From Immersion to Seizure: A Novel Case of Water Intoxication Complicating a Water Birth
Sarah Al-Musawi, Rukhsana Iqbal, Greeshma Rajeev

TL;DR
A woman developed a seizure after a water birth due to dangerously low sodium levels, highlighting risks of prolonged water immersion and fluid intake.
Contribution
This case report identifies water intoxication as a potential complication of water immersion birth, emphasizing the need for fluid balance monitoring.
Findings
A 33-year-old woman developed severe hyponatremia and a seizure after a water immersion birth.
Prolonged immersion and fluid intake may lead to dilutional hyponatremia and water intoxication.
Monitoring fluid balance and serum sodium levels is recommended during prolonged water births.
Abstract
Water immersion birth (WIB) is increasingly used for pain relief during labour, offering high maternal satisfaction and reduced need for epidural analgesia. However, its potential complications, particularly regarding fluid and electrolyte balance, remain underexplored. We report a case of a healthy 33-year-old woman who developed a generalized tonic-clonic seizure two hours after delivering via WIB. Her antenatal course and labour progression were clinically normal; however, she experienced retention of urine and continued fluid intake during her four hours of immersion. Post-seizure investigations revealed serum sodium measured at 124 mmol/L indicated severe hyponatremia and metabolic acidosis. Neurological imaging and EEG were unremarkable. With supportive care and correction of sodium levels, her condition stabilized. This case highlights the possibility of dilutional hyponatremia…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
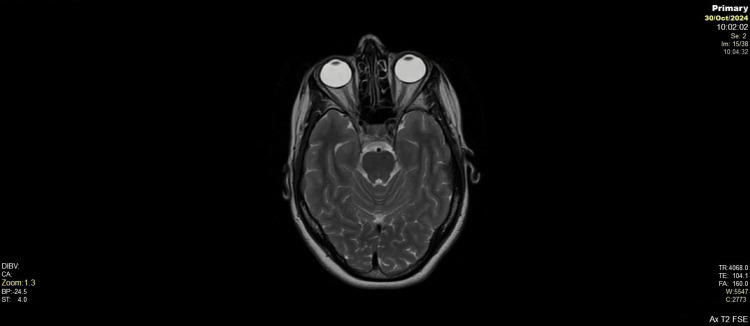 Figure 1
Figure 1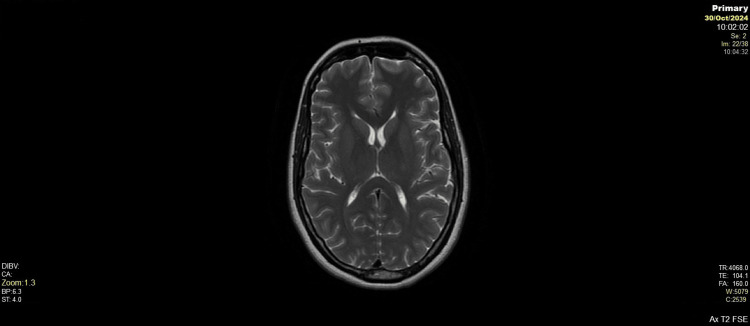 Figure 2
Figure 2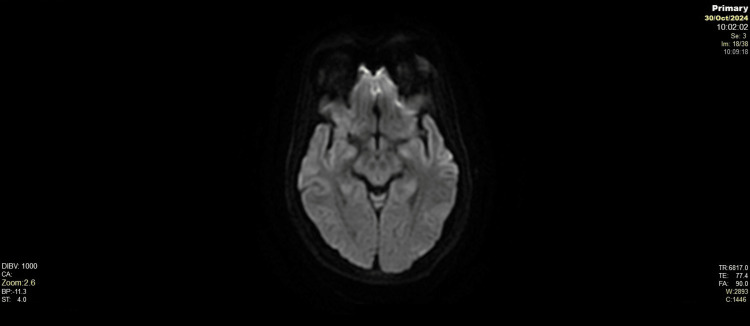 Figure 3
Figure 3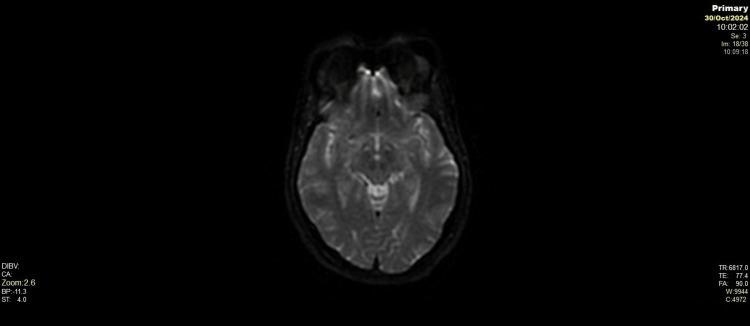 Figure 4
Figure 4| Component | Initial Value | After One Day Value | Units | Normal Range |
| WBC | 23.2 | 10.1 | x10^9/L | 4.0-11.0 |
| RBC | 4.74 | 3.72 | x10^12/L | 3.80-5.80 |
| HB | 129 | 109 | g/L | 115-165 |
| PCV | 0.390 | 0.301 | L/L | 0.370-0.470 |
| MCV | 82.3 | 80.9 | fL | 76.0-97.0 |
| MCH | 27.2 | 27.5 | pg | 27.0-33.0 |
| MCHC | 331 | 339 | g/L | 300-360 |
| RDW | 14.1 | 13.9 | % | 9.0-15.0 |
| Platelets | 233 | 175 | x10^9/L | 150-450 |
| MPV | 12.7 | 12.4 | fL | 7.5-11.0 |
| Neutrophils | 19.2 | 8.4 | x10^9/L | 2.0-7.5 |
| Lymphocytes | 2.3 | 1.2 | x10^9/L | 1.5-4.0 |
| Monocytes | 1.6 | 0.5 | x10^9/L | 0.2-1.0 |
| Eosinophils | 0.1 | 0.0 | x10^9/L | 0.0-0.5 |
| Basophils | 0.1 | 0.0 | x10^9/L | 0.0-0.2 |
| NRBCs | 0.0 | 0.0 | x10^9/L | 0.0-0.1 |
| CRP | 8 | 19 | mg/L | <5 |
| Bilirubin | 16 | 8 | µmol/L | 0-21 |
| ALT | 27 | 22 | IU/L | <33 |
| Albumin | 39 | 31 | g/L | 35-50 |
| Alk. Phos | 142 | 106 | U/L | 30-130 |
| Total protein | 67 | 49 | g/L | 60-80 |
