Lateral Flow Device Aspergillus Routine Testing for Invasive Pulmonary Aspergillosis in Patients Who Are Critically Ill: A Multicenter Intensive Care Unit Cohort Study
Stefan Hatzl, Lisa Kriegl, Christina Geiger, Philipp Eller, Robert Krause

TL;DR
A new rapid test for a dangerous lung infection in ICU patients shows high accuracy and could help doctors act faster.
Contribution
The study evaluates a lateral flow device for rapid Aspergillus detection in ICU patients, showing strong clinical utility.
Findings
The lateral flow device test showed 71% sensitivity and 98% specificity for diagnosing probable IPA.
The test has a high positive predictive value (92%) and negative predictive value (90%).
The diagnostic odds ratio was 104, indicating strong diagnostic performance.
Abstract
The incidence of invasive pulmonary aspergillosis (IPA) is rising among intensive care unit (ICU) patients, with early diagnosis and treatment being critical for survival. Lateral flow assays for Aspergillus antigen detection have recently been introduced, enabling rapid results within an hour and potentially supporting earlier clinical decision making and timely antifungal therapy. This retrospective multicenter study included 180 ICU patients, 48 with IPA and 132 controls, across 9 treatment centers. Fungal infections were classified according to the FUNDICU criteria (Invasive Fungal Diseases in Adult Patients in Intensive Care Unit). Among the 180 patients, 48 were classified as having probable IPA, while 132 exhibited host factors and radiologic findings consistent with IPA but did not meet the FUNDICU criteria. In this cohort, the sensitivity and specificity of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
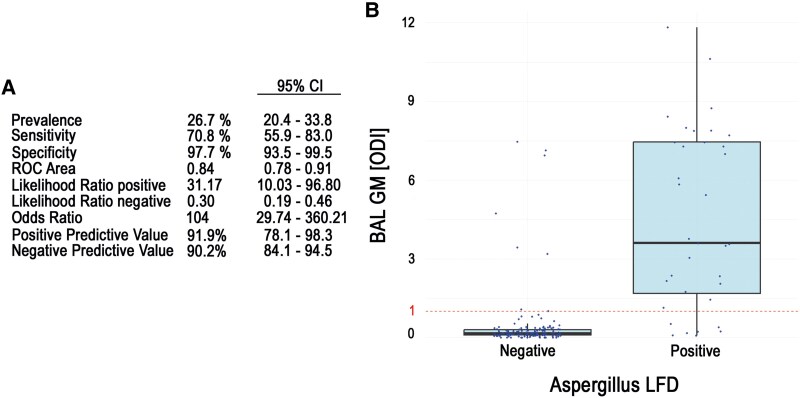 Figure 1
Figure 1| No. (%) or Median (IQR) | ||||
|---|---|---|---|---|
| Variable | Overall (n = 180) | IPA (n = 48) | No-IPA (n = 132) |
|
| Age, y | 63 (55–74) | 61 (49–69) | 65 (55–75) | .014 |
| Female | 53 (29) | 9 (18) | 44 (33) | .058 |
| Body mass index, kg/m2 | 27.9 (24.7–32.4) | 25.6 (22.8–28.1) | 28.6 (25.4–33.2) | .001 |
| Laboratory findings | ||||
| Leukocytes, G/L | 9.5 (6.8–13.9) | 9.9 (6.9–15.9) | 9.4 (6.8–13.2) | .552 |
| Neutrophils, G/L | 8.6 (5.9–12.1) | 9.4 (5.8–13.7) | 8.4 (5.9–11.7) | .661 |
| Lymphocytes, G/L | 0.7 (0.4–0.9) | 0.6 (0.3–0.9) | 0.7 (0.5–0.9) | .204 |
| Hemoglobin, g/dL | 11.5 (8.6–13.5) | 9.4 (8.6–11.0) | 12.3(10.7–13.8) | <.001 |
| Platelets, G/L | 207 (66–290) | 133 (65–227) | 221 (157–309) | <.001 |
| CRP, mg/L | 123 (71–191) | 140 (88–217) | 112 (70–177) | .075 |
| Bilirubin, mg/dL | 0.5 (0.4–0.9) | 1.2 (0.5–2.3) | 0.5 (0.4–0.7) | <.001 |
| Creatinine, mg/dL | 1.1 (0.8–2.0) | 1.6 (0.9–7.0) | 1.1 (0.8–1.4) | <.001 |
| Host factor | <.001 | |||
| EORTC/MSG risk factor | 57 (32) | 15 (31) | 42 (32) | |
| Hematologic malignancy | 28 (49) | 7 (47) | 21 (50) | |
| Allogeneic SCT | 9 (16) | 4 (27) | 5 (12) | |
| Solid organ transplant | 12 (21) | 4 (27) | 8 (19) | |
| Glucocorticoids | 39 (68) | 11 (73) | 28 (66) | |
| Neutropenia | … | 7 (46) | 20 (47) | |
| B-cell inhibitor | 7 (12) | 3 (20) | 4 (10) | |
| T-cell inhibitor | 17 (30) | 6 (40) | 11 (26) | |
| Inborn error of immunity | 1 (2) | 1 (7) | 0 (0) | |
| COVID-19 | 63 (35) | 10 (21) | 53 (40) | |
| Influenza | 25 (14) | 5 (10) | 20 (15) | |
| Solid tumor | 8 (4) | 2 (4) | 6 (5) | |
