Renal cell carcinoma and upper tract urothelial carcinoma in kidney transplant recipients
Oana Moldoveanu, Cătălin Baston, Bogdan Sorohan, Lucas Discalicău, Ioanel Sinescu

TL;DR
This study examines the occurrence and treatment of kidney cancers in people who have received kidney transplants, emphasizing the need for better screening and personalized care.
Contribution
The study provides new insights into the incidence and management of RCC and UTUC in kidney transplant recipients.
Findings
The incidence of RCC was 0.78% and UTUC was 0.087% among kidney transplant recipients.
Surgical interventions and adjusted immunosuppression led to prolonged survival in 25% of patients with metastases.
Localized disease at diagnosis and individualized treatment strategies are critical for optimizing outcomes.
Abstract
Renal cell carcinoma (RCC) is the most common solid-organ malignancy in Western countries, and upper tract urothelial carcinoma (UTUC) is the most common malignancy in Asian countries. The management of RCC/UTUC in kidney transplant recipients is complex and clinically challenging due to post-transplant modifications associated with immunosuppressive treatment. This retrospective study evaluated the incidence, risk factors, treatment outcomes, and oncological implications of RCC and UTUC in kidney transplant recipients from 2008 to 2023. Data were collected from clinical records, and follow-up calls for 20 patients diagnosed with RCC and UTUC among 2,283 kidney transplant recipients, revealing an incidence rate of 0.78% for RCC (18 patients) and 0.087% (two patients) for UTUC. Most patients presented localized disease at diagnosis. Surgical interventions included radical nephrectomy for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
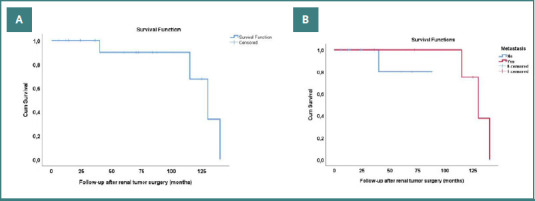 Figure 1
Figure 1| Sex | Age KT | Cause of ESKD | Donor type | Dialysis pre-KT (y) | Risk factors | Age | Diagnostic | Renal tumor location | Type of renal tumor | Graft function | Immunosuppression time before renal tumor (years) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | F | 34 | N | D | 3 | HTA | 54 | Hematuria | G | ccRCC | F | 18 |
| Case 2 | M | 41 | ADPKD | L | 2 | Smoking | 45 | Inflammatory | G | cc-pRCC | Non-F | 5 |
| Case 3 | M | 52 | Obstructive uropathy | D | 10 | HTA | 64 | Hematuria | G | UTUC | F | 10 |
| Case 4 | M | 48 | Glomerulopathy | D | 3 | HTA | 50 | I | NK | ccRCC | Non-F | 1 |
| Case 5 | F | 53 | N | D | 2 | HTA | 60 | I | NK | pRCC | F | 8 |
| Case 6 | M | 28 (1st) | Glomerulopathy | L | 0 | HTA | 42 | I | NK | ccRCC | Non-F | 15 |
| Case 7 | M | 35 | Glomerulopathy | L | 14 | HTA | 42 | I | NK | ccRCC | Non-F | 3 |
| Case 8 | F | 28 | Uropathy | L | 13 | HTA | 51 | I | NK | ccRCC | Non-F | 10 |
| Case 9 | F | 61 | Uropathy | D | 8 | HTA | 63 | Hematuria | NK | ccRCC | F | 3 |
| Case 10 | M | 30 | Glomerulopathy | D | 0 | HTA | 36 | Incidental | NK | pRCC | F | 11 |
| Case 11 | M | 48 | Glomerulopathy | L | 4 | HTA | 49 | I | Bilat. NK | ccRCC | F | 0.4 |
| Case 12 | M | 37 | N | L | 2 | HTA | 50 | I | NK | ccRCC | F | 14 |
| Case 13 | F | 54 | Glomerulopathy | L | 12 | HTA | 64 | Hematuria | NK | ccRCC | F | 10 |
| Case 14 | M | 50 | ADPKD | D | 0 | No | 59 | I | NK | pRCC | F | 9 |
| Case 15 | M | 55 | N | L | 2 | HTA | 67 | Abd. Pain | NK | UTUC | F | 12 |
| Case 16 | M | 44 | N | D | 5 | HTA | 46 | I | NK | ccRCC | F | 2 |
| Case 17 | M | 45 | N | D | 5 | HTA | 47 | I | NK | ccRCC | F | 2 |
| Case 18 | F | 57 | Glomerulopathy | D | 6 | HTA | 58 | I | NK | ccRCC | F | 2 |
| Case 19 | M | 31 | Glomerulopathy | D | 6 | HTA | 47 | I | NK | chRCC | Non-F | 5 |
| Case 20 | M | 60 | Glomerulopathy | D | 5 | HTA | 61 | I | NK | ccRCC | Non-F | 1 |