| Lactate | 13.56 | 1.44 | mmol/L | 0.50-2.20 |
| TSH | 2.77 | - | mIU/L | 0.27-4.20 |
| Amylase | 88 | - | IU/L | 28-100 |
| Sodium | 124 | 134 | mmol/L | 133-146 |
| Potassium | 3.2 | 4.2 | mmol/L | 3.5-5.3 |
| Urea | 2.4 | 1.8 | mmol/L | 2.1-7.1 |
| Creatinine | 64 | 65 | µmol/L | 45-84 |
| eGFR | >90.0 | >90.0 | ml/min/1.73m² | >90.0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElectrolyte and hormonal disorders · Anesthesia and Neurotoxicity Research · Renal function and acid-base balance
Introduction
Water immersion during labour and birth is gaining popularity in numerous nations, especially within midwifery-led care environments. Water immersion birth (WIB) is associated with a reduced need for epidural anaesthesia without affecting the mode of delivery or the rate of perineal tears [1]. In England, 6,264 out of 46,088 low- and intermediate-risk singleton term spontaneous vaginal births were delivered using WIB (representing 13.6% of births in 35 NHS Trusts) [2]. Peripartum hyponatremia is a rare condition related mainly to water intoxication that is associated with a high intake of hypotonic fluids, or it could be a result of the use of oxytocin [3]. Oxytocin acts on the V2 (vasopressin) receptor in the kidney leading to water retention; both endogenous and exogenous had affinity for these receptors explaining the possible association with dilutional hyponatremia [4]. An association between WIB and hyponatremia has not been reported previously; interestingly, prior studies investigated the effects of WIB in the initial 60 minutes or less with no additional maternal oral fluid intake which could lead to further haemodilution and the subsequent hyponatremia [5]. Water immersion has also been found to increase the rate of water retention mainly by the increased production of vasopressin as suggested by Gabrielsen et al. [6]; this water retention in addition to the oral and intravenous fluids increases the possibility of hyponatremia in WIB. The management of hyponatremia depends on correction of the cause and volume status; in more severe forms, intravenous hypertonic saline is used [7]. We present a case of a healthy woman who developed a generalized seizure (single episode) after waterbirth that was attributed to hyponatremia, highlighting the importance of careful monitoring of fluid balance during waterbirth.
Case presentation
A 33-year-old woman, pregnant with her second child, arrived at the delivery ward at 41 weeks and three days of gestation after she had started to labour spontaneously, and she had a rupture of her membrane two hours prior to labour ward admission. She had a body mass index (BMI) of 30 and a posterior placenta which was not low, with foetal growth estimated between the 10th and 50th percentiles. Her pregnancy was otherwise uncomplicated, although she had reported a family history of epilepsy in her maternal relatives and a personal history of febrile seizures in childhood.