| Decompensated cirrhosis | 7 (3) | 4 (9) | 3 (2) | |
| Moderate/severe COPD | 20 (11) | 12 (25) | 8 (6) | |
| Fungal prophylaxis | 20 (11) | 7 (14) | 23 (17) | .651 |
| ICU characteristics | ||||
| SOFA | 7 (4–9) | 7 (4–8) | 7 (4–9) | .614 |
| PaO2/FIO2 | 125 (79–271) | 125 (81–350) | 136 (79–178) | .572 |
| Ventilatory support | .001 | |||
| Noninvasive ventilation | … | 3 (6) | 2 (1) | |
| Invasive ventilation | … | 37 (77) | 124 (94) | |
| vv-ECMO | … | 8 (17) | 6 (5) | |
| No. (%) or Median (IQR) | |||||
|---|---|---|---|---|---|
| Mycologic Findings | Missing | Overall (n = 48) |
|
|
|
| Optical density index | |||||
| Serum-GM | 0 (0) | 0.32 (0.11–0.95) | 0.12 (0.10–0.91) | 0.32 (0.14–1.6) | .316 |
| BAL-GM | 0 (0) | 3.58 (1.13–7.29) | 1.07 (0.8–4.73) | 3.76 (2.16–7.45) |
|
| β- | 0 (0) | 92.5 (15.4–254.7) | 92.4 (15.4–485.0) | 92.5 (29.4–235.0) | .937 |
|
| 14 (30) | 24/34 (71) | 3/10 (30) | 19/24 (80) |
|
| BAL culture positive | 0 (0) | 29 (60) | 6 (20) | 23 (80) |
|
|
| 24 (85) | 3 (50) | 21 (92) | ||
|
| 1 (3) | 1 (16) | 0 (0) | ||
|
| 1 (3) | 0 (0) | 1 (4) | ||
|
| 1 (3) | 0 (0) | 1 (4) | ||
|
| 2 (6) | 2 (33) | 0 (0) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Pneumocystis jirovecii pneumonia detection and treatment
Invasive pulmonary aspergillosis (IPA), caused by the ubiquitous mold Aspergillus, is a major cause of morbidity and mortality among patients in the intensive care unit (ICU) who are immunocompromised and nonneutropenic [1]. Adults who are nonneutropenic and critically ill with varying comorbidities represent a diverse group at risk for invasive fungal infections. To address this shift in the at-risk population, the FUNDICU algorithm (Invasive Fungal Diseases in Adult Patients in Intensive Care Unit) for diagnosing IPA in the ICU was recently developed [2]. The FUNDICU algorithm was created to standardize outcome definitions in clinical research on fungal diseases in the ICU setting. An initial validation study showed that the FUNDICU criteria outperform previously published diagnostic algorithms for IPA in clinical settings [1, 3, 4]. Galactomannan (GM) detection in serum or bronchoalveolar lavage fluid (BALF) remains the primary diagnostic method for IPA, alongside culture-based identification of Aspergillus species [2, 5]. GM detection has also been validated for noninvasive upper airway samples, highlighting its utility in different clinical settings [6]. The GM enzyme-linked immunosorbent assay has a turnaround time of approximately 3 hours and requires skilled laboratory personnel. However, it is typically performed in batches due to processing constraints, limiting its availability around the clock and reducing its utility for patients who are critically ill and require rapid decision making [7]. This is particularly concerning for patients with severe influenza, who may develop IPA upon ICU admission, where delays in initiating effective antifungal therapy are linked to higher mortality [8, 9]. Lateral flow assays for detection of Aspergillus antigen have recently been introduced, offering rapid testing within an hour, which may enable faster decision making and timely initiation of antifungal treatment [7, 10]. In this multicenter cohort study, we aimed to evaluate the diagnostic properties of an easy-to-use lateral flow assay for diagnosing IPA at the bedside in the ICU.