| Parameter | Value |
|---|---|
| Type of surgery | G-RN 1/20 (5%) |
| Clavien-Dindo complications at the time of surgery | I (14/20, 70%), II (6/20, 30%) |
| RCC stages and grading | pT1a G 2/20(10%) |
| UTUC stages and grading | pT2 LG – native kidney (1/20, 5%) |
| Follow-up | 57.2 months (range 6 to 140 months) |
| Metastasis sites (6 metastatic patients) | Extra-regional LN 1/20 (5%) |
| Cause of death (4 patients died) | Cancer-related death 1/20 (5%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral-associated cancers and disorders · Polyomavirus and related diseases · Bladder and Urothelial Cancer Treatments
INTRODUCTION
Kidney transplant (KT) is the treatment of choice for patients with end-stage kidney disease (ESKD), significantly improving overall survival (OS). KT offers the advantage of a lower complication rate than patients who remain on dialysis [1-3]. Advances in surgical techniques, postoperative care, and the development of new immunosuppressive agents have contributed to longer graft survival and significant improvements in quality of life. However, the risk of developing malignancies remains high in this population [1,4-7]. Renal cell carcinoma (RCC) is the most prevalent solid-organ malignancy, with a 5- to 10-fold higher risk than in the general population, and represents 6.8% of all malignancies in this population [7-9]. In 90% of the cases, RCC is located in the native kidneys, rarely in the kidney graft [7]. Urothelial carcinoma (UC) is typically localized in the bladder, but upper tract urothelial carcinoma (UTUC) of the native kidneys or kidney grafts is less common in Western countries compared to Asia. In Asia, UTUC in native kidneys is the most frequent malignancy following KT [10-16].
Radical nephrectomy or nephroureterectomy remains the treatment of choice for RCC and UTUC in non-functional native kidneys [16-20]. Diagnosing and treating RCC and UTUC in kidney grafts is particularly challenging, as it requires balancing the preservation of renal function with optimal oncologic outcomes. These malignancies in kidney transplant recipients are further complicated by local anatomical changes, transplant-related risk factors, and underlying ESKD-related factors [16-25]. Managing these types of cancers in kidney transplant recipients is a complex process that demands an experienced, multidisciplinary approach to ensure personalized treatment. To date, there are no established guidelines or clear recommendations for the therapeutic management of these patients. This study aimed to examine the incidence, risk factors, surgical outcomes, and survival rates for kidney transplant recipients with RCC and UTUC.
MATERIAL AND METHODS
Study design and participants
This retrospective study evaluated kidney transplant recipients diagnosed with RCC or UTUC in either the native kidneys or the kidney graft between 2008 and 2023. Patient data was collected using the Fundeni Clinical Institute Hipocrate platform, patient record files, and follow-up calls. Inclusion criteria were kidney transplant recipients diagnosed with renal cell carcinoma and upper tract urothelial carcinoma who underwent radical or partial nephrectomy or nephroureterectomy of native kidneys or kidney graft. The functional status of the graft was defined according to the need to initiate dialysis in functional and non-functional grafts. Exclusion criteria were patients diagnosed with post-transplant lymphoproliferative disorder (PTLD) affecting kidneys, patients who did not receive active treatment for RCC or UTUC, patients who received partial or radical nephrectomy or nephroureterectomy for other causes, and patients diagnosed with other types of malignancies pretransplant.
