Unmasking Visceral Leishmaniasis: Nephrotic Syndrome as a Rare Pediatric Complication in Morocco
Ghizlane Kassal, Houda Nassih, Rabiy Elqadiry, Aicha Bourrahouat, Imane Aitsab

TL;DR
This paper reports two rare cases of children in Morocco with visceral leishmaniasis who developed nephrotic syndrome, highlighting the importance of early diagnosis and treatment.
Contribution
The paper presents two rare pediatric cases of nephrotic syndrome as a complication of visceral leishmaniasis in immunocompetent children.
Findings
Two children with visceral leishmaniasis developed nephrotic syndrome as a rare complication.
One child died, while the other improved with corticosteroids and antimonial drugs.
The cases emphasize the need for clinician awareness to enable early diagnosis and treatment.
Abstract
Nephrotic syndrome in children with visceral leishmaniasis (VL) is an uncommon presentation, often accompanied by other clinical signs such as febrile splenomegaly. This report highlights two cases of VL in immunocompetent children admitted to Mohamed VI University Hospital in Marrakech, who developed nephrotic syndrome as a complication. One child unfortunately passed away, while the other responded well to treatment with corticosteroids and pentavalent antimonial drugs, showing favorable clinical progress. This rare condition underscores the need to raise awareness among clinicians to facilitate early diagnosis and prompt treatment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
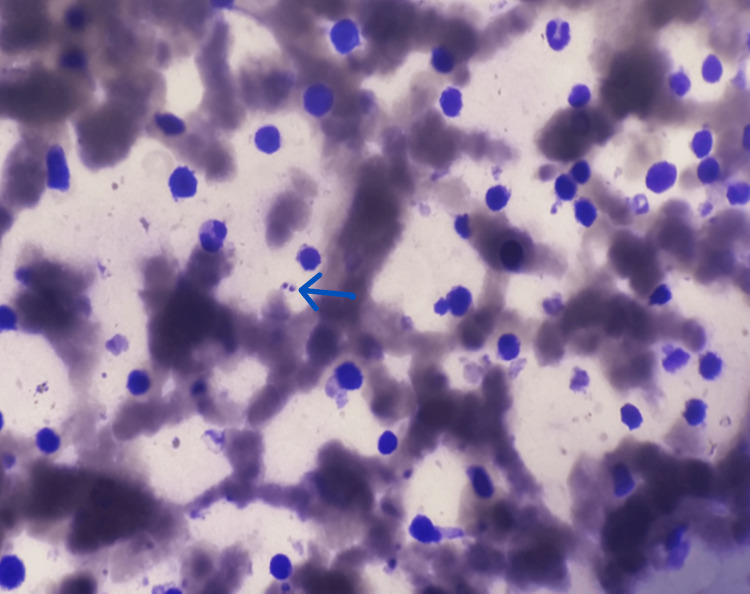 Figure 1
Figure 1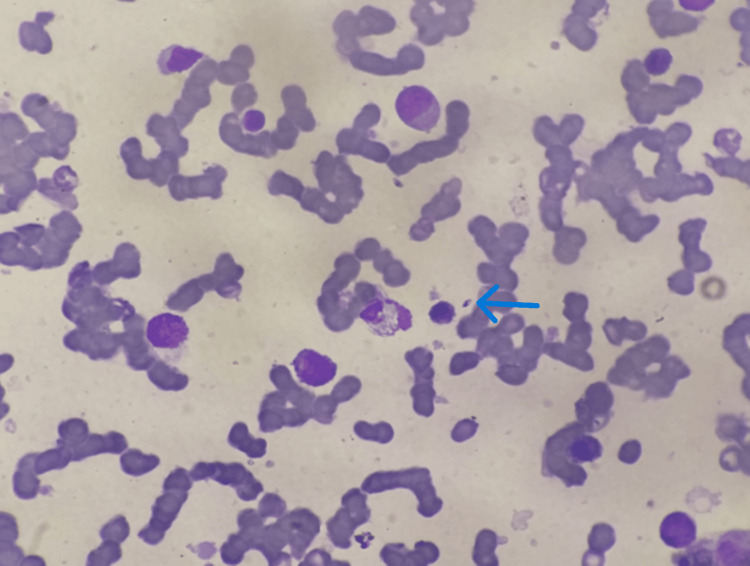 Figure 2
Figure 2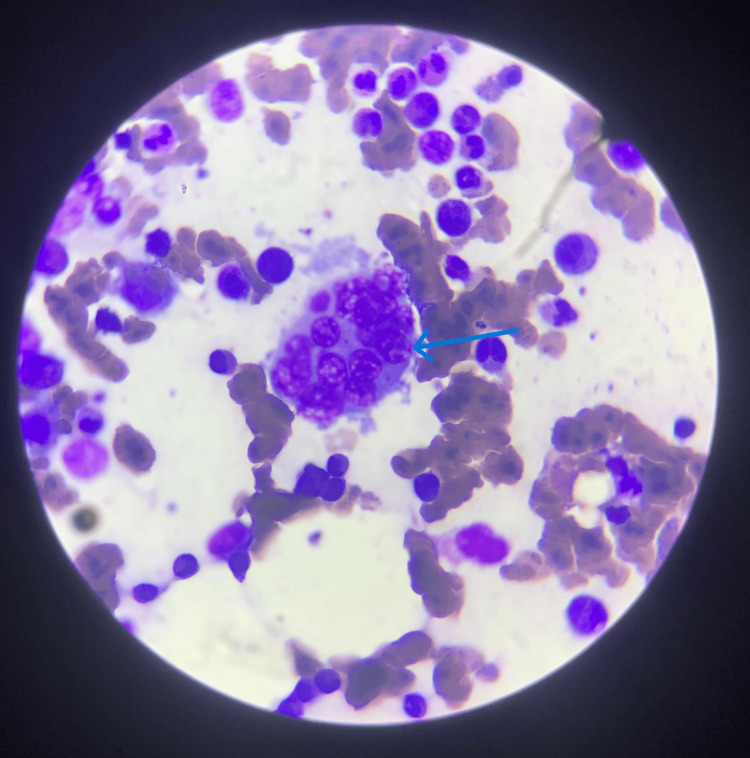 Figure 3
Figure 3| Variables | Case 1-Child: (VL+MAS+NS) | Case 2-Infant: (VL+NS) | ||