Upon admission, her vital signs were stable: blood pressure 139/88 mmHg, pulse 82 beats per minute, oxygen saturation 96%, and temperature 36.7°C. A vaginal examination revealed a 5-cm-dilated cervix, the baby’s head was at -2 station (mid-pelvis), and the head position was occiput posterior. Contractions were occurring three times every 10 minutes. The patient expressed a preference for a water birth, which was approved after an assessment found no contraindications.
During labour, she received oral dihydrocodeine, paracetamol, inhaled nitrous oxide (Entonox), intramuscular pethidine for pain relief, and intramuscular cyclizine. No oxytocin was given as the patient already had efficient uterine contractions. The water immersion continued for four hours in total. Despite adequate fluid intake, she did not pass urine for three hours. A urinary catheter drained 1,000 mL of urine, prompting close monitoring of fluid intake and output. At 19:38, she delivered a healthy male infant weighing 3.7 kg with Apgar scores of 8 at one minute and 10 at five and 10 minutes. Blood loss was minimal (200 mL), and the third stage of labour was actively managed.
Two hours following delivery, the patient experienced a sudden generalized tonic-clonic seizure without warning. Her husband supported her head during the 20-second episode, preventing injury. She briefly appeared cyanosed but did not have hypersalivation or lose bladder/bowel control. Post-seizure, she remained confused for three hours. Initial assessments revealed low oxygen saturation (89%), which improved to 99% with 15 L/min oxygen via a non-rebreathe mask. Blood tests showed hyponatremia (sodium 124 mmol/L), elevated lactate (13.56 mmol/L), and metabolic acidosis (pH 7.12, base deficit -14.4). Other notable results included a raised white cell count (23.2 ×10⁹/L), C-reactive protein (8 mg/L), and mild hypokalaemia (3.2 mmol/L); blood investigations just after the seizure and after one day are shown in Table 1.
Based on clinical signs, elevated inflammatory markers, and metabolic acidosis, empirical antibiotics were started following local sepsis protocols. Once blood cultures returned negative and the patient improved clinically, antibiotics were stopped.
The neurology team recommended correction of hyponatremia with slow intravenous fluids, a sepsis workup, and initiation of levetiracetam (1,500 mg oral loading dose followed by 500 mg twice daily). Intravenous co-amoxiclav was administered empirically. Over 24 hours, her sodium levels normalized, WBC on the second day was 10.1, and her mental clarity returned. Later on, blood culture came back negative. Follow-up brain MRI (shown in Figures 1-4) and electroencephalogram (EEG) showed no abnormalities. She was discharged in a stable condition with outpatient neurology follow-up; the antiepileptic medications were stopped after the results of EEG and MRI.
Brain axial T2-weighted MRIAxial T2-weighted MRI showing no central pontine demyelination, normal brainstem, cerebellum, temporal lobes, and basal cistern anatomy. No lesions, oedema, or structural abnormalities noted.
Axial T2-weighted MRI at lateral ventriclesNo evidence of cerebral oedema or abnormal signal intensity on T2-weighted axial images. The brain parenchyma appears normal with preserved grey-white matter differentiation. No signs of PRES or other postpartum-related intracranial abnormalities are identified.
Axial diffusion-weighted imaging (DWI)No areas of restricted diffusion seen on DWI, excluding acute ischemia or cytotoxic oedema. Findings are within normal limits.
Axial apparent diffusion coefficient (ADC) mapAxial ADC map confirms normal diffusion patterns across the brain with no reduction suggestive of ischemia or cytotoxic oedema. Cerebellum, brainstem, and cerebral hemispheres demonstrate homogenous diffusion properties.
Discussion
Hyponatremia in healthy peripartum women is an underreported condition that needs careful consideration and active investigation [3]. Water immersion birth is widely considered a safe and effective method to reduce pain and increase maternal satisfaction; it also presents physiological challenges that are not yet fully understood, particularly regarding fluid and electrolyte homeostasis [2].
Thaker [8] found that women were more prone to develop hyponatremia in the peripartum period, and it could be either a dilutional or a non-dilutional type. The dilutional hyponatremia is caused by higher intake of water, either intravenously or orally, in addition to the effect of oxytocin (both endogenous and exogenous), which acts as a potent antidiuretic hormone, leading to pronounced water retention and increasing the possibility of dilutional hyponatremia. In this case report, the patient continued to take oral fluid with initial delayed diuresis (for three hours) could be attributed to fluid retention contributing to dilutional hyponatremia.