Patient data
Clinical and demographic data collected for this study included age, sex, cause of ESKD, duration of dialysis before transplantation, and presence of acquired cystic kidney disease (ACKD). Additional variables included history of previous kidney transplantation, non-specific pre-transplant risk factors (such as smoking status, hypertension, analgesic exposure, obesity, history of infections, and history of urinary lithiasis), year of transplantation, and donor type. Information regarding the immunosuppressive regimen prior to malignancy diagnosis, graft function status, post-transplant infections, and occurrence of other post-transplant malignancies was also recorded. Data related to the timing and type of surgery for malignancy (radical nephrectomy, partial nephrectomy, or nephroureterectomy), postoperative complications, tumor characteristics (histopathology, staging, and grading), changes in immunosuppression following malignancy, follow-up period, time to metastasis, treatment of metastasis, and time and cause of death were systematically collected for analysis.
Outcomes
The primary endpoint of the study was overall survival, defined as the time from the date of surgery for RCC or UTUC to the date of death or the last follow-up before June 1, 2024. Overall survival at over 10 years of follow-up was evaluated using Kaplan–Meier survival analysis.
RESULTS
Between 2008 and 2023, among 2,283 patients who underwent kidney transplantation, twenty-one recipients were diagnosed with RCC or UTUC. One patient was excluded due to refusal of nephrectomy for a cT3aN1M1 RCC (low-volume pulmonary metastasis) of the left native kidney with functional kidney graft. Twenty patients were included in the study. Among them, three patients (15%) were diagnosed with kidney graft tumors (one patient with RCC on functional graft, one patient with RCC in low functional graft, and one patient with allograft UTUC), and 17 (85%) patients with native kidney tumors (one patient with bilateral RCC, one patient with unilateral UTUC).
Most patients diagnosed with RCC post-KT were men (14 out of 20, 70%). The mean age of kidney transplant recipients was 45.55 years (range 28–61). Most kidney grafts were obtained from deceased donors (13/20, 65%). One patient (5%) developed RCC following a second transplant from a living donor. None of the deceased or living donors had a history of malignancy, and no living donor subsequently developed urologic or other types of malignancies.
The mean age of developing renal tumor after KT was 52.65 years (51.22 years for RCC and 65.5 years for UTUC). The evaluated risk factors are presented in Table 1. The mean dialysis time before KT was 5.1 years (range 0 to 14 years). Eight patients presented ACKD prior to KT and developed RCC in native kidneys (8/16, 50%). Immunosuppression regimens included calcineurin inhibitors for all patients. The mean time of immunosuppression was 7.07 years (range 3 months to 18 years). Six patients were diagnosed with RCC in native kidneys with non-functional grafts at the time of diagnosis (6/16, 37.5%), and one patient was diagnosed with RCC in a non-functional transplanted kidney (1/3, 33.33%). Both patients with UTUC had functional grafts at the time of malignancy detection.
Surgical aspects
A retroperitoneal open radical nephrectomy was performed for most cases of RCC in native kidneys (15/20 patients, 75%). In one case of bilateral RCC, a laparoscopic simultaneous bilateral nephrectomy was performed (5%). For RCC involving the kidney allograft, retroperitoneal transplantectomy was performed in one patient (Case 2) and open partial nephrectomy in another (Case 1). In the case of UTUC involving the kidney graft (Case 3), radical nephroureterectomy with bladder cuff excision was performed. Similarly, for native upper tract UC (Case 15), radical nephroureterectomy was carried out. Only five patients (25%) presented Clavien–Dindo grade II complications, and no patient developed grade III or higher complications in the first month after surgery.
