Erythema Elevatum Diutinum: A Rare Case Wth Atypical Presentation
Karthika Ps, Manimaran R, Koppolu Kanchana, Srinivasan C, Ankita Swarnkar

TL;DR
A 56-year-old woman presented with a rare skin condition, Erythema Elevatum Diutinum, with unusual painful lesions, requiring surgical treatment.
Contribution
This case report highlights an atypical presentation of EED with pain and the use of surgical intervention for symptom management.
Findings
The patient presented with painful EED lesions, unlike the typical painless manifestation.
Surgical removal with skin grafts improved symptoms when medical therapy was ineffective.
The case emphasizes the need for personalized treatment in atypical EED presentations.
Abstract
Erythema elevatum diutinum (EED) is an uncommon, chronic vascular dermatosis characterized by plaques, nodules, and violaceous papules, typically affecting the extensor regions of the arms and legs. Although the etiology remains unclear, associations with autoimmune disorders, infections, and malignancies have been proposed. This case report presents a 56-year-old woman, non-diabetic, with an atypical presentation of EED, featuring painful lesions in contrast to the usual painless manifestations. The patient initially presented with painless nodules two years prior, which later became painful, involving multiple sites such as the hands, feet, knees, and back. Diagnostic evaluations, including histopathological examination, confirmed EED. The atypical pain prompted further investigations, ruling out underlying systemic conditions like arthritis or myositis. The treatment consisted of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