METHODS
Study Cohort
We conducted a multicenter observational study across 9 clinical centers in Austria, including patients admitted to the ICU from 1 January 2019 to 1 January 2025. Aspergillus LFD analysis was performed alongside conventional GM testing during the clinical workup (Supplementary Figure 1). The cohort included 48 consecutive adult patients diagnosed with IPA based on the FUNDICU algorithm, forming the case group. The control group consisted of 132 patients who had FUNDICU host factors and thoracic computed tomography changes consistent with the algorithm but tested negative for invasive fungal infection [2]. Patients with immunosuppression were classified according to the revised criteria of the European Organization for Research and Treatment of Cancer/Mycoses Study Group (EORTC/MSG), as outlined in the FUNDICU algorithm [11]. The study was approved by the local review board (EK: 32-302ex19/20) and conducted in accordance with the Declaration of Helsinki principles.
Lateral Flow Assay Performance
We used an Aspergillus-specific lateral flow device (LFD; OLM Diagnostics), which detects an extracellular glycoprotein antigen secreted during active growth of Aspergillus spp. For routine LFD testing, 100 μL of untreated BALF samples were applied to the LFD. Results were visually assessed after a 15-minute incubation at room temperature, as recommended. Bound antigen-antibody-gold complexes were indicated by a red line, with intensity proportional to the antigen concentration. Test line intensity ranged from strong positive to weak positive or negative [12, 13]. OLM Diagnostics recently merged with IMMY, and the OLM LFD test is no longer available.
Statistical Analysis
Statistical analysis was performed in R version 4.0.5 (https://www.r-project.org/). The diagnostic performance of the LFD for probable IPA vs no IPA based on the FUNDICU algorithm was evaluated. Proven IPA cases were diagnosed postmortem via necropsies whenever possible. Negative predictive value, positive predictive value, sensitivity, and specificity were calculated. Additionally, diagnostic odds ratios with 95% CIs were determined. Survival outcomes between patients who were Aspergillus LFD positive and negative were assessed in patients with probable IPA via Kaplan-Meier estimators. In addition, we investigated the impact of other Aspergillus biomarkers (bronchoalveolar lavage [BAL]–GM, serum-GM, Aspergillus polymerase chain reaction, and positive Aspergillus culture result) on 30-day overall survival in Cox regression models. To evaluate potential factors associated with false-negative LFD test results, we employed an unbiased approach by determining univariable predictors of false-negative LFD within logistic regression models and using adaptive LASSO regression (least absolute shrinkage and selection operator), including all baseline parameters to identify independent factors.
RESULTS
Study Cohort
A total of 180 adult patients admitted to the ICUs of our 9 treatment centers were evaluated for IPA via the FUNDICU algorithm, with Aspergillus LFD testing also available. LFD testing was conducted as part of the routine patient workup alongside other fungal parameters. Of these, 48 patients exhibited probable IPA, while 132 had host factors and radiologic findings consistent with IPA but did not meet the FUNDICU criteria and were thus classified as not having IPA. Respiratory samples for GM and LFD testing were collected via bronchoscopy. Of the 34 patients who were Aspergillus LFD positive, 33 had a strong reaction and 1 moderate. None showed a weak reaction.
