Immune thrombotic thrombocytopenic purpura and diabetic ketoacidosis: a case report and literature review
Geng-Hao Bai, Mei-Hwa Lin, Yu-Pei Chen, Tien-Jyun Chang, Sheng-Chieh Chou

TL;DR
A rare case of immune thrombotic thrombocytopenic purpura and diabetic ketoacidosis is reported, highlighting the importance of prompt diagnosis and treatment.
Contribution
This case report adds to the limited literature on the co-occurrence of diabetic ketoacidosis and TTP.
Findings
The patient presented with DKA and developed TTP, requiring plasma exchange and immunosuppressive therapy.
Acute renal failure was a rare complication observed in this TTP case.
The PLASMIC score and ADAMTS-13 activity were used to confirm the TTP diagnosis.
Abstract
Thrombotic thrombocytopenic purpura (TTP) is an uncommon and life-threatening disorder caused by a deficiency of ADAMTS-13, and eventually leads to microangiopathic hemolytic anemia, severe thrombocytopenia, and organ damages. Acute TTP events could be triggered by infections, or inflammations in the context of ADAMTS-13 deficiency. Recently, several case reports have indicated an association between diabetic ketoacidosis (DKA) and TTP. Here, we present a case with the concomitant presentation of DKA and TTP. A 37-year-old male with diabetes mellitus presented with typical symptoms of diabetic ketoacidosis. He was managed with an insulin pump and intravenous fluids. However, he developed seizure and progressed to coma, his rapidly deteriorating condition necessitated continuous renal replacement therapy, intubation, and inotropic support. Laboratory data indicated hemolytic anemia and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
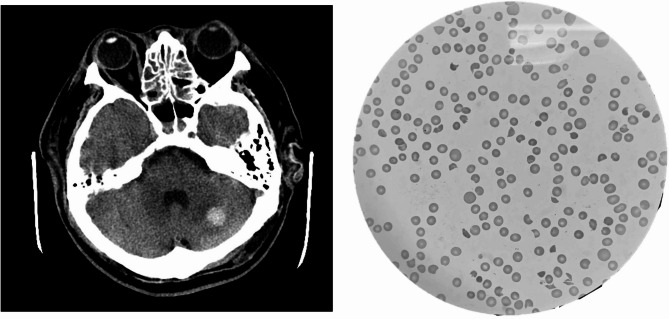 Figure 1
Figure 1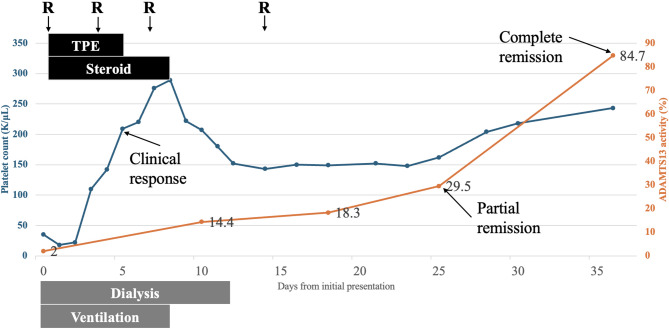 Figure 2
