Right Ventricular Morphology in PA/IVS: Integrating Developmental Pathology With Echocardiographic Prognostication
Ghassan Alnaami

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
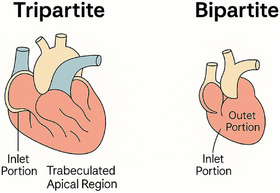 FIGURE 1
FIGURE 1| Right ventricular region | Embryological origin | Structures included | Function |
|---|---|---|---|
| Inlet portion | Primitive ventricle of the early heart tube | Tricuspid valve, chordae tendineae, papillary muscles | Receives deoxygenated blood from the right atrium |
| Trabeculated apical region | Also from the primitive ventricle | Muscular trabeculations | Contributes to myocardial contractile force |
| Outlet (infundibulum/conus) | Bulbus cordis (conus cordis segment) | Smooth‐walled outflow tract to pulmonary valve and artery | Channels blood from RV into the pulmonary circulation |
| Parameter | Function measured | Advantages | Limitations |
|---|---|---|---|
| TAPSE | Longitudinal systolic | Simple, reproducible | Angle and load‐dependent |
| TDI S' | Longitudinal systolic | Early dysfunction detection | Load‐ and angle‐dependent |
| FAC | Global systolic | Quantitative, standard cutoff | Requires a clear endocardial definition |
| RIMP (Tei index) | Global (systolic + diastolic) | Independent of shape | Affected by heart rate, rhythm |
| STE (strain) | Myocardial deformation | Detects subclinical dysfunction | Vendor differences, limited availability |
| 3D echo | Volume, ejection fraction | Most accurate RV EF | Image quality, technical demand |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Vascular anomalies and interventions
Commentary
The manuscript by Moras et al. [1] introduces a critical framework for individualized post‐interventional care in neonates with pulmonary atresia with intact ventricular septum (PA/IVS) or critical pulmonary stenosis (CPS) by leveraging echocardiographic classification of right ventricular (RV) morphology. Their work aligns directly with the developmental understanding of RV anatomy, as outlined in the next paragraph on RV developmental pathology.
Bipartite RV is composed of only two parts: the inlet and a hypoplastic outlet in most cases.
Developmental Basis of RV Morphology
The normal right ventricle is tripartite, composed of:
- Inlet portion (receives blood via the tricuspid valve),
- Apical trabeculated region (contributes to contractility),
- Outlet or infundibular portion (directs flow to the pulmonary artery).
Failure of development or muscular obliteration of the apical and/or infundibular segments leads to bipartite or monopartite RVs. (Figure 1) These developmental anomalies underlie many presentations of congenital heart disease, including tricuspid or PA, and significantly influence the RV's ability to respond to decompression interventions (See Table 1)
In their study, Moras et al. classify patients into two groups based on this anatomical distinction: Group A (tripartite RVs) and Group B (bipartite RVs). This classification strongly predicted complications post‐Pulmonary Valve Balloon Dilatation (PVBD): Tripartite RVs were associated with left ventricular (LV) systolic dysfunction due to volume redistribution and interventricular interaction. Bipartite RVs were prone to infundibular spasm, evidenced by dynamic outflow obstruction requiring beta‐blockade.
Clinical Implications of Morphotype Stratification
The clinical implications of this work are profound. Moras et al. demonstrate that 92.9% of patients with tripartite RVs experienced transient LV dysfunction, necessitating inodilator therapy and prolonged ventilation. In contrast, 76.9% of bipartite RV patients exhibited infundibular spasm managed effectively with beta‐blockers.
This distinction supports the development of a morphotype‐specific post‐procedural algorithm:
- · Tripartite RVs: Anticipate LV dysfunction, initiate inodilators early, delay extubation, and monitor for mesenteric ischemia before initiating enteral feeds.
- · Bipartite RVs: Monitor for dynamic RV outflow tract obstruction, administer beta‐blockers, and assess the need for additional pulmonary blood flow support.
In tripartite RVs, the left ventricle often encounters a sudden increase in preload following decompression due to restored antegrade pulmonary flow. This surge in pulmonary venous return, compounded by ventricular interdependence and an under‐conditioned LV, can result in transient systolic dysfunction. The LV may be particularly susceptible if it was relatively underloaded in utero. These physiologic shifts necessitate early initiation of inodilator therapy, cautious fluid management, and delayed enteral feeding until hemodynamic stability is achieved [2].
By individualizing care based on early echocardiographic findings, outcomes may improve, and unnecessary interventions may be avoided.
Surgical Versus Transcatheter Approach: A Developmental Consideration
In addition to phenotype‐specific care, our knowledge of RV developmental pathology adds valuable context comparing transcatheter RV decompression with open‐heart surgical strategies. Although transcatheter approaches offer minimally invasive access with the potential to promote RV growth, high reintervention rates and unsuitability for RV‐dependent coronary circulation limit their use in certain morphologies. Open‐heart surgery remains a viable, though more invasive, option with potential for definitive repair in select cases, typically RV‐dependent coronary circulation and non‐trabeculated or monopartite RV [3].
This dichotomy further reinforces the need for developmental and anatomical considerations in early decision‐making. Understanding which RV segments are present prenatally or at birth may help anticipate whether a patient can achieve a biventricular repair or is destined for single‐ventricle palliation.
The contribution by Moras et al. elegantly merges echocardiography with developmental anatomy to guide real‐time neonatal care. As our understanding of RV morphogenesis advances, so too must our strategies to support these vulnerable infants.
The work prompts further research avenues:
- Can prenatal echocardiographic imaging predict RV phenotype and inform delivery planning?
- Can machine learning models use echocardiographic data to automate phenotype classification and predict ICU trajectories?
- Can RV function modalities (strain, speckle tracking, TAPSE) be applied to fetal echocardiographic studies to be integrated into therapeutic planning?
These extensions could lead to a new era of precision neonatal cardiology—one grounded in the biology of development and expressed through the lens of bedside diagnostics (See Table 2)
Lastly, here is a table summarizing various echocardiographic methods to measure the RV function, which can be used in congenital heart disease, too. Unlike postnatal imaging, fetal echocardiography faces unique challenges, including limited views, high fetal heart rate, and absence of standardized RV pressure/volume measurements [4].
Conflicts of Interest
The author declares no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1P. Moras , L. Pasquini , C. M. Campanale , et al., “Echocardiographic Assessment of Cardiac Phenotype Predicts Complications and Guides Intensive Care Management Following Pulmonary Valve Balloon Dilation in Neonates With Pulmonary Atresia/Critical Pulmonary Stenosis With Intact Ventricular Septum,” Echocardiography (forthcoming).10.1111/echo.70182 PMC 1207786840367357 · doi ↗ · pubmed ↗
- 2C. Petko , A. N. Redington , and M. K. Friedberg , “Transient Left Ventricular Dysfunction After Right Ventricular Decompression in Pulmonary Atresia With Intact Ventricular Septum: Mechanisms and Clinical Implications,” Pediatric Cardiology 31, no. 6 (2010): 861–865.20204345
- 3Y. P. Mi , A. K. Chau , C. S. Chiu , T. C. Yung , K. S. Lun , and Y. F. Cheung , “Evolution of the Management Approach for Pulmonary Atresia With Intact Ventricular Septum,” Heart 91, no. 5 (2005): 657–663.15831657 10.1136/hrt.2004.033720 PMC 1768866 · doi ↗ · pubmed ↗
- 4J. Rychik , “Fetal Cardiovascular Physiology,” Pediatric Cardiology 25, no. 3 (2004): 201–209.15360113 10.1007/s 00246-003-0586-0 · doi ↗ · pubmed ↗