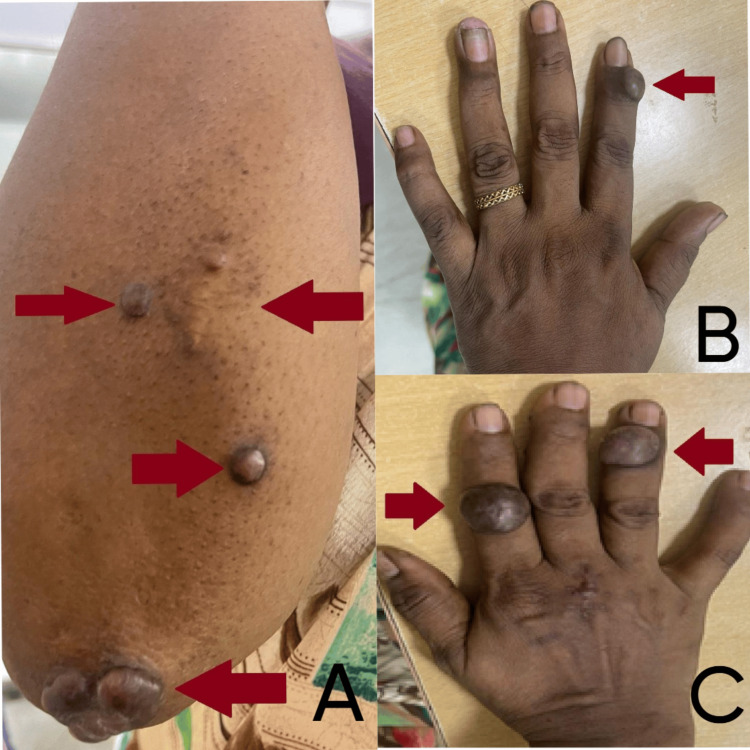 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3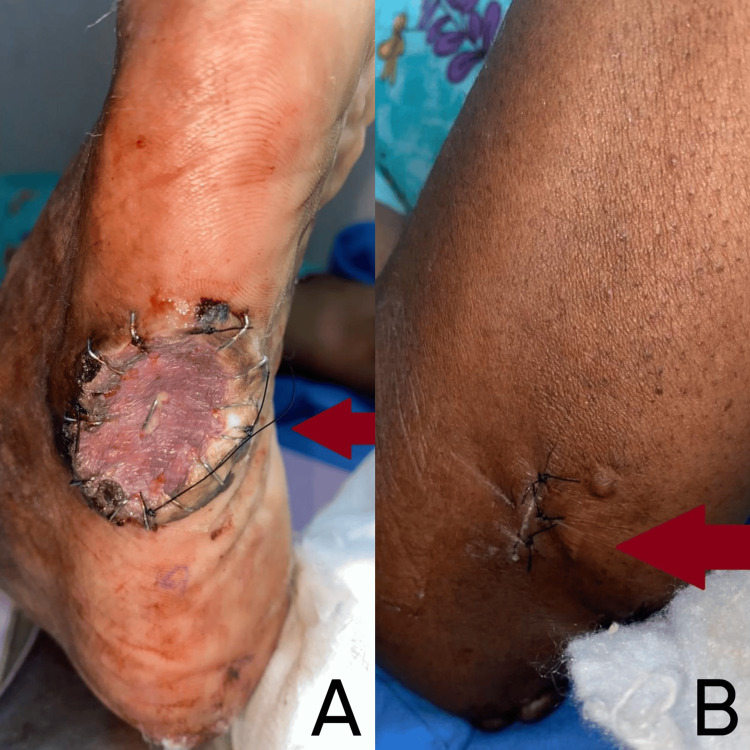 Figure 4
Figure 4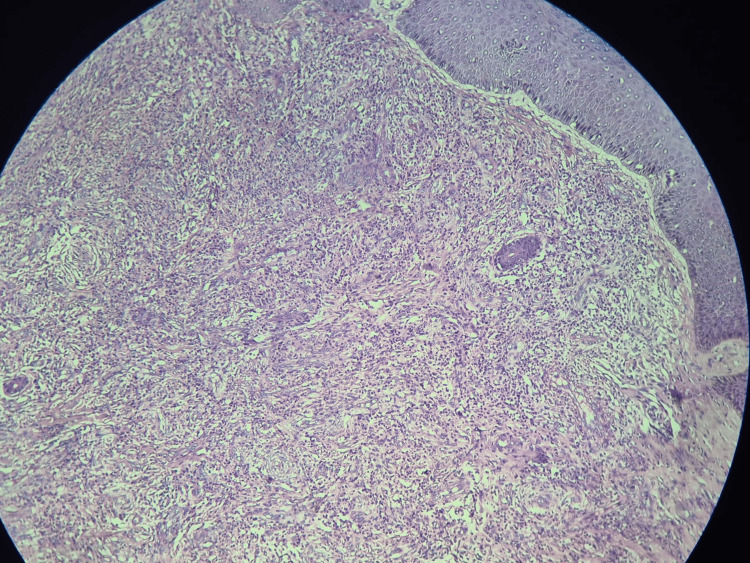 Figure 5
Figure 5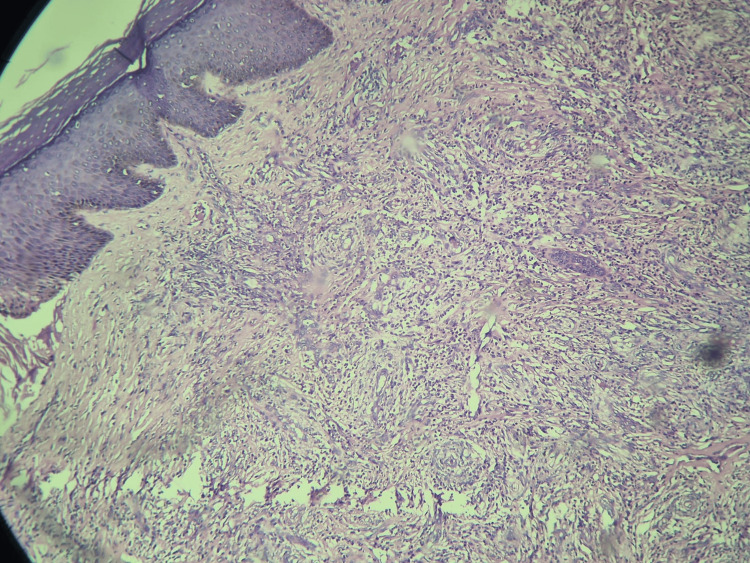 Figure 6
Figure 6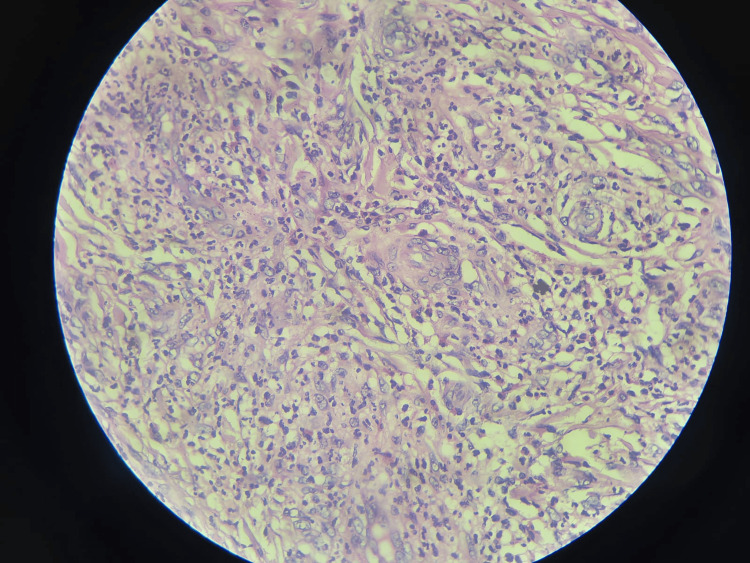 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Autoimmune and Inflammatory Disorders · Chemotherapy-related skin toxicity
Introduction
Erythema elevatum diutinum (EED) is a rare, chronic form of leukocytoclastic vasculitis [1]. This distinctive inflammatory condition presents as persistent violaceous to red brown papular, plaque-like, and nodular lesions, frequently found on extensor surfaces. The symmetric involvement of hands, elbows, knees, and ankles represents the classic presentation, though clinical variations do occur. While epidemiologic studies demonstrate equal gender distribution, emerging evidence suggests a modest male predominance, particularly in patients aged 30-60 years [2]. The pathophysiology of EED remains incompletely understood, though current evidence points to immune complex-mediated vasculitis as the primary mechanism. Histopathologic examination usually shows abundant neutrophils with fibrinoid degeneration of vascular walls [3]. Clinicians should maintain a high index of suspicion for associated systemic conditions, as EED frequently coexists with autoimmune disorders (particularly rheumatoid arthritis and systemic lupus erythematosus, SLE), hematologic abnormalities (notably immunoglobulin (Ig)A paraproteinemia), and chronic infections including HIV and streptococcal pharyngitis [4-6]. Dapsone remains the cornerstone of therapy, exerting its therapeutic effect through neutrophil inhibition [7]. Alternative regimens incorporating colchicine, systemic corticosteroids, or immunomodulators may be considered in refractory cases [8].
The diagnostic challenge intensifies when encountering atypical presentations, whether in morphology, distribution, or symptomatology, as these may closely mimic other inflammatory or rheumatologic conditions [9]. This case presentation underscores the importance of comprehensive evaluation, including histopathologic confirmation, when faced with unusual manifestations of EED. The present case illustrates these diagnostic complexities while highlighting key management considerations for this uncommon entity.
Case presentation
A 56-year-old female patient presented with multiple painful swellings for the past one week involving the back and extremities, which were painless two years back when the patient was presented initially. Routine blood tests, inflammatory markers, erythrocyte sedimentation rate, C-reactive protein, basic metabolic panel, and autoimmune workup were normal when checked initially. Histopathological examination of the skin biopsy confirmed the diagnosis of EED two years ago. On examination, multiple tender, soft swellings, each measuring 2 x 2 cm nodules, were found at the posterior and medial aspect of the right elbow, left hand, and right hand (Figure 1), the medial and lateral aspect of the right foot, and the dorsal and plantar aspect of the left foot. The lesions were hyper- and hypopigmented with intact sensation and a normal range of motion in the joints involved.