Figure 2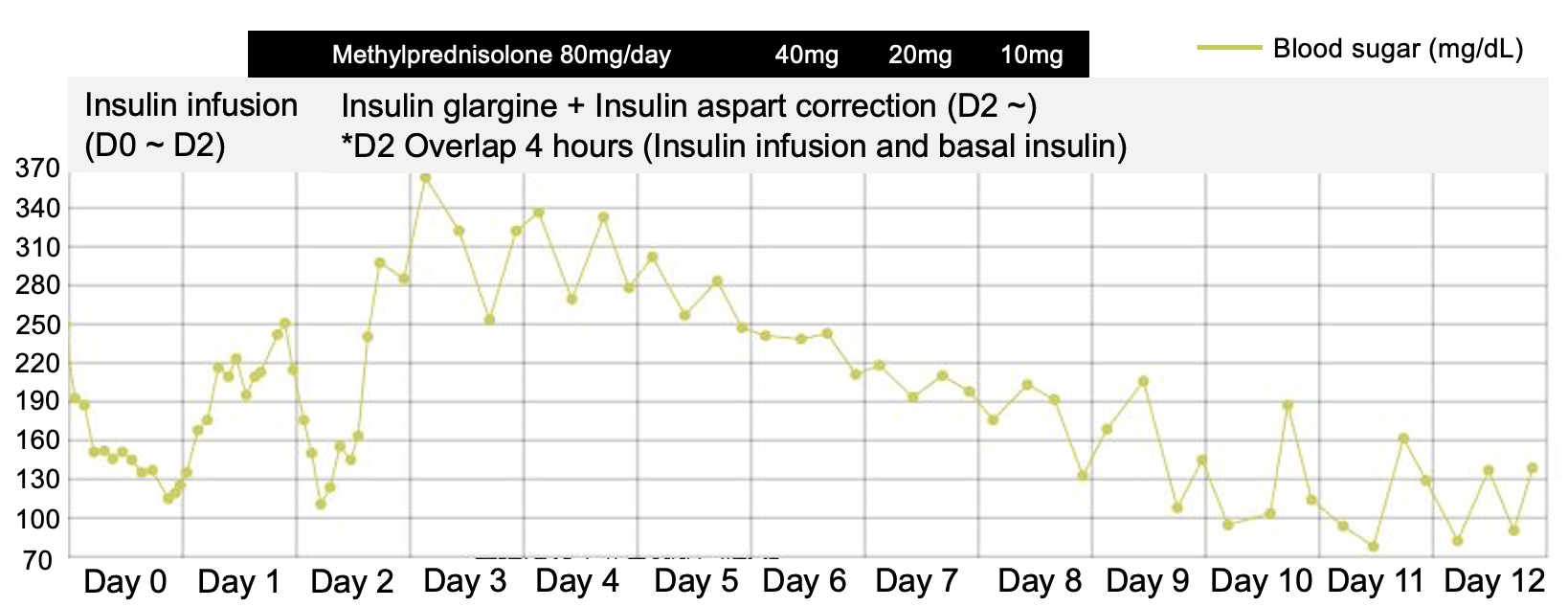 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsComplement system in diseases · Renal Transplantation Outcomes and Treatments · Blood groups and transfusion
Background
Thrombotic thrombocytopenic purpura (TTP) is a rare and life-threatening thrombotic microangiopathy characterized by microangiopathic hemolytic anemia, severe thrombocytopenia, fever, neurological symptoms, and kidney injury [1]. TTP is caused by a severe deficiency of the von Willebrand factor (vWF) cleaving protease, ADAMTS-13 (a disintegrin and metalloprotease with thrombospondin type 1 repeats, member 13) [2–5]. Most ADAMTS-13 deficiencies are due to autoantibodies, a condition known as immune TTP (iTTP). iTTP requires rapid diagnosis and urgent management, including therapeutic plasma exchange (TPE), and immunosuppressants such as steroids and rituximab [1, 2, 4, 6, 7]. The development of autoantibodies against ADAMTS-13 is generally idiopathic [1, 5, 8, 9], but acute TTP episodes could be triggered by infections, inflammations or pregnancy. On the other hand, diabetic ketoacidosis (DKA) is one of the most common life-threatening complications of diabetes mellitus. While it predominantly affects patients with type 1 diabetes, those with type 2 diabetes are also susceptible, particularly during periods of acute illness and catabolic stress. Appropriate treatment has reduced the mortality of DKA to less than 1%; however, the metabolic decompensation precipitated by underlying medical illness remains a leading cause of death in patients with DKA [10]. Several case reports have shown that TTP or similar thrombotic microangiopathy can develop concomitantly with DKA [11–21]. Here, we present a case of a man with type 2 diabetes mellitus who developed iTTP during an episode of DKA and reviewed all similar case reports from the literature.