Pathology findings
Clear cell RCC (ccRCC) was the most common histological subtype, identified in both native kidneys and, in one case, within the allograft (13/20, 65%). Papillary RCC was found in native kidneys in four patients (20%), while a mixed papillary-clear cell subtype was detected in the kidney graft in one patient (Case 2, 5%). In Case 19, an initial suspicion of oncocytoma was revised after a second pathology review, confirming a diagnosis of chromophobe RCC (chRCC, 5%). Regarding tumor grading, Fuhrman grade 3 was observed in five patients (25%), while most RCC cases were low-grade (Fuhrman grade 1–2, 65%). Both UTUC cases (10%) were identified as high-grade, muscle-invasive tumors: one was staged as pT4 in the transplanted kidney and the other as pT2 involving the renal pelvis and distal ureter of the native upper urinary tract.
Oncological outcomes
The oncological outcomes are summarized in Table 2. The mean follow-up for all patients was 56.9 months, ranging from 6 months to 140 months, and consisted of regular ultrasound examinations, CT scans, and evaluations of kidney function.
Two patients (10%) who had RCC in native kidneys developed metastases during follow-up, with a mean time to metastasis of 6.5 years after radical nephrectomy. One patient (5%) developed local recurrence at 4 years post-surgery, another patient (5%) was diagnosed with RCC in the contralateral kidney at 5 years, and one patient (5%) had pulmonary metastases detected at the time of nephrectomy.
Among the patients who developed metastases, one (5%) developed ccRCC metastasis localized to the prostate and seminal vesicle at 7 years post-nephrectomy, confirmed by biopsy. The patient received tyrosine-kinase inhibitors (TKIs) and maintained stable disease for 4 years with a functioning kidney graft. During the immunosuppression regimen, tacrolimus was changed to sirolimus after metastasis detection. Unfortunately, the patient died due to COVID-19 infection after 4 years. Another patient (5%) developed extra-regional lymph node metastases 6 years after surgery. No adjuvant treatment was administered, and sirolimus was added to the immunosuppression regimen. This patient also died of COVID-19 infection 5 years later, with progressive metastatic disease but a functional allograft. The patient with chRCC developed local recurrence four years after radical nephrectomy of the native kidney, requiring surgical resection. A second local recurrence occurred after another four years without distant metastasis. Surgery for the retroperitoneal tumor (stage IV with liver invasion) was performed; however, the patient died 5 days postoperatively due to cancer-related complications. The pathology findings after both tumor recurrences confirmed the chRCC histology. At the time of the native kidney nephrectomy, the patient was on dialysis after an allograft nephrectomy for a non-functional graft one year earlier. One patient developed contralateral RCC five years after undergoing native kidney nephrectomy for clear cell RCC (pT1aN0M0). This patient had returned to dialysis one year after transplantation due to chronic graft dysfunction. The patient refused contralateral nephrectomy and remained alive at the time of the study.
One case of urothelial carcinoma of the transplanted kidney was detected 10 years after KT. Initially, the patient was diagnosed with bladder UC and treated with TURBT for multiple pTa low-grade tumors. Bacillus Calmette–Guérin (BCG) therapy was initiated and maintained for one year without adverse reactions or recurrence. No changes to immunosuppression were made during BCG instillation. Two years later, hematuria and iliac fossa pain prompted reevaluation. The initial suspicion of BCG pyelonephritis was not sustained by the urinary tests. A kidney graft biopsy was performed, confirming the UC of the allograft. The CT scan detected pulmonary metastasis. A nephroureterectomy of the allograft with bladder cuff was performed, and the pathology exam showed pT4HG (pelvicalyceal urothelial carcinoma with sinus and perinephric fat invasion and psoas muscle involvement). The patient returned to dialysis, withdrawal of immunosuppression, and spontaneous remission of pulmonary metastasis was confirmed 3 months after surgery, with no adjuvant therapy. The patient is still alive, with neither bladder recurrence nor distant metastasis at 36 months follow-up.
Regarding immunosuppressive management, 10 patients (50%) underwent no changes. Conversion from tacrolimus to sirolimus occurred in three cases (15%), while in one case (5%), cyclosporine was reduced, and sirolimus was added. In two cases (10%), tacrolimus dose reduction was performed. In four cases (20%), immunosuppression was completely withdrawn. None of these adjustments negatively impacted graft function.