The median age of the cohort was 63 years (IQR, 55–75), with patients with IPA being younger than controls at 61 years (49–69) vs 65 (55–75, P = .014). Among the cohort, 53 patients (29%) were female. The groups had similar immunosuppression profiles, as indicated by baseline blood counts, and approximately 30% of patients in both groups were classified according to the EORTC/MSG criteria due to underlying immunosuppressive conditions. Antimold prophylaxis use was comparable between groups, with 7 (14%) in the IPA group and 23 (17%) in the control group.
Regarding nonneutropenic ICU conditions, differences emerged between the groups. Patients with IPA more frequently had chronic obstructive pulmonary disease, while COVID-19 was more prevalent in the control group. Both groups were characterized by severe respiratory failure, but extracorporeal membrane oxygenation was more commonly used in patients with IPA than in controls. Detailed patient characteristics are summarized in Table 1.
Fungal Characteristics of the Patients With IPA
As outlined previously, 48 patients had probable IPA according to the FUNDICU criteria and, for patients treated in the ICU who were immunocompromised, the EORTC/MSG criteria. The most common Aspergillus species cultured from BALF was Aspergillus fumigatus, identified in 24 of 48 cases (50%). Interestingly, patients with a positive Aspergillus LFD result tended to have higher levels of mycologic biomarkers, particularly those obtained from BALF. BAL-GM levels were significantly higher in patients who were LFD positive (3.76; IQR, 2.16–7.45) as compared with patients who were LFD negative (1.07; IQR, 0.8–4.73; P = .034). Additionally, patients who were LFD positive had a higher frequency of positive Aspergillus polymerase chain reaction results from BALF at 19 of 24 (79%) vs 3 of 10 (30%) in patients who were LFD negative (P = .001). This finding was consistent for positive Aspergillus culture results overall, with 23 of 29 (79%) in patients who were LFD positive as compared with 6 of 29 (21%) in patients who were LFD negative (P = .042; Table 2). Despite this higher evidence of Aspergillus infection in patients who were LFD positive, a positive LFD result did not influence patient survival outcomes (Supplementary Figure 2). In addition, we analyzed the impact of other Aspergillus biomarkers on the 30-day survival in patients with IPA. Interestingly, none were associated with survival outcomes (Supplementary Table 1).
Diagnostic Properties of the Aspergillus LFD Test
The sensitivity and specificity of the BAL LFD test for diagnosing probable IPA vs no IPA in our cohort were 71% (95% CI, 56%–83%) and 98% (94%–100%), respectively, when applied to patients with FUNDICU or EORTC/MSG host factors and radiologic findings consistent with the criteria. The area under the receiver operating characteristic curve for the LFD test was 0.84. The positive and negative likelihood ratios were 31.17 (10.03–96.80) and 0.30 (.19–.46). The diagnostic odds ratio for IPA was 104 (30–360). The positive and negative predictive values were 92% (78%–98%) and 90% (84%–95%). For the LFD test as a surrogate for established mycologic factors, the sensitivity for positive BAL-GM and Aspergillus culture was calculated. The sensitivity of the BAL LFD test for a positive BAL-GM test result (optical density index >1) was 71% (56%–83%; 30 of 39 patients had positive LFD results). The LFD test had a sensitivity of 80% for a positive Aspergillus culture finding (23 of 29 patients with a positive culture finding had a positive LFD result). Diagnostic properties are summarized in Figure 1. Of the 48 patients diagnosed with IPA, 32 died, and 18 of these underwent necropsy with histopathologic examination. Among the 18 necropsies, 15 showed histopathologic evidence of proven IPA.
A, The diagnostic properties of the Aspergillus lateral flow device (LFD) test. B, The box plots of bronchoalveolar lavage–galactomannan (BAL-GM) tests in relation to a positive or negative Aspergillus LFD test result. Data are presented as median (line), IQR (box), and 95% CI (error bars). ODI, optical density index; ROC, receiver operating characteristic curve.