Case presentation
A 37-year-old male without medical history, presented with mild generalized abdominal pain, nausea, vomiting, watery diarrhea, and oliguria for two days. Initially, he sought medical assistance at a local clinic, where acute viral gastroenteritis was suspected, and he was treated with hydration therapy. However, his symptoms worsened the following day, prompting a visit to the emergency department of a local hospital. Upon arrival, he experienced a generalized seizure lasting two minutes during triage. Hypertension (172/108 mmHg), icteric sclerae, and petechiae on the limbs and trunk were noted. Initial laboratory findings indicated extreme hyperglycemia (721.8 mg/dL), high anion gap metabolic acidosis (pH 7.2, bicarbonate 12.2 mmol/L, anion gap 20.8 mEq/L), hyperkalemia (5.1 mmol/L), and elevated blood ketones with an HbA1c of 11.5%. Additional findings included anemia (hemoglobin 10.8 g/dL), thrombocytopenia (16 × 10^9^/L), indirect hyperbilirubinemia (total bilirubin 3.40 mg/dL, direct bilirubin 0.94 mg/dL), mildly elevated aspartate transaminase (61.5 U/L), high blood urea nitrogen (91.29 mg/dL) and creatinine (8.53 mg/dL). Coagulation screening tests, including prothrombin time, partial thromboplastin time, and fibrinogen were normal.
The patient was admitted to the intensive care unit (ICU) on the same day and was managed with an insulin pump while continuous renal replacement therapy (CRRT) was initiated. A transfusion of platelets was administered; however, the patient’s condition worsened the following day, characterized by disturbed consciousness, hypoxia, and shock. Norepinephrine was administered and he was intubated with ventilator support. Whole-body computed tomography (CT) revealed only left cerebellum hemorrhage (Fig. 1a). After five days of management in the local hospital, the patient was transferred to a tertiary care center ICU for further evaluation of the unidentified cause of thrombocytopenia and unstable hemodynamics.
Fig. 1(a) Brain computed tomography of left cerebellum intracerebral hemorrhage; (b) Peripheral blood smear of schistocyte
On arrival, patient was in a complete coma (E1VTM1) with worsening hemolytic anemia and thrombocytopenia (12 × 10^9^/L). Both direct and indirect Coombs tests were negative. An initial blood smear revealed multiple schistocytes (Fig. 1b). The PLASMIC score was 5 and the French score was 1, suggesting an intermediate risk of TTP (Table 1). It took one day to receive the ADAMTS-13 activity result, which was 2%, confirming a severe deficiency of ADAMTS-13 and TTP. Therapeutic plasma exchange, initiated on the day the ADAMTS-13 result was confirmed and was performed for five consecutive days until platelet count rose above 150 × 10^9^/L. Steroid and rituximab were also applied at the initiation of TPE. Specifically, methylprednisolone was given 80 mg daily until the cessation of TPE and then tapered over three days. Rituximab (fixed dose, 500 mg) was administered on day 1, 4, 7, and 14. ADAMTS-13 activity was monitored weekly after clinical remission, achieving ADAMTS-13 partial remission at day 25 (29.5%), and complete remission at day 36 (84%) (Fig. 2); moreover, genetic testing for ADAMTS13 revealed no mutations.
Table 1PLASMIC score and French score of the patientParameterLaboratory dataPLASMIC score [22]French score [23]Platelet count12 × 10^9^/L (< 30 × 10^9^/L)11Creatinine level5.63 mg/dL (< 2 mg/dL; ≤2.26 mg/dL)00Parameters of hemolysisReticulocytosis, indirect bilirubinemia, highly elevated LDH, undetectable haptoglobin.1Associated conditionsNo active cancer, No history of solid-organ or hematopoietic stem cell transplant1MCV90.4 fL (< 90 fL)0INR1.01 (< 1.5)1ANA1:80 (positive ANA)0Total score (Risk category)PLASMIC score: 5 (Intermediate risk, risk of TTP: 5 ~ 24%) [20]French score: 1 (Intermediate risk, risk of TTP: 70%) [11]
Fig. 2. Platelet counts and ADAMTS-13 activity. The blue curve represents the platelet count and corresponds to the left axis, while the orange curve represents ADAMTS-13 activity and corresponds to the right axis
Continuous renal replacement therapy was transitioned to hemodialysis on the first day of plasma exchange. The patient’s consciousness improved following the initiation of therapeutic plasma exchange. We monitored blood glucose levels, blood gases, anion gap, and serum ketones in accordance with the DKA management protocol. The DKA showed significant improvement within two days of initiating continuous insulin infusion. Glycemic control improved further following the tapering of steroid therapy (Supplemental Fig. 1). The patient’s oxygen saturation and urine output showed gradual improvement. He successfully passed the spontaneous breathing trial and weaning parameters on day seven, leading to successful extubation on day eight. He was subsequently transferred to the general ward on day nine, and hemodialysis was paused on day ten. Blood urea nitrogen (BUN) and creatinine levels improved, negating the need for further hemodialysis. A glucagon test confirmed preserved pancreatic beta-cell function, facilitating the transition from insulin to oral antidiabetic medication once blood sugar levels were controlled. Kidney function remained stable over time. Prior to discharge, he regained the ability to care for himself independently, perform calculations accurately, walk long distances, and climb stairs without assistance.
