Co‐Infection of Mucormycosis and COVID‐19: A Retrospective Cross‐Sectional Study of Patients Admitted to Imam Khomeini Hospital in Ahvaz, Iran
Javad Zarei, Hanieh Raji, Seyed Mohammad Alavi, Farid Yousefi, Nasrin Amirrajab

TL;DR
This study found that a rare fungal infection called mucormycosis co-occurred with COVID-19 in 0.2% of hospitalized patients, mostly in older men with diabetes and severe illness.
Contribution
The study reports the prevalence and clinical features of mucormycosis co-infection in a specific hospital during the pandemic.
Findings
31 out of 12,978 patients had both mucormycosis and COVID-19 (0.2%).
Most co-infected patients were male, over 60, and had diabetes.
Severe COVID-19 was associated with a higher risk of mucormycosis co-infection.
Abstract
During the COVID‐19 pandemic, the emergence of mucormycosis, a rare but often fatal fungal infection, gained significant attention due to its increased prevalence among immunocompromised patients. This study aimed to determine the prevalence and characterize the clinical features of COVID‐19‐associated mucormycosis in patients admitted to Imam Khomeini Hospital, Ahvaz, Iran. This retrospective, cross‐sectional study analyzed clinical data from patients admitted between November 2020 and November 2021. Inclusion criteria encompassed individuals with concurrent diagnoses of COVID‐19 and mucormycosis. Data collected included demographic details, clinical features, comorbidities, laboratory findings, and treatment information. Descriptive statistics were used to summarize patient characteristics, and prevalence estimates were provided with 95% confidence intervals. Of the 12,978…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1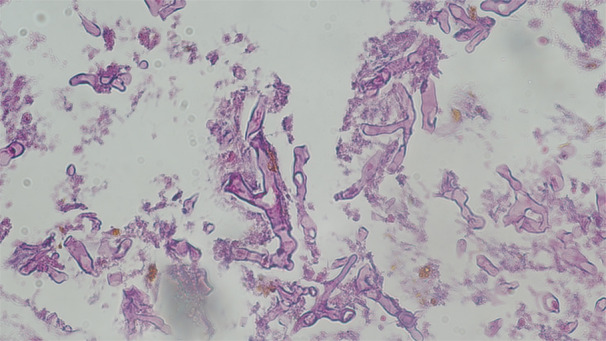 Figure 2
Figure 2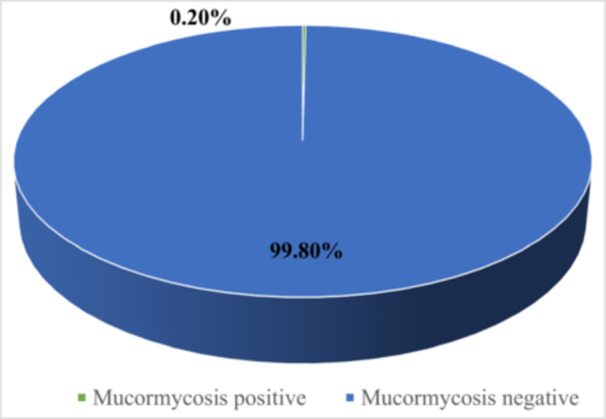 Figure 3
Figure 3| Characteristics | Number | % | 95% CI low | 95% CI up | |
|---|---|---|---|---|---|
| Age group (years) | 40 > years | 5 | 16.1 | 6.5 | 34.6 |
| 40–59 years | 11 | 35.5 | 20.2 | 54.5 | |
| ≥ 60 years | 15 | 48.4 | 30.8 | 66.4 | |
| Gender | Male | 17 | 54.8 | 36.5 | 72.0 |
| Female | 14 | 45.2 | 28.0 | 63.5 | |
| COVID‐19 severity | Number | % | 95% CI low | 95% CI up |
|---|---|---|---|---|
| Severe | 19 | 61.3 | 43.1 | 79.5 |
| Moderate | 2 | 6.5 | −2.7 | 15.6 |
| Mild | 10 | 32.2 | 14.8 | 49.7 |
| Clinical symptoms | Number | % | 95% CI low | 95% CI up |
|---|---|---|---|---|
| Fever | 6 | 19.4 | 8.5 | 38.2 |
| Cough | 18 | 58.1 | 39.4 | 74.7 |
| Chest pain | 1 | 3.2 | 0.4 | 21.6 |
| Muscular pain | 5 | 16.1 | 6.2 | 34.6 |
| Respiratory distress | 21 | 67.7 | 48.6 | 82.3 |
| Loss of consciousness | 5 | 16.1 | 6.5 | 34.6 |
| Loss or reduction of the sense of smell | 0 | 0 | N/A | N/A |
| Losing or reducing the sense of taste | 2 | 6.5 | 1.5 | 23.9 |
| Seizure | 0 | 0 | N/A | N/A |
