j.jcrc.2019.04.032 · doi ↗ · pubmed ↗
- 7Correia I Simas Chaves S Paixão AI Catarino A Gonçalves-Pereira J The PA Lliative M Ulticenter Study in Intensive Care (Pal Mu SIC). Results from a multicenter study addressing frailty and palliative care interventions in intensive care units in Portugal J Palliat Care 20223745525613412843110.1177/08258597211020964 · doi ↗ · pubmed ↗
- 8Graham JE Snih SA Berges IM Ray LA Markides KS Ottenbacher KJ Frailty and 10-year mortality in community-living Mexican American older adults Gerontology 20095566446511969039510.1159/000235653 PMC 2783319 · doi ↗ · pubmed ↗