At study completion, 15 patients (75%) were alive, with 14 of them (70%) free from tumor recurrence or distant metastases (Figure 1). Three patients (15%) were on dialysis at the time of nephrectomy for RCC, one patient (5%) returned to dialysis after transplantectomy for RCC, and another patient (5%) after nephroureterectomy for UTUC of the allograft. No patient underwent re-transplantation following surgical treatment of malignancy.
Kaplan-Meier analysis for patients’ survival. A, Overall survival; B, Survival according to the presence/absence of metastasis.
DISCUSSION
The incidence of RCC in kidney transplant recipients is significantly higher than in the general population (0.7% vs. 0.04%). RCC affecting the native kidneys is the most common presentation [7,25-29]. In our study, 80% (16/20) of cases involved RCC in native kidneys, while RCC in the kidney graft was identified in two cases (10%). The most important risk factors associated with RCC in kidney transplant recipients are male sex, male donor sex, history of ACKD, duration of dialysis prior to kidney transplant, history of RCC, smoking, obesity, hypertension, immunosuppression and donor-derived malignancies [4,5,30]. Sapir et al. found an elevated risk of primary malignant neoplasms in female patients receiving higher cumulative doses of mycophenolate, as well as in young male patients exposed to tacrolimus over an extended period [5].
The cumulative incidence of primary malignancies rises with time post-transplantation, reaching 4–5% at 5 years, 10% at 10 years, and 25% at 20 years [4]. ESKD, as well as its etiology, significantly contributes to this risk, with a 3.6-fold increased likelihood of developing RCC compared to the general population. ESKD due to vascular or glomerular disease, or hypertensive nephrosclerosis, is associated with a higher risk of RCC than ESKD resulting from diabetes or polycystic kidney disease [1,31,32]. Approximately 60% of patients undergoing dialysis for 2–4 years develop ACKD, and among these, 20% may eventually develop RCC. The documented involution of the cysts after kidney transplant may suggest a protective role of transplant for developing RCC in patients with ACKD [33-35]. However, the risk of RCC in the kidney transplant population is higher than in the general population, suggesting that not just ACKD is related to RCC pathogenesis and that the post-transplant risk factors may play an important role in the process [33-35].
In our study, we observed that ccRCC was the predominant subtype RCC (70%) encountered in both native kidneys and, in one case, within an allograft, followed by pRCC (20%), occurring mostly in male patients. These findings agree with other studies [23,36,37]. All RCCs in our study were Fuhrman grades 2–3. Localized tumors (stages T1–T2) were more common (65%); however, 25% (5/20) of RCCs arising in native kidneys were stage T3a. This finding differs from data previously published [5,23,24,37].
The incidence of UC is also higher in kidney transplant recipients, with a threefold increase compared to the general population [38]. Risk factors for UC include exposure to aristolochic acid (from Chinese herbs or Balkan endemic nephropathy), BK virus (BKV) reactivation, smoking, and occupational exposures [39-41]. Data regarding UTUC in native or graft kidneys remain limited to small studies and case reports. In our study, both cases of UTUC were high-grade, muscle-invasive tumors (10%), consistent with findings by Zhang et al. in a Chinese cohort [16].
Currently, there are no guidelines for managing or screening RCC or UC in kidney transplant patients. The 2020 KDIGO Clinical Practice Guidelines on the Evaluation and Management of Candidates of Kidney Transplantation recommend screening candidates at increased risk for RCC (e.g., dialysis for more than three years, ACKD, or analgesic nephropathy) via ultrasound [42]. In our study, 55% (11/20) of renal tumors were diagnosed incidentally during routine post-transplant follow-up, supporting the potential value of structured screening programs.
Radical nephrectomy is recommended for RCC in native non-functional kidneys, for RCC in kidney grafts, for locally advanced or metastatic RCC, for multicentric papillary RCC, or in cases of non-functional grafts in order to ensure good oncologic outcomes [43-48]. Nephron-sparing surgery is preferred for T1a tumors (<4 cm) in functional grafts, achieving favorable oncological outcomes while preserving graft function [21,22,24,49,50]. Open partial nephrectomy for a T1a tumor of kidney graft offered a good oncologic outcome and a functional kidney graft at 36 months follow-up in Case 1. For UTUC occurring in native non-functional kidneys, radical nephroureterectomy with bladder cuff is preferred given the typically high-grade nature of these tumors [10,12,14,16,51-55].