The sensitivity and specificity of the Aspergillus LFD for diagnosing postmortem proven IPA were 92% (95% CI, 62%–100%) and 83% (36%–100%), respectively. The area under the receiver operating characteristic curve was 0.88, indicating good overall diagnostic performance. The positive likelihood ratio was 5.5 (.91–33.18), and the negative likelihood ratio was 0.10 (.01–.68), resulting in a diagnostic odds ratio of 55.00. The positive and negative predictive values were 92% (62%–100%) and 83% (36%–100%).
Risk Factors Associated With False-Negative LFD Test Results
Having demonstrated high specificity in our ICU cohort, which consisted of patients with a high pretest probability for IPA but lower sensitivity, we sought to determine whether independent factors were associated with false-negative results. First, we used logistic regression models to analyze potential associations between false-negative LFD results and baseline parameters. We found that high absolute leukocyte counts and belonging to the EORTC/MSG host factor group were associated with lower odds of false-negative Aspergillus LFD results (Supplementary Table 2). To identify independent predictors of false-negative LFD results, we applied an adaptive LASSO regression as an unbiased approach suitable for small event numbers (Supplementary Figure 3). Interestingly, none of the baseline characteristics were associated with false-negative LFD results.
DISCUSSION
We report the utility of a bedside Aspergillus LFD in the ICU, acknowledging the recent shift in IPA classification toward patients who are critically ill and nonneutropenic as an at-risk population. Our analysis focused on a cohort of patients with a high pretest probability of IPA, including those who met the host criteria and radiologic findings defined by the recent FUNDICU algorithm [1, 2]. This is reflected by an exceptionally high prevalence of 26.7%. The composition of our cohort is important to note, as there are differences in host factors between patients with IPA and the control group of patients without IPA. For example, more patients with COVID-19 in the control group underwent LFD testing than those in the IPA group. This likely reflects early findings of COVID-19–associated pulmonary aspergillosis, which prompted more aggressive diagnostics for invasive fungal diseases in these patients as compared with others, resulting in a higher number of patients without IPA in the control group [14, 15]. Aspergillus LFD positivity serves as a surrogate marker for mold growth in the tracheobronchial system, which explains the association with higher BAL-GM levels and successful culture of Aspergillus spp. The observed correlation between LFD positivity and the BAL biomarker but not the serum biomarker likely reflects the higher diagnostic sensitivity of BAL as compared with serum [16]. Ultimately, since LFD positivity indicates the presence of Aspergillus spp in the tracheobronchial tree, this correlation is to be expected. Using the JF5 monoclonal antibody, the LFD test in this study detects an extracellular mannoprotein antigen secreted during the active growth of Aspergillus species. Several biological factors, including environmental growth conditions (eg, pH and carbon source due to viral replication), can influence the amount of mannoprotein and other fungus-specific proteins released, potentially affecting the binding capacity of the JF5 antibody [12]. In addition, host-related factors such as prior or ongoing antifungal therapy may affect LFD sensitivity, as this has been demonstrated in large clinical studies and in animal models for other fungal proteins [17]. Bedside testing for IPA is an attractive approach for the early identification of patients with this critical condition, particularly in an ICU setting where timely treatment is crucial [9]. We also investigated the impact of Aspergillus LFD positivity alongside other established biomarkers on 30-day survival in patients with IPA. Surprisingly, none of these biomarkers significantly affected survival. This may be due to the varying host factors in our cohort, known to be major determinants of survival, and the limited sample size. For example, serum-GM, a marker of angioinvasion, showed a trend toward worse outcomes, which aligns with previous reports [18]. However, these findings are exploratory and require validation in larger studies. A major difference between our cohort and previous reports on bedside LFD testing for IPA is that the testing in our study was conducted during routine patient care, with BALF analyzed immediately rather than being stored and tested later [7, 10, 19, 20]. As expected for a population in which the test is used as a confirmatory tool for patients judged to have a high probability of IPA, the LFD demonstrated very high specificity of nearly 98% and moderate sensitivity of 71%. As with any diagnostic algorithm, including the FUNDICU criteria, there is an inherent diagnostic “gray zone” that introduces a degree of uncertainty [1]. This makes such algorithms challenging to define as a true gold standard, as the only definitive proof of invasive fungal disease remains the histopathologic demonstration of invasive hyphae in tissue. To address this, we evaluated the diagnostic performance of the LFD against postmortem proven cases of IPA. The LFD demonstrated a sensitivity of 92% and a specificity of 83%, thereby confirming its diagnostic accuracy when compared with histologic evidence. This finding suggests that the LFD could be utilized as a tool to confirm the presence of IPA and promptly initiate antimold therapy. However, the LFD alone is not sufficient to completely rule out IPA. These findings represent the classic trade-off of single-parameter tests. Future research could minimize this trade-off in sensitivity by combining the LFD with risk scores for IPA in the ICU setting [21, 22]. The moderate sensitivity might also be influenced by antifungal prophylaxis, which was applied in 14% of patients with IPA, thus lowering the sensitivity of mycologic biomarker testing [10].