| Abdominal pain | 0 | 0 | N/A | N/A |
| Headache | 4 | 13.0 | 4.6 | 31.1 |
| Nausea | 0 | 0 | — | 38.2 |
| Vomit | 1 | 3.2 | 0.4 | 21.6 |
| Anorexia | 2 | 6.5 | 1.5 | 23.9 |
| Dizziness | 2 | 6.5 | 1.5 | 23.9 |
| Muscular pain | 5 | 16.1 | 6.2 | 34.6 |
| Diarrhea | 0 | 0 | N/A | N/A |
| Limb Plegia | 0 | 0 | N/A | N/A |
| Risk factor | Number | % | 95% CI low | 95% CI up |
|---|---|---|---|---|
| Diabetes | 6 | 19.4 | 8.5 | 38.2 |
| Chronic blood diseases | 0 | 0 | — | — |
| Heart disease | 2 | 6.5 | 1.5 | 23.9 |
| Smoking | 0 | 0 | — | — |
| Drug abuse | 0 | 0 | — | — |
| Cancer | 0 | 0 | — | — |
| Chronic liver diseases | 0 | 0 | — | — |
| Pregnant | 0 | 0 | — | — |
| Immunodeficiency | 0 | 0 | — | — |
| HIV/AIDS | 0 | 0 | — | — |
| Inflammation | 0 | 0 | — | — |
| Hypertension | 4 | 13.0 | 4.7 | 31.1 |
| Chronic kidney diseases | 1 | 3.2 | 0.4 | 21.6 |
| Asthma | 0 | 0 | — | — |
| Other chronic lung diseases, except asthma | 0 | 0 | — | — |
| Chronic neurological disorders | 0 | 0 | — | — |
| Mortality | 25 | 80.7 | 61.9 | 91.5 |
| Detection Factor | Number | % | 95% CI low | 95% CI up | |
|---|---|---|---|---|---|
| Level PO2 | < 93 | 12 | 38.7 | 22.7 | 57.6 |
| > 93 | 19 | 61.3 | 42.4 | 77.3 | |
| CT scan | Positive | 29 | 96.7 | 77.8 | 99.6 |
| Negative | 1 | 3.3 | 0.4 | 22.2 | |
| RT‐PCR | Positive | 31 | 100.0 | — | — |
| Negative | 0 | 0.0 | — | — | |
| Histopathology | Positive | 31 | 100.0 | — | — |
| Negative | 0 | 0.0 | — | — | |
| Creatinine | Low (< 6.0 mg/dL) | 6 | 19.3 | 8.8 | 38.1 |
| Medium (6.0–20.0 mg/dL) | 21 | 67.7 | 48.6 | 82.3 | |
| High (> 20.0 mg/dL) | 4 | 13.0 | 4.7 | 31.1 | |
| Glucose | Low (< 75 mg/dL) | 0 | 0.0 | — | — |
| Medium (75–115 mg/dL) | 4 | 13.8 | 4.9 | 33.0 | |
| High (> 115 mg/dL) | 25 | 86.2 | 67.0 | 95.1 | |
| CRP § | Positive | 22 | 84.6 | 63.5 | 94.5 |
| Negative | 4 | 15.4 | 5.5 | 36.3 | |
| Cortone use | Yes | 14 | 45.2 | 28.0 | 63.5 |
| No | 17 | 54.8 | 36.5 | 72.0 | |
| Antibiotic use | Yes | 25 | 80.6 | 61.9 | 91.5 |
| No | 6 | 19.4 | 8.5 | 38.1 | |
| Surgery | Yes | 12 | 38.7 | 22.7 | 57.6 |
| No | 19 | 61.3 | 42.4 | 77.3 | |
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility
Introduction
1
The Coronavirus disease 2019 (COVID‐19) pandemic, driven by the severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2), has placed immense pressure on global healthcare systems, leading to millions of cases and fatalities worldwide. COVID‐19 presents with a broad clinical spectrum, ranging from mild respiratory symptoms to severe and potentially fatal complications [1]. Hospitalized COVID‐19 patients, especially those with underlying health conditions or in intensive care units (ICUs), are at high risk of secondary infections due to their immunocompromised status, prolonged hospital stays, and extensive use of invasive devices such as ventilators [2, 3, 4].