Discussion
Accurate diagnosis of immune thrombotic thrombocytopenic purpura (iTTP) necessitates clinical awareness. As demonstrated by this case, iTTP was not considered until the patient was transferred to a tertiary medical center. The presence of diabetic ketoacidosis (DKA) complicated the clinical picture, rendering the presentation of TTP atypical. Moreover, the primary physicians initially focused solely on managing the DKA and its complications, overlooking signs such as hemolytic anemia and thrombocytopenia that warranted further investigation. It is imperative to enhance the awareness of intensivists and other physicians managing critical care settings to facilitate the accurate diagnosis and treatment of iTTP, particularly in complex cases such as this one.
The PLASMIC score [22] and the French score [23] are both useful tools for identifying patients with severe ADAMTS-13 deficiency before ADAMTS-13 results are available. However, in our patient, both scores yielded intermediate results, with a predicted risk of TTP ranging from 5 to 24% using the PLASMIC score and 70% using the French score [24]. Lee et al. [25, 26] further validated the predictive accuracy of the PLASMIC score in Taiwanese population, finding that MCV did not significantly contribute to risk stratification. Tang et al. also demonstrated that MCV < 90 fL was not an independent predictor of TTP. A simpler scoring system that omits MCV < 90 fL may be more suitable for identifying TTP in Chinese patients [27]. These findings suggest that MCV < 90 fL may be less relevant in predicting TTP among East-Asian populations, as evidenced by this patient’s initial MCV of 90.4 fL. Furthermore, both prediction models indicate that kidney injury is less commonly observed in TTP compared to atypical hemolytic uremic syndrome (aHUS). In this report, the patient had complicated with DKA and severe kidney injury, which could also hamper the accuracy of both scores. Most renal dysfunction in TTP is mild, but acute renal failure requiring dialysis still occurs in 4–15% of TTP patients [28]. Generally, severe renal injury happens more frequently among patients with atypical hemolytic uremic syndrome (aHUS) than those with iTTP [29]. However, a retrospective study of 92 cases of TTP with low ADAMTS-13 activity (< 10%) found that more than half of the patients had acute kidney injury, with nearly half experiencing stage 3 acute kidney injury and a quarter requiring renal replacement therapy [30]. This case highlights the relatively rare presentation of iTTP. In retrospect, uncontrolled diabetes mellitus, hypertension, and subsequent DKA may have contributed to the kidney injury more than iTTP itself in this case. Similarly complicated situation might happen in other iTTP patients, therefore extra caution should be taken while interpretating kidney injuries in possible iTTP patients.
Caplacizumab is a humanized immunoglobulin fragment that targets the A1 domain of von Willebrand factor (vWF), thereby inhibiting its interaction with the platelet glycoprotein Ib-IX-V receptor. Phase 2 and 3 clinical trials have demonstrated that caplacizumab treatment is associated with more rapid normalization of platelet counts. However, an increased risk of bleeding has also been reported, with the most common adverse events being epistaxis and gingival bleeding—most of which resolved without intervention [31]. Schofield et al. described four cases of acute thrombotic thrombocytopenic purpura (TTP) complicated by intracranial hemorrhage (ICH) in patients treated with caplacizumab. These cases were associated with poor neurological outcomes. Although refractory TTP may have contributed to the unfavorable prognoses, ICH remains a serious and recognized potential complication of caplacizumab therapy [32]. In our case, cerebellar ICH was initially detected at the local hospital. Given caplacizumab’s known risk of bleeding, its use might have exacerbated the hemorrhage, potentially increasing the risk of brainstem compression and cerebellar herniation. Furthermore, our patient’s platelet count normalized within five days following therapeutic plasma exchange alone. Therefore, the bleeding risk of caplacizumab may outweigh its potential benefits for this patient. Generally, for iTTP patients with ICH, we believe that using caplacizumab might be the most difficult decision to make and should be considered individually with extreme caution.