Easy-to-use bedside tests such as the LFD may serve as a practical surrogate for BAL-GM diagnostics, particularly in time-sensitive ICU settings where comprehensive laboratory workups may be limited, such as nights or weekends. In such cases, a positive LFD result could support the diagnostic algorithm in place of BAL-GM, potentially enabling the timely initiation of mold-active treatment in patients with suspected IPA. However, given the lack of large-scale clinical trials validating rapid testing systems, IPA diagnoses should still be reevaluated by conventional methods and established biomarkers, as outlined in diagnostic frameworks such as the FUNDICU criteria.
Therefore, we conclude that LFD testing could serve as an important tool for quickly diagnosing IPA in time-critical ICU situations. However, it is not sufficient to fully rule out IPA, and a comprehensive workup including biomarkers and microbiological techniques remains essential.
Supplementary Material
ofaf256_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hatzl S, Geiger C, Kriegl L, et al Performance of diagnostic algorithms in patients with invasive pulmonary aspergillosis. Clin Infect Dis. Published online 20 December 2024. doi:10.1093/cid/ciae 63310.1093/cid/ciae 633PMC 1213591239703147 · doi ↗ · pubmed ↗
- 2Bassetti M, Giacobbe DR, Agvald-Ohman C, et al Invasive fungal diseases in adult patients in intensive care unit (FUNDICU): 2024 consensus definitions from ESGCIP, EFISG, ESICM, ECMM, MSGERC, ISAC, and ISHAM. Intensive Care Med 2024; 50:502–15.38512399 10.1007/s 00134-024-07341-7PMC 11018656 · doi ↗ · pubmed ↗
- 3Blot SI, Taccone FS, Van den Abeele A, et al A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am J Respir Crit Care Med 2012; 186:56–64.22517788 10.1164/rccm.201111-1978 OC · doi ↗ · pubmed ↗
- 4Hamam J, Navellou J, Bellanger A, et al New clinical algorithm including fungal biomarkers to better diagnose probable invasive pulmonary aspergillosis in ICU. Ann Intensive Care 2021; 11:41–3.33683480 10.1186/s 13613-021-00827-3PMC 7938267 · doi ↗ · pubmed ↗
- 5Patterson TF, Thompson GR 3rd, Denning DW, et al Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis 2016; 63:e 1–60.27365388 10.1093/cid/ciw 326PMC 4967602 · doi ↗ · pubmed ↗
- 6Chun JY, Jeong S, Kim S, et al Performance of the galactomannan test for the diagnosis of invasive pulmonary aspergillosis using non-invasive proximal airway samples. J Infect 2024; 88:106159.38641139 10.1016/j.jinf.2024.106159 · doi ↗ · pubmed ↗
- 7Mercier T, Dunbar A, Veldhuizen V, et al Point of care Aspergillus testing in intensive care patients. Crit Care 2020; 24:642–7.33168049 10.1186/s 13054-020-03367-7PMC 7652676 · doi ↗ · pubmed ↗
- 8Vanderbeke L, Janssen NAF, Bergmans DCJJ, et al Posaconazole for prevention of invasive pulmonary aspergillosis in critically ill influenza patients (POSA-FLU): a randomised, open-label, proof-of-concept trial. Intensive Care Med 2021; 47:674–86.34050768 10.1007/s 00134-021-06431-0PMC 8164057 · doi ↗ · pubmed ↗