Mucormycosis, commonly called “black fungus”, is a highly aggressive fungal infection that predominantly affects immunocompromised individuals, such as those with uncontrolled diabetes or patients on immunosuppressive therapies. This infection is characterized by its rapid progression, often involving the sinuses, brain, and lungs, and can lead to high mortality rates if not detected and treated early [4, 5]. The concurrence of COVID‐19 and mucormycosis has created a complex and high‐risk co‐infection scenario, especially in patients subjected to prolonged ICU stays, high‐dose corticosteroid therapy, and severe hyperglycemia, which collectively increase mortality risks [5, 6].
In 2021, several countries, particularly India, reported a surge in mucormycosis cases among patients recovering from COVID‐19, highlighting an urgent need to understand this coinfection's prevalence, associated risk factors, and clinical outcomes [4, 7, 8, 9, 10, 11, 12]. However, limited data are available on COVID‐19‐associated mucormycosis in other regions, including the Middle East. Therefore, this study aims to examine the epidemiological and clinical characteristics of COVID‐19‐associated mucormycosis in patients admitted to Imam Khomeini Hospital in Ahvaz, Iran. Understanding these features can better inform clinical management practices and public health strategies to address this emerging healthcare challenge.
Materials and Methods
2
Study Design and Participants
2.1
This retrospective, cross‐sectional study analyzed clinical records of patients admitted to Imam Khomeini Hospital in Ahvaz, Iran, between November 2020 and November 2021. Ethical approval was obtained from the Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1400.484), and the study adhered to the Helsinki Declaration. The study population included patients diagnosed with both COVID‐19 and mucormycosis. The study population included patients diagnosed with both COVID‐19 and mucormycosis. COVID‐19 was confirmed through a positive RT‐PCR test for SARS‐CoV‐2. At the same time, mucormycosis diagnosis was based on clinical, radiological, and histopathological assessments following criteria established by the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the Mycoses Study Group Education and Research Consortium (EORTC/MSGERC) [13, 14, 15].
Patient Demographics and Comorbidities
2.2
The retrospective study primarily consisted of patients aged 60 years and older, a demographic more susceptible to COVID‐19‐associated mucormycosis. Key comorbidities observed included diabetes and hypertension, both of which are known risk factors for mucormycosis. Additionally, some of the patients had a history of heart disease, although conditions such as immunodeficiency and chronic lung disease were not present in this study.
Data Collection
2.3
Demographic and clinical data, including age, gender, COVID‐19 severity, comorbid conditions, and in‐hospital outcomes, were extracted from patient medical records. Laboratory parameters, such as blood glucose levels, C‐reactive protein (CRP), and creatinine, were documented alongside clinical features, including corticosteroid use, antibiotic administration, and prior surgical history. Radiological evaluations, such as CT scans of the orbit, paranasal sinuses, and lungs, were performed (Figure 1), and nasal mucosal biopsies underwent histopathological staining with hematoxylin–eosin (H&E) and Gomori methenamine silver (GMS) to confirm mucormycosis (Figure 2).
Axial CT scan of a patient with COVID‐19‐associated mucormycosis. This non‐enhanced axial CT scan shows notable mucosal thickening in the bilateral maxillary sinuses, consistent with sinonasal mucormycosis. The image also reveals partial opacification of both maxillary sinuses and the right nasal cavity, accompanied by air entrapment. These findings are characteristic of mucormycosis and illustrate the extent of sinonasal involvement in a patient concurrently diagnosed with COVID‐19.
Histopathological analysis of nasal mucosal glands in COVID‐19‐associated Mucormycosis. This histopathological smear from the left maxillary sinus highlights nasal mucosal glands with evident necrosis and mononuclear inflammatory cell infiltration, characteristic of mucormycosis. Broad, nonseptate, or pauciseptate hyphae are visible, displaying wide‐angle branching and significant tissue invasion. These fungal structures, typical of mucormycosis, are stained with Hematoxylin and Eosin at a magnification of 200×.