| Initial assessment | Day 5 | Initial assessment | Day 7 | |
| Leukocytes | 1300 (7000-13000) | 2100 | 1500 (3800-10400) | 3000 |
| Hemoglobin (Hb, g/dL) | 6.3 (10-12) | 7.5 | 5.3 (11-14) | 12 |
| Platelets | 30000 (185000-399000) | 40000 | 45000 (150000-450000) | 139000 |
| Albumin (g/L) | 18.6 (25-49) | 23 | 32 (35-48) | 13 |
| TP (%) | 80 (70-100) | 30 | 90 (70-100) | 100 |
| GPT (U/l) | 35 (9-25) | 850 | 35 (9-25) | 40 |
| GOT (U/l) | 46 (21-44) | 973 | 40 (18-36) | 25 |
| Ferritin (ng/mL) | 100 (5.3-99.9) | 833 | 750 (13.7-78.8) | 150 |
| Triglyceride (mg/dL) | 6.1 (25-119) | 365 | 200 (22-131) | 30 |
| Fibrinogen (g/L) | 2.0 (1.57-4.0) | <1.1 | 2.5 (1.7-4.09) | 3.2 |
| LDH (U/L) | 3.8 (192-321) | 700 | 411 (170-283) | 195 |
| GFR (mL/min) | 140 (95-150) | 51 | 140 (95-150) | 120 |
| 24-hour proteinuria (mg/kg/24h) | 63.75 (<5) | - | ND | ND |
| Uprot/Ucr ratio | ND | ND | ND | 3.1 (<0.2) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsResearch on Leishmaniasis Studies · Autoimmune and Inflammatory Disorders Research · Endometriosis Research and Treatment
Introduction
Leishmaniasis is a vector-borne tropical disease caused by intracellular protozoa of the genus Leishmania. Its clinical spectrum varies from self-limiting cutaneous ulcers to severe systemic, multi-organ involvement. The disease manifests primarily as visceral leishmaniasis (VL, or kala-azar), cutaneous leishmaniasis (CL), and mucocutaneous leishmaniasis (MCL). VL affects 0.2-0.4 million people annually [1,2]. The definitive diagnosis of VL relies on the identification of the parasite in samples obtained from bone marrow, spleen, or lymph nodes, which remains the diagnostic gold standard.