Pre-operative images of the patientA. 2 x 2 cm multiple painful nodules on the elbow region, B. 2 x 2 cm painful nodule in the anterior aspect of left index finger, C. 2 x 2 cm painful nodule in the anterior aspect of right index and ring finger.
Pre-operative image of the patient's right foot 2 x 2 cm multiple painful nodules on the lateral part of the right foot.
Anesthesia fitness was obtained. Under aseptic preparation and general anesthesia in supine position, the affected parts were painted and draped. Elliptical incisions were made around the lesion. The incisions were deepened and lesions were excised for biopsy. A split-thickness skin graft was then harvested from thigh and meticulously tailored to fit the raw areas (Figures 3-4). The SSG graft was then placed and secured over the recipient sites. Following surgery, the patient improved well.
Post-operative images of the patientA. Excision with split-thickness skin grafts (SSG) over left index finger, B. Excision with SSG over right index finger, C. Excision with SSG over right ring finger.
Post-operative image of the patients limbsA. Excision with split-thickness skin grafts (SSG) over the right foot, B. Excision with SSG over the elbow region.
The new development of pain in the existing lesions required further investigations. The histopathology report confirmed the diagnosis. Histological features were consistent with erythema elevatum diutinum (Figures 5-7).
Histopathology result image 1Microscopy image shows a lesion with a dermal and perivascular vasculopathy reaction pattern.
Histopathology result image 2Microscopy shows dermal perivascular fibrosis in onion skinning pattern with polymorphous infiltrate of predominantly neutrophils, few lymphocytes, macrophages and occasional eosinophils.
Histopathology result image 3The image shows classic small vessel vasculitis with focal fibrinoid necrosis.
Discussion
Erythema elevatum diutinum (EED) is an uncommon, chronic inflammatory, painless skin lesion that typically presents as violaceous, red-brown, yellow papules, nodules, or plaques that are located on the extensor regions of the limbs, particularly the hands, forearms, elbows, feet, and ankles [10]. The lesions may be asymptomatic or present with pain, burning sensations, or pruritus; these may also ulcerate or form crusts. The course in EED can last for months or even years. While the exact cause of EED remains unknown, some cases may be associated with underlying systemic diseases such as lupus, sarcoidosis, or lymphoma, and autoimmune diseases [11,12]. By understanding the classical presentation, healthcare professionals can better recognize EED and differentiate it from other skin conditions. Atypical EED can present with a variety of features that deviate from the classic presentations, making diagnosis challenging. Here’s a breakdown of some difficulties associated with atypical EED: While typically violaceous, red-brown, or yellow, lesions might exhibit unusual colors or a more uniform hue. EED lesions can be smaller or much larger than the usual 2-5 cm range, potentially mimicking other conditions [13]. Although extensor regions of the limbs are the most common sites, atypical presentations involve less common areas like the trunk, buttocks, or head.