Sample Size and Data Analysis
2.4
To estimate the frequency of co‐infection, all patients meeting the inclusion criteria during the specified timeframe were retrospectively enrolled in this study. Thoroughly trained medical professionals reviewed each patient's medical records, ensuring data accuracy and consistency. These records were then anonymized for confidentiality. Data were analyzed using STATA version 14, and a 95% confidence interval (CI) was calculated to assess the association between co‐infection and demographic factors, comorbidities, and COVID‐19 severity.
Results
3
Among the 12,978 hospitalized patients during the study period, 31 individuals (0.2%, 95% CI: 0.2%–0.3%) were identified with COVID‐19‐associated mucormycosis. The prevalence rate was highest in male patients and those aged 60 years or older. Concurrent infections were more frequent in patients with severe cases of COVID‐19. The most common symptoms observed were respiratory distress, cough, and fever, while diabetes was the most prevalent comorbidity (Figure 3).
Frequency of Mucormycosis infection among assessed COVID‐19 patients.
Demographic Differentiation
3.1
The highest prevalence of mucormycosis related to COVID‐19 was observed in patients aged 60 years or older, with 48.4% presenting with co‐infections, compared to only 16.1% of those younger than 40. Among male patients, 54.8% had concurrent infections, whereas 45.2% were female (Table 1).
COVID‐19 Severity
3.2
The prevalence of concurrent mucormycosis was 61.3% (95% CI: 43.1%–79.5%) in patients with severe COVID‐19. In moderately ill patients, the prevalence was 6.5% (95% CI: −2.7%–15.6%); in patients with mild cases, it was 32.2% (95% CI: 14.8%–49.7%) (Table 2).
Clinical Symptoms
3.3
The most prevalent symptoms in coinfected patients were respiratory distress (67.7%), cough (58.1%), and fever (19.4%). Less common symptoms included headache (13.0%) and loss of taste (6.5%). None of the coinfected cases displayed symptoms such as limb plegia, nausea, loss of smell, seizures, abdominal pain, or diarrhea (Table 3).
Risk Factors
3.4
Diabetes was the most frequent risk factor, observed in 19.4% of coinfected patients, followed by hypertension (13.0%) and heart disease (6.5%). Mortality among coinfected cases was 80.7%, underscoring the severity of this co‐infection (Table 4).
Detection Factors
3.5
Among the diagnostic and clinical factors, 38.7% of coinfected patients had hypoxia (PO_2_ < 93), while 61.3% did not. All cases were confirmed by CT imaging and histopathology. Elevated blood glucose (> 115 mg/dL) was present in 86.2% of cases, and most had elevated CRP levels (84.6%), indicating significant inflammation. Corticosteroid exposure was documented in 45.2% of cases, antibiotic use in 80.6%, and prior surgeries in 38.7% (Table 5).
Discussion
4
This retrospective study identified a 0.2% prevalence of COVID‐19‐associated mucormycosis among hospitalized patients, a rate that aligns with the lower range of prevalence figures reported in studies from India, where prevalence estimates have ranged from 0.2% to 1.8% among COVID‐19 cases [7, 16, 17, 18, 19]. The relatively higher prevalence documented in some Indian studies has been attributed to various factors, including high corticosteroid usage in COVID‐19 treatment protocols, environmental exposure to fungal spores, and the substantial prevalence of uncontrolled diabetes, which is a significant risk factor for mucormycosis [4, 6].
The comparatively lower prevalence observed in this study may reflect regional differences in corticosteroid administration practices, variations in healthcare protocols, and SARS‐CoV‐2 strain diversity. Certain aggressive strains of the virus have been associated with an increased incidence of mucormycosis in some studies, suggesting that regional strain variability may influence co‐infection prevalence [7, 20]. Furthermore, the differences in mucormycosis prevalence across geographic areas underscore the impact of local environmental and clinical factors, such as fungal spore exposure and ICU care protocols, on infection rates [10, 11]. In Middle Eastern regions, where environmental and clinical conditions differ from those in South Asia, a lower prevalence of mucormycosis may be expected, which is in line with our study findings.
Emerging studies from other regions, including Southeast Asia and the United States, have reported prevalence rates lower than those documented in India, supporting the hypothesis that local clinical practices, including controlled corticosteroid use and proactive diabetes management, may play a critical role in reducing mucormycosis risk [21, 22]. These findings highlight the importance of region‐specific clinical guidelines and infection control practices in managing COVID‐19 patients and preventing secondary fungal infections such as mucormycosis.