Renal impairment may result from various factors, including anemia, hypoalbuminemia, hypovolemia, and direct renal toxicity. Histological analysis often reveals changes such as tubulointerstitial nephritis, proliferative glomerulonephritis, and proximal tubulopathy [3,4]. Severe nephrotic-range proteinuria in VL has been reported exclusively in cases associated with either HIV or amyloidosis [4].
We report two cases of nephrotic syndrome as a complication of VL in immunocompetent children. These cases were managed in the Pediatric Department at Mohamed VI University Hospital in Marrakech, a public healthcare institution in Morocco. To the best of our knowledge, these represent the first documented cases of their kind in Morocco.
Case presentation
Case 1
It’s about a 10-year-old child from Ouarzazate, a Moroccan city known for its endemic leishmaniasis. The child was admitted with fever and hemorrhagic syndrome persisting for about a month. There was no history of recurrent infections or chronic diarrhea. Clinical examination revealed hepato-splenomegaly (HPSM) and a left leg ulcer measuring 5 cm × 4 cm. The child weighed 32 kg and measured 140 cm in height, both within the mean standard deviations. Edema was noted in the lower limbs and facial puffiness.
A urine dipstick (UD) test indicated massive proteinuria (+++), without hematuria. Nephrotic syndrome was confirmed with hypoalbuminemia (18.6 g/L) and 24-hour proteinuria (63.75 mg/kg/24 hours). Pancytopenia was observed in the blood count, and bone marrow aspiration confirmed the presence of Leishmania amastigotes (Figure 1 and Table 1).
Bone Marrow Aspiration Showing Leishmania Amastigotes (Blue Arrow)
HIV serology was negative. Treatment with Glucantime at 60 mg/kg/day was initiated, leading to a gradual decrease in the edematous syndrome.
However, after five days, the patient developed respiratory distress, acute renal failure (glomerular filtration rate: GFR 51 mL/min), and hepatocellular failure, prompting discontinuation of Glucantime. Macrophage activation syndrome (MAS) was diagnosed based on fever, splenomegaly, pancytopenia, hypertriglyceridemia (365 mg/dL), hypofibrinogenemia (≤1.1 g/L), and hyperferritinemia (833 u/ml) (Table 1). Methylprednisolone boluses (1 g/1.73 m^2^/day) and oral corticosteroid therapy were administered. Despite adequate management, the patient’s condition worsened, leading to multivisceral failure and death on the 15th day of hospitalization.
Case 2
A two year and six months old child, without a pathological history, residing in Ouarzazate, was admitted with a significant decline in general health following a prolonged six-month fever. He weighed 13 kg (below -1 SD) and measured 92 cm in height (mean SD). Clinical and biological assessments revealed HPSM and pancytopenia, with a GFR of 140 mL/min. Serological tests and a myelogram confirmed VL (Figure 2).
Bone Marrow Aspiration Showing Leishmania Amastigotes (Blue Arrow)
The presence of hemophagocytosis, along with elevated lactate dehydrogenase (LDH) (411 U/L) and ferritin (750 U/L) levels, led to the diagnosis of associated MAS (Table 1, Figure 3, and Appendix A).
Bone Marrow Aspiration Showing Hemophagocytic Activity (Blue Arrow)
Treatment consisted of three intravenous boluses of methylprednisolone (1 g/1.73 m^2^/day), followed by oral corticosteroid therapy, resulting in rapid clinical improvement. Glucantime was started as early as the seventh day after corticosteroid therapy.
In addition, the child developed peripheral edema with ascites and proteinuria confirmed using the UD. Nephrotic syndrome was diagnosed based on hypoalbuminemia (13 g/L) and a urinary protein-to-creatinine (Uprot/Ucr) ratio of 3.1 g/g. HIV serology was negative. The child was treated with an albumin infusion, resulting in a favorable clinical outcome, with proteinuria resolving entirely after 28 days of therapy. No relapse was observed during a one-year follow-up period.