Water immersion affects the body physiology in different mechanisms as the external pressure of the water on the body leads to redistribution of blood volume, promoting central volume expansion and the release of atrial natriuretic peptide (ANP) and suppression of renin and aldosterone, as suggested by Stadeager et al. [9]. Furthermore, immersion may also stimulate non-osmotic release of arginine vasopressin (AVP), impairing the kidneys’ ability to excrete free water and predisposing to water retention and hyponatremia [6,10]. Previous studies on water immersion mostly focused on short-term exposures to immersion and no actual consideration to ongoing fluid intake throughout labour. The current case findings highlight the importance of monitoring the fluid input in prolonged immersion as this led to additional water retention leading to a clinically significant hyponatremia.
The neurological presentation was consistent with acute symptomatic hyponatremia as a probable contributing factor to seizure, characterized by sudden onset, postictal confusion, and low serum sodium (124 mmol/L). Elevated lactate and metabolic acidosis further reflect the physiological stress associated with this seizure activity. The elevated WBC noticed initially could be explained by the period of hypoxia during the seizure attack as suggested by Huang et al. [11]. However, the possibility of concurrent infection cannot be entirely ruled out. The use of empirical antibiotics was based on initial elevated white cell count, CRP, and acidosis.
Previous studies found case of hyponatremia-induced seizure at Na level of 124 mmol/L (Halawa et al. [12]) is rare, but it is not a never incident. This highlights the importance of this case report as the patient was more prone to develop seizure even with minimal hyponatremia.
Transient urinary retention in this case may have further contributed to impaired free water clearance, compounding the dilutional effect of continued oral fluid intake during immersion. Although water intoxication-induced maternal seizure was reported previously (Walter et al. [13]), this is the only case that could connect the WIB directly to hyponatremia-induced maternal seizure. This case report highlights the importance of careful monitoring of fluid balance in WIB to avoid unpredicted electrolyte disturbance and minimizing maternal mortality in post-partum period.
Limitation of the study
There was no report of sodium level prior to the start of water immersion for the comparison. The water intake from the patient was not measured/not documented, and this could be further cause of water intoxication.
Conclusions
Water immersion birth could be associated with an increased risk of water retention, and unregulated intake of water could lead to a cumulative effect resulting in symptomatic hyponatremia and potential maternal seizure. Careful patient selection, vigilant fluid balance monitoring, and sodium measurement should be considered, especially in cases of prolonged immersion or abnormal urinary output. This case highlights the importance of balancing the known benefits of WIB with the potential risk of water intoxication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Immersion in water during labour and birth Cochrane Database Syst Rev Cluett ER Burns E Cuthbert A 05201810.1002/14651858.CD 000111.pub 4PMC 649442029768662 · doi ↗ · pubmed ↗
- 2Waterbirth: a national retrospective cohort study of factors associated with its use among women in England BMC Pregnancy Childbirth Aughey H Jardine J Moitt N 2562120213377111510.1186/s 12884-021-03724-6PMC 8004456 · doi ↗ · pubmed ↗
- 3Severe hyponatremia in obstetrics: presentations and outcome. Retrospective cohort over 10 years Int J Gynaecol Obstet Elbarbary N Datta T Viswanatha R Johnstone H Shehata H Ganapathy R 1026103016820253944557910.1002/ijgo.15939 · doi ↗ · pubmed ↗
- 4Water balance during parturition and early puerperium: a prospective open trial Clin Biochem Risberg A Sjöquist M Wedenberg K Olsson U Larsson A 8378424820152610234310.1016/j.clinbiochem.2015.06.012 · doi ↗ · pubmed ↗
- 5Systematic review of case reports of poor neonatal outcomes with water immersion during labor and birth J Perinat Neonatal Nurs Vanderlaan J Hall P 3113233420203307980510.1097/JPN.0000000000000515 · doi ↗ · pubmed ↗
- 6Arterial pulse pressure and vasopressin release during graded water immersion in humans Am J Physiol Regul Integr Comp Physiol Gabrielsen A Warberg J Christensen NJ Bie P Stadeager C Pump B Norsk P 08278200010.1152/ajpregu.2000.278.6.R 158310848527 · doi ↗ · pubmed ↗
- 7Diagnosis and management of hyponatremia: a review JAMA AdroguéHJ Tucker BM Madias NE 28029132820223585252410.1001/jama.2022.11176 · doi ↗ · pubmed ↗
- 8Recognizing and avoiding significant maternal hyponatremia J South Asian Fed Obstet Gynaecol Thaker S 100103122020