Despite the relatively low prevalence, concurrent mucormycosis represents a serious risk among severe COVID‐19 cases, particularly for immunocompromised patients, elderly individuals, and those requiring extended ICU admission [4, 20, 23]. Patients aged 60 years and older in our study exhibited a markedly higher rate of co‐infection, likely due to age‐associated immunosenescence and the prevalence of comorbidities, which have been shown to increase susceptibility to opportunistic fungal infections [24, 25, 26]. This pattern underscores the importance of vigilant monitoring for fungal superinfections in older COVID‐19 patients, especially those with other risk factors.
Our findings underscore the prominent role of diabetes as a major risk factor, observed in 19.4% of COVID‐19‐associated mucormycosis cases in this study. This aligns with previous reports indicating diabetes prevalence between 15% and 70% in coinfected patients, highlighting the critical role of hyperglycemia in fostering fungal growth while compromising immune responses to Mucorales fungi [6, 27]. Additionally, the observed prevalence of hypertension (13%) is consistent with other studies and suggests that hypertension may compound COVID‐19's pro‐thrombotic and inflammatory effects, increasing vulnerability to mucormycosis [28, 29].
Furthermore, 38.7% of mucormycosis patients in our study presented with hypoxia, which aligns with previous reports indicating high rates of respiratory distress in coinfected patients [21, 22, 30]. Hypoxia and other respiratory symptoms, such as dyspnea and cough, are common among mucormycosis patients and may exacerbate respiratory complications in COVID‐19, further impairing oxygenation and leading to poorer outcomes. Co‐infection among non‐hypoxic patients in our study underscores the critical need for broader screening practices for mucormycosis in COVID‐19 patients, regardless of respiratory symptoms. This is particularly relevant as latent or subclinical mucormycosis infections may progress undetected, leading to severe complications. Cornely et al. and Samson and Dharne emphasize that early identification of asymptomatic or mildly symptomatic cases can prevent the escalation of invasive fungal disease [31, 32]. Moreover, Dilek et al. [22] suggest that screening protocols inclusive of non‐hypoxic COVID‐19 patients could improve early detection and treatment outcomes by identifying fungal colonization before it advances to more severe disease states.
Furthermore, 38.7% of mucormycosis patients in our study presented with hypoxia, which aligns with previous reports indicating high rates of respiratory distress in coinfected patients [21, 22, 30]. However, the presence of co‐infection in non‐hypoxic patients highlights the necessity of screening for mucormycosis across all COVID‐19 patients, regardless of respiratory symptoms, to identify potential latent fungal infections.
Diagnostic confirmation through universal RT‐PCR and CT positivity in this study supports the reliability of these tools for detecting COVID‐19 in patients with mucormycosis, even in cases without typical hypoxic symptoms [31, 33]. The frequent observations of glucose dysregulation and heightened inflammatory markers in coinfected cases further reinforce the interplay between hyperinflammation, hyperglycemia, and mucormycosis risk in COVID‐19 patients [4]. Although corticosteroid use was documented in nearly half of the cases, careful glucocorticoid management remains essential to mitigate infection risk without exacerbating hyperglycemic conditions.
Diagnostic confirmation of Mucor infection in this study was based on clinical, radiological, and histopathological criteria, which are widely accepted for the diagnosis of mucormycosis. As highlighted in recent literature, RT‐PCR analysis of Mucorales in tissue or biopsy samples can detect probable mucormycosis infection up to 11 days before standard diagnostic methods, offering a significant advantage for early intervention [34, 35].
While this study provides valuable insights into the epidemiological and clinical characteristics of COVID‐19‐associated mucormycosis, several limitations must be acknowledged. First, the retrospective nature of the study design limited our ability to control for confounding variables, potentially introducing selection bias, as only patients meeting stringent inclusion criteria were analyzed. Additionally, our reliance on clinical, radiological, and histopathological diagnostic methods may have resulted in an underestimation of mucormycosis cases due to potential misclassification or undiagnosed instances within the COVID‐19 patient population. We recognize the significant value of molecular diagnostic techniques, such as RT‐PCR, for the early and accurate identification of Mucorales, and we emphasize the importance of incorporating these advanced methods in future research to enhance diagnostic precision and guide targeted therapeutic interventions. Furthermore, the absence of a control group comprising COVID‐19 patients without mucormycosis restricts our ability to draw direct comparative conclusions regarding symptom profiles and risk factors specific to mucormycosis. Lastly, due to resource constraints, molecular diagnostic techniques—which could have improved pathogen specificity—were not employed. Future studies utilizing a prospective, multicenter design, along with molecular diagnostic tools and a more comprehensive control group, are essential to validate our findings and to further elucidate the complex relationship between COVID‐19 and mucormycosis.