The same surgical approach was used in Case 15 in our cohort, with no local recurrence or metastasis at 14 months follow-up. Zhang et al. reported a 33.3% contralateral recurrence rate after unilateral nephroureterectomy and demonstrated improved cancer-specific and overall survival with simultaneous bilateral nephroureterectomy without compromising graft function [16,20]. A particular malignancy evolution was observed in Case 3, where late donor-derived malignancy was suspected due to complete regression of pulmonary metastasis after allograft nephroureterectomy with bladder cuff for pT4HG UC and withdrawal of immunosuppression. Management of UTUC in graft kidneys is largely based on case reports and small retrospective series. Conservatory management (partial nephrectomy, ureteral resection) was also described in case reports [56-58].
This study has limitations, with potential selection bias due to its retrospective design and small sample size. Additionally, the lack of screening protocols for renal tumors in kidney transplant recipients may have led to the exclusion of some cases. Furthermore, the study did not identify the underlying cause of ESKD for all patients.
CONCLUSION
In summary, RCC and UTUC in kidney transplant recipients present significant therapeutic challenges for the multidisciplinary team. Surgical management provides good oncologic outcomes with a low complication rate. It is important to highlight that screening for RCC and UC in kidney transplant recipients with associated risk factors may facilitate earlier diagnosis at lower stages and grades. Further prospective research or collaboration with larger multicentric cohorts could improve the elaboration of therapeutic and screening guidelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Karami S Yanik EL Moore LE Pfeiffer RM Copeland G Gonsalves L Risk of renal cell carcinoma among kidney transplant recipients in the United States Am J Transplant 201616113479348910.1111/ajt.1386227160653 PMC 5104677 · doi ↗ · pubmed ↗
- 2Hickman LA Sawinski D Guzzo T Locke JE Urologic malignancies in kidney transplantation Am J Transplant 2018 Jan 181132210.1111/ajt.1453328985026 · doi ↗ · pubmed ↗
- 3Butler AM Olshan AF Kshirsagar AV Edwards JK Nielsen ME Wheeler SB Brookhart MA Cancer incidence among US Medicare ESRD patients receiving hemodialysis, 1996-2009 Am J Kidney Dis 201565576377210.1053/j.ajkd.2014.12.01325662835 PMC 4924349 · doi ↗ · pubmed ↗
- 4Au E Wong G Chapman JR Cancer in kidney transplant recipients Nat Rev Nephrol 2018 Aug 14850852010.1038/s 41581-018-0022-629802400 · doi ↗ · pubmed ↗
- 5Sapir-Pichhadze R Laprise C Beauchamp ME Kaouache M Zhang X Della Vecchia Atal Immunosuppression and cancer risk in kidney transplant recipients: A retrospective cohort study Int J Cancer 2024 Jun 15154122043205310.1002/ijc.3487538345158 · doi ↗ · pubmed ↗
- 6Al-Adra DP Hammel L Roberts J Woodle ES Levine D Mandelbrot D Pretransplant solid organ malignancy and organ transplant candidacy: A consensus expert opinion statement Am J Transplant 2021 Feb 21246047410.1111/ajt.1631832969590 PMC 8576374 · doi ↗ · pubmed ↗
- 7Dahle DO Skauby M Langberg CW Brabrand K Wessel N Midtvedt K Renal Cell Carcinoma and Kidney Transplantation: A Narrative Review Transplantation 2022 Jan 11061 e 52e 6310.1097/TP.000000000000376233741842 PMC 8667800 · doi ↗ · pubmed ↗
- 8Grulich A Evan Leeuwen MT Falster MO Vajdic CM Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis Lancet 20073709581596710.1016/S 0140-6736(07)61050-217617273 · doi ↗ · pubmed ↗