To the best of our knowledge, our case represents the second instance of definite iTTP complicated with DKA, and notably, it is the first to demonstrate not only clinical response but also ADAMTS-13 response. The literature contains several reports of concurrent thrombotic microangiopathy and DKA in both pediatric [11–18] and adult patients [19–21](Table 2); however, ADAMTS-13 activity below 10% was observed in only one previous case [20]. Half (5 of 12) cases had ADAMTS-13 higher than 20%, ruling out TTP, and the rest (6 of 12) had no available ADAMTS-13 results. Among all these cases, only one-third of the patients presented with platelet counts below 30 × 10^9^/L [11, 15, 17, 20], half exhibited altered consciousness [11–13, 16, 21], seizures occurred in two cases [16, 21], and a quarter required renal replacement therapy [12, 14]. Therapeutic plasma exchange (TPE) was utilized in most instances, with only two cases treated exclusively with fresh frozen plasma transfusion [17, 18]. Notably, only two cases received adjunct treatment with steroids and rituximab alongside TPE [20, 21]. Among all reported patients, only one fatality occurred [21]. From the pooled reports, DKA can occur alongside thrombotic microangiopathy (TMA), which may or may not be iTTP. Given that iTTP requires specific treatments distinct from other types of TMA, testing for ADAMTS-13 is crucial for proper clinical management. Beyond therapeutic plasma exchange (TPE), which is the standard treatment for iTTP, steroids may complicate the condition by affecting blood sugar levels and potentially exacerbating DKA. Additionally, ADAMTS-13 levels play a critical role in evaluating the remission status of iTTP. As demonstrated in this case, follow-up of ADAMTS-13 levels is equally important for guiding adjustments in immunosuppressive therapy.
Table 2. Case reports of concomitant thrombotic microangiopathy and diabetic ketoacidosisAgeSexInitial presentationLab before TPE/FFPADAMTS-13 activityTreatment for TMAOutcomeConfirmed TTPJackson et al. 2021 [20]62maleGeneralized abdominal pain, thirst, and fatigue for several daysHb: 7.5PLT: 18LDH: > 2800BUN: 78CRE: 2.4< 1SteroidFFPTPERituximabImproved and survivedTMA with high ADAMTS-13 activityPatra et al. 2011 [11]12femaleIrritability and drowsiness for one dayHb: 10.6PLT: 29LDH: 1349BUN: 61CRE: 2.252TPEImproved and survivedAlsaied et al. 2016 [14]18femaleRespiratory distress few hoursHb: 8.8PLT: 32LDH: >4000CRE: 4.431CRRTTPEImproved and survived with left side weaknessKumar et al. 2016 [15]1femaleVomiting for two daysHb: 7.7PLT: 20LDH: 743BUN: 67.5CRE: 1.9834FFPTPEImproved and survivedHermelin et al. 2019 [19]34femaleGeneral weakness and blurred visionHb: 9.6PLT: 33LDH: 2130CRE: 2.640.7TPEImproved and survived with blindnessNwankwo et al. 2023 [21]45maleSevere abdominal pain, vomiting, and altered sensorium for one daySeizureHb: 8.5PLT: 51LDH: 588CRE: 2.221SteroidTPERituximabExpiredTMA with unknown ADAMTS-13 activityKhan et al. 2013 [12]14femaleFever, vomiting, respiratory distress and LOC for one dayHb: 7.0PLT: 42LDH: 1223BUN: 75CRE: 4.4NACRRTTPEImproved and survived13femaleVomiting and LOC few hoursHb: 8.7PLT: 45LDH: 1439BUN: 39CRE: 3.5NACRRTTPEImproved and survivedMerrick et al. 2014 [13]9femaleLOCPLT: 31Deteriorating renal functionNATPEImproved and survivedMostofizadeh et al. 2018 [16]6femaleRespiratory distress, seizure and deep comaHb: 8.9PLT: 62LDH: 1455BUN: 60CRE: 2.7NATPEImproved and survivedMeenakshi et al. 2020 [17]11maleVomiting and abdominal pain for five daysHb: 10.5PLT: 16LDH: 1179BUN: 125CRE: 2.7NAFFPImproved and survivedPonnambalam et al. 2020 [18]2maleFever and breathlessness for 3 daysHb: 6.2PLT: 52LDH: 1133BUN: 52CRE: 0.8NAFFPImproved