Conclusion
5
These findings align with global reports on the demographics, clinical presentations, comorbidities, and prognosis of patients with COVID‐19 and secondary mucormycosis. The prevalence underscores the need for healthcare providers to maintain high clinical vigilance for signs of opportunistic fungal infections, especially in older males with diabetes presenting with typical COVID‐19 respiratory symptoms. Early detection and management of diabetes, along with cautious corticosteroid use, are prudent in these high‐risk patients.
The high mortality rate of 80.7% among coinfected patients in this study highlights the severe and life‐threatening nature of COVID‐19‐associated mucormycosis. This alarming mortality rate underscores the urgent need for early diagnosis, aggressive treatment, and preventive measures to reduce the devastating impact of this co‐infection.
Further collaborative studies are necessary to confirm population‐based estimates, elucidate infection mechanisms, and standardize prevention and treatment protocols for this life‐threatening COVID‐19 complication. Our findings provide essential insights to guide clinical vigilance and timely interventions that could mitigate mucormycosis occurrence and its severe consequences in vulnerable hospitalized COVID‐19 patients. Future studies should aim to incorporate molecular characterization techniques to improve the specificity of mucor isolate identification and potentially reveal species‐specific clinical patterns.
Author Contributions
Javad Zarei: data curation, project administration, and supervision. Hanieh Raji: methodology and data curation. Seyed Mohammad Alavi: data curation, supervision, and conceptualization. Farid Yousefi: methodology and data curation. Nasrin Amirrajab: data curation, software, writing – original draft, investigation, formal analysis, validation, writing – review and editing, and visualization.
Conflicts of Interest
The authors declare no conflicts of interest.
Transparency Statement
The lead author Nasrin Amirrajab affirms that this manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization , “WHO Coronavirus (COVID‐19) Dashboard,” published 2023, https://covid 19.who.int/.
- 2W. Guan , Z. Ni , Y. Hu , et al., “Clinical Characteristics of Coronavirus Disease 2019 in China,” New England Journal of Medicine 382, no. 18 (2020): 1708–1720.32109013 10.1056/NEJ Moa 2002032 PMC 7092819 · doi ↗ · pubmed ↗
- 3Z. Wu and J. M. Mc Googan , “Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID‐19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention,” Journal of the American Medical Association 323, no. 13 (2020): 1239–1242.32091533 10.1001/jama.2020.2648 · doi ↗ · pubmed ↗
- 4A. K. Singh , R. Singh , S. R. Joshi , and A. Misra , “Mucormycosis in COVID‐19: A Systematic Review of Cases Reported Worldwide and in India,” Diabetes & Metabolic Syndrome 15, no. 4 (2021): 102146.34192610 10.1016/j.dsx.2021.05.019PMC 8137376 · doi ↗ · pubmed ↗
- 5A. Patel , H. Kaur , I. Xess , et al., “A Multicentre Observational Study on the Epidemiology, Risk Factors, Management and Outcomes of Mucormycosis in India,” Clinical Microbiology and Infection 26, no. 7 (2020): 944.e 9–944.e 15.10.1016/j.cmi.2019.11.02131811914 · doi ↗ · pubmed ↗
- 6T. M. John , C. N. Jacob , and D. P. Kontoyiannis , “When Uncontrolled Diabetes Mellitus and Severe COVID‐19 Converge: The Perfect Storm for Mucormycosis,” Journal of Fungi 7, no. 4 (2021): 298.33920755 10.3390/jof 7040298 PMC 8071133 · doi ↗ · pubmed ↗
- 7A. Patel , R. Agarwal , S. M. Rudramurthy , et al., “Multicenter Epidemiologic Study of Coronavirus Disease–Associated Mucormycosis, India,” Emerging Infectious Diseases 27, no. 9 (2021): 2349–2359.34087089 10.3201/eid 2709.210934 PMC 8386807 · doi ↗ · pubmed ↗
- 8H. Prakash and A. Chakrabarti , “Global Epidemiology of Mucormycosis,” Journal of Fungi 5, no. 1 (2019): 26.30901907 10.3390/jof 5010026 PMC 6462913 · doi ↗ · pubmed ↗