This can lead to confusion with other skin diseases [14]. Atypical EED can be surprisingly painful, which is not a typical characteristic. This pain may mimic other inflammatory skin conditions or lead to misdiagnosis as a musculoskeletal issue. Lesions are often scattered; however, atypical presentations may involve clustered lesions, further adding to diagnostic challenges. This atypical presentation can resemble various other skin conditions, such as sarcoidosis, lupus erythematosus, granuloma annulare, or even bacterial infections. This case report presented an atypical manifestation of EED with painful swelling in the lesions. While the exact cause of pain in EED remains elusive [4], several potential mechanisms might explain the patient's pain experience. Increased inflammatory infiltrates composed of immune cells can release various inflammatory mediators that contribute to pain perception [3]. Large or deeply situated lesions might compress nearby nerves, leading to pain and discomfort [13]. Ulceration of the lesions can expose and irritate nerve endings, causing pain and discomfort for the patient [10]. The differential diagnosis for the patient's pain included underlying joint issues (e.g., arthritis), muscular involvement (myositis), and nerve involvement, all of which could coexist with EED [6,8]. Considering the potential inflammatory nature of EED, analgesics and non-steroidal anti-inflammatory drugs were initiated to manage the patient's pain. Treatment for EED typically involves medications such as dapsone [7,10], colchicine, or corticosteroids, antimicrobials, immunomodulatory agents like methotrexate, cyclophosphamide, antibiotics or antifungals, and treatment of underlying systemic disease [2,9]. This case highlights the diagnostic challenges posed by atypical presentations of EED, such as pain. Despite initial medical treatment, the patient's symptoms persisted, necessitating an excisional biopsy with split-thickness skin grafting (SSG) to improve their quality of life.
Conclusions
Erythema elevatum diutinum is a rare disease in which patients present with skin lesions that are usually painless. In some cases, there are typical symptoms such as pain, which may lead to a diagnostic dilemma. In such scenarios, it is important to reevaluate the patient as a whole and tailor the treatment options for the benefit of the patient. A thorough knowledge of this rare disease and its varied presentations will help in a multimodal approach to the treatment. Finally, the main objective of this report is to bring awareness about the possibility of the occurrence of atypical presentation of EED, such as pain. In the long run, medical treatment of EED might be unsatisfactory and require other treatment modalities. Hence, this patient underscores the importance of close follow-up and interventional procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Erythema elevatum diutinum: a case report and review of literature Int J Dermatol Doktor V Hadi A Hadi A Phelps R Goodheart H 4084155820193007462410.1111/ijd.14169 · doi ↗ · pubmed ↗
- 2Erythema elevatum diutinum: a clinical and histopathologic study of 13 patients J Am Acad Dermatol Yiannias JA El-Azhary RA Gibson LE 3844261992173233410.1016/0190-9622(92)70003-x · doi ↗ · pubmed ↗
- 3Erythema elevatum diutinum a rare and poorly understood cutaneous vasculitis: a single institution experience J Cutan Pathol Sardiña LA Jour G Piliang MP Bergfeld WF 971014620193036215010.1111/cup.13378 · doi ↗ · pubmed ↗
- 4Nodular lesions of erythema elevatum diutinum in patients infected with the human immunodeficiency virus J Am Acad Dermatol Le Boit PE Cockerell CJ 919922281993849645410.1016/0190-9622(93)70130-l · doi ↗ · pubmed ↗
- 5Erythema elevatum diutinum associated with lupus panniculitis in a patient with discoid lesions of chronic cutaneous lupus erythematosus J Am Acad Dermatol Hancox JG Wallace CA Sangueza OP Graham GF 6526535020041503452710.1016/j.jaad.2003.08.016 · doi ↗ · pubmed ↗
- 6Erythema elevatum diutinum with primary Sjögren syndrome associated with Ig A antineutrophil cytoplasmic antibody Br J Dermatol Shimizu S Nakamura Y Togawa Y Kamada N Kambe N Matsue H 73373515920081854730510.1111/j.1365-2133.2008.08676.x · doi ↗ · pubmed ↗
- 7Erythema elevatum diutinum in systemic lupus erythematosus Rheumatol Int Chan Y Mok CC Tang WY 2592623120112065281310.1007/s 00296-010-1574-3 · doi ↗ · pubmed ↗
- 8Erythema elevatum diutinum associated with Hashimoto's thyroiditis and antiphospholipid antibodies J Am Acad Dermatol Yamamoto T Nakamura S Nishioka K 1651665220051562710310.1016/j.jaad.2004.05.029 · doi ↗ · pubmed ↗