and survived Developmental regression (motor, language)Abbreviations: TMA, thrombotic microangiopathy; TTP, thrombotic thrombocytopenic purpura; DKA, diabetic ketoacidosis; LOC, loss of consciousness; Hb, hemoglobin (g/dL); PLT, platelet count (K/µL); LDH, Lactate dehydrogenase (U/L); BUN, blood urea nitrogen (mg/dL); CRE, creatinine (mg/dL); ADAMTS-13 activity (%) (a disintegrin and metalloprotease with thrombospondin type 1 repeats, member 13); CRRT, continuous renal replacement therapy; TPE, therapeutic plasma exchange; FFP, fresh frozen plasma transfusions; NA, not available
The pathophysiologic association between TTP and diabetes mellitus is not well understood, but several mechanisms have been proposed in recent studies. Diabetes mellitus is a disease that affects the microvasculature, leading to diabetic microangiopathic changes through capillary basement membrane thickening, non-enzymatic glycosylation, increased free radical activity, and increased flux through the polyol pathway [33]. Moreover, alterations in the cholesterol-to-phospholipid ratio in the red blood cell membrane may lead to stasis within the microcirculation and increased erythrocyte mechanical fragility [34]. Hyperglycemia may also induce repression of microRNA-24 (miR-24), leading to increase von Willebrand factor (VWF) expression and secretion in diabetes mellitus [35]. Additionally, plasma ADAMTS-13 levels are decreased in diabetic nephropathy, potentially due to peripheral consumption for the cleavage of chronically increased VWF and an increase in circulating proteolytic enzymes (thrombin and plasmin) that cleave ADAMTS-13. The deterioration of renal function in diabetic nephropathy is associated with even lower ADAMTS-13 levels and a high VWF/ADAMTS-13 ratio. These mechanisms may contribute to increasing severity of iTTP and might also trigger the onset of iTTP. Therefore, the concomitant existence of TTP and DKA may not be a mere coincidence [36].
Conclusions
This case report described a patient who presented with both DKA and iTTP simultaneously, presenting with coma and acute renal failure. Physician awareness of iTTP is crucial for prompt recognition and accurate diagnosis. Both the PLASMIC and French scores can assist in the initial identification of iTTP; however, ethnic differences and complex conditions may affect the accuracy of these prediction tools. Proposed mechanisms suggest that diabetes mellitus might exacerbate the severity of iTTP. Therefore, cases like this one, involving concomitant DKA and iTTP, may not occur purely by chance.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1: Supplemental Fig.1. Blood glucose trends and corresponding interventions throughout the clinical course
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sukumar S, Lämmle B, Cataland SR. Thrombotic thrombocytopenic purpura: pathophysiology, diagnosis, and management. J Clin Med 2021, 10.10.3390/jcm 10030536 PMC 786717933540569 · doi ↗ · pubmed ↗
- 2Jackson LJ, Fischer H, Abdelsayed N, Carter M. Diabetic ketoacidosis: possible cause of thrombotic thrombocytopenic purpura. Cureus 2021, 13.10.7759/cureus.18017 PMC 852031634667692 · doi ↗ · pubmed ↗
- 3Nwankwo CI, Samuels KA, Abung A, Oshikoya AF, Waqar D, Omole AE. Diabetic ketoacidosis complicated by thrombotic thrombocytopenic purpura: A rare association. Cureus 2023, 15.10.7759/cureus.37983 PMC 1020222337223178 · doi ↗ · pubmed ↗
- 4Lee C-H, Huang Y-C, Li S-S, Hsu Y-T, Chen Y-P, Chen T-Y. Application of PLASMIC score in risk prediction of thrombotic thrombocytopenic purpura: Real-World experience from a tertiary medical center in Taiwan. Front Med 2022, 9.10.3389/fmed.2022.893273 PMC 912489035615090 · doi ↗ · pubmed ↗