Discussion
Leishmaniasis occurs not only in tropical regions but also in semi-tropical areas. Over 90% of VL cases are concentrated in six countries. VL primarily affects children and is a life-threatening disease if left untreated [1,2]. In Morocco, as well as in Algeria and Tunisia, VL is predominantly caused by Leishmania infantum (90%). Clinically, it manifests as a febrile illness associated with weight loss, pancytopenia, hepatosplenomegaly, and lymphadenopathy, with potential complications such as acute renal damage [5-7]. Renal involvement can encompass both tubular and glomerular dysfunction, resulting in proteinuria and hematuria [8,9]. Massive proteinuria can be a defining feature of nephrotic syndrome, which is clinically characterized by the presence of edema, hypoalbuminemia (serum albumin <25 g/L), and nephrotic-range proteinuria, typically defined as ≥40 mg/m^2^/hour or a Uprot/Ucr ratio exceeding 200 mg/mmol in a spot urine sample [10].
Glomerulopathy in VL is thought to result from immune complex deposition, driven by the polyclonal activation of B lymphocytes induced by the parasite. However, research suggests that other immune system components, such as macrophages, T cells, and cytokines, may play a more significant role than immune complexes in certain cases [11]. Additionally, Leishmania parasites can directly invade kidney tissue, causing localized damage [12].
As noted in the literature, the two cases described in this study illustrate nephrotic syndrome as a rare complication of VL in children. Pentavalent antimony salts remain the most widely used treatment for VL; however, their nephrotoxic potential increases in cases of overdose or impaired renal function. Liposomal amphotericin B (AmBisome) offers a less nephrotoxic alternative and enhances intramacrophagic penetration of antileishmanial therapies.
The second case had severe hepatic impairment, such as hepatocellular insufficiency, alongside renal impairment, which made the treatment available in our context (Glucantime) impossible. In addition, due to the lack of availability of AmBisome, no treatment was established. And severe thrombocytopenia further complicated, making renal puncture biopsy impossible.
High-dose corticosteroid therapy combined with antileishmanial agents appears to be crucial in managing severe renal impairment, especially when its origin is immune-mediated. This therapeutic approach was effectively administered to the patients in this study.
Conclusions
VL is an uncommon yet notable cause of secondary nephrotic syndrome in children. Its potential should be particularly considered for pediatric patients residing in endemic regions. Raising clinicians’ awareness of this condition and its possible nephrotic complications is crucial, as it enables timely diagnosis and appropriate treatment, ultimately improving patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Childhoodvisceral leishmaniasis Indian J Med Res Bhattacharya SK Sur D Karbwang J 353356123200616778316 · pubmed ↗
- 2Leishmaniasis worldwide and global estimates of its incidence P Lo S One Alvar J Vélez ID Bern C 07201210.1371/journal.pone.0035671 PMC 336507122693548 · doi ↗ · pubmed ↗
- 3Renal involvement in visceral leishmaniasis Am J Kidney Dis Dutra M Martinelli R de Carvalho EM Rodrigues LE Brito E Rocha H 222761985402532510.1016/s 0272-6386(85)80034-2 · doi ↗ · pubmed ↗
- 4Kidney involvement in leishmaniasis - a review Braz J Infect Dis Silva Junior GB Barros EJ Daher Ede F 4344401820142469043110.1016/j.bjid.2013.11.013PMC 9427481 · doi ↗ · pubmed ↗
- 5Post-kala-azar dermal leishmaniasis: does it play a role in the transmission of Leishmania donovani in the Sudan?Trop Med Int Health El Hassan AM Khalil EA 743744620011155544310.1046/j.1365-3156.2001.00776.x · doi ↗ · pubmed ↗
- 6Leishmaniasis in Sudan. 3. Visceral leishmaniasis Trans R Soc Trop Med Hyg Zijlstra EE El-Hassan AM 095200110.1016/s 0035-9203(01)90218-411370250 · doi ↗ · pubmed ↗
- 7Epidemiology and clinical manifestations of Leishmania donovani infection in two villages in an endemic area in eastern Sudan Trop Med Int Health Khalil EA Zijlstra EE Kager PA El Hassan AM 3544720021185195310.1046/j.1365-3156.2002.00832.x · doi ↗ · pubmed ↗
- 8Involvement of the renal function in patients with visceral leishmaniasis (kala-azar) [Article in Portuguese]Rev Soc Bras Med Trop Salgado Filho N Ferreira TM Costa JM 2172213620031280645710.1590/s 0037-86822003000200004 · doi ↗ · pubmed ↗