The MATTERHORN trial: Percutaneous MitraClip vs surgical repair in heart-failure-related secondary mitral regurgitation
Susy Kotit

TL;DR
The MATTERHORN trial compared MitraClip and surgical repair for heart failure-related mitral regurgitation, finding similar effectiveness but fewer short-term risks with MitraClip.
Contribution
This trial provides the first direct comparison of transcatheter and surgical repair for secondary mitral regurgitation in high-risk patients.
Findings
M-TEER showed noninferiority to surgery for key outcomes at 1 year.
M-TEER had fewer major adverse events within 30 days but higher MR recurrence.
Surgical repair had lower MR recurrence but higher short-term risks.
Abstract
Introduction: Functional mitral regurgitation (FMR) is a common complication of heart failure and is associated with poor prognosis and increased morbidity and mortality. Surgical mitral valve repair (MVRe) and MitraClip transcatheter edge-to-edge repair (M-TEER) are used to improve FMR, however, there has not been sufficient comparison between the benefits of both approaches. The MATTERHORN trial aimed to compare the efficacy and safety outcomes of percutaneous versus surgical repair in high-risk patients with heart failure and FMR, to determine the noninferiority of transcatheter edge-to-edge therapy in this population. Study and results: 208 patients were randomized in a 1:1 ratio to either M-TEER with MitraClip device or surgical mitral valve repair or replacement. The average age was 70.5 ± 7.9 years, 39.9% were female, mean LVEF was 43.0 ± 11.7%, 85.7% of patients had NYHA…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
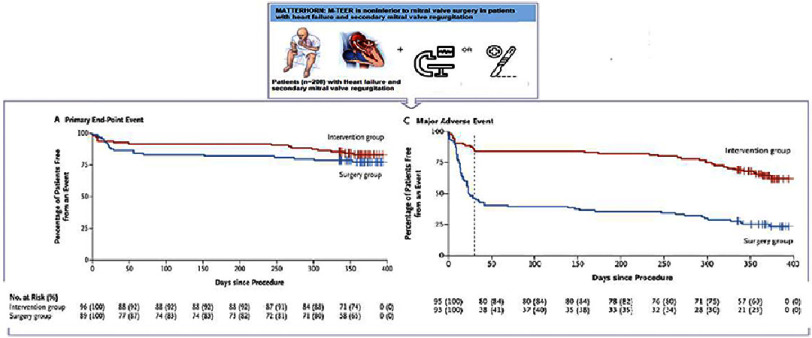 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair · Cardiac pacing and defibrillation studies
Introduction
Functional mitral regurgitation (FMR) resulting from left ventricular (LV) dysfunction, which impairs leaflet coaptation of a structurally normal mitral valve (MV), is a common complication of heart failure (HF), with moderate to severe mitral regurgitation (MR) affecting 24% to 59% of these patients^2–5^. FMR is associated with adverse outcomes, including increased morbidity and mortality^1, 6, 7^, aggravated by the underlying cardiac pathology. The one-year mortality rates for FMR typically range from 15–40%^5, 8–10^ and the advantages of mitral valve intervention remain uncertain^1^.
Medical management remains pivotal in FMR treatment^3, 11^, especially in advanced right or left HF, where the outcomes of MV interventions may offer limited benefits^12, 13^. Surgical mitral valve repair is recommended for suitable candidates according to current guidelines. In contrast, percutaneous approaches, notably MitraClip transcatheter edge-to-edge repair (M-TEER), are advised for patients at high surgical risk or with unfavorable anatomical considerations^11, 14^.
Although MV surgery can alleviate symptoms^19–21^, it is associated with operative risks and uncertain long-term benefits. Its impact on altering the natural progression of the primary disease (cardiomyopathy/LV dysfunction) or enhancing survival remains inconclusive^15–18^.
M-TEER has emerged as an alternative to surgery. The MitraClip device, a polyester-covered cobalt-chromium clip, is inserted via the femoral vein and guided into the left atrium (LA) through transseptal puncture under fluoroscopic and transesophageal echocardiography (TEE) guidance, which mimics the surgical Alfieri stitch by grasping and reducing MR-causing mitral leaflet edges ^1^. This procedure has been shown to improve symptoms^22–28^, enhance survival rates^22–28^, reduce heart failure-related hospitalizations, and enhance quality of life for select patients unresponsive to medical therapy ^1^.
However, there has not been a sufficient comparison between the benefits of surgery and M-TEER in HF-related FMR. The goal of the Multicenter Mitral Valve Reconstruction for Advanced Insufficiency of Functional or Ischemic Origin (MATTERHORN) trial was to compare the efficacy and safety outcomes of M-TEER versus surgical mitral valve repair in high-risk patients with heart failure and FMR and to determine the non-inferiority of transcatheter edge-to-edge therapy in this specific population.
Methods
The MATTERHORN trial was a multicenter, prospective, randomized, open-label, non-inferiority trial that compared the MitraClip system to reconstructive mitral valve surgery in the setting of depressed left ventricular ejection fraction (LVEF) and functional MR to determine whether transcatheter edge-to-edge therapy is non-inferior to mitral valve surgery in high-risk patients who are at high surgical risk.
Inclusion in the trial required clinically significant functional MR (grade 3+ or 4+) which was defined by meeting at least two of the following criteria: effective regurgitant orifice area of at least 20 mm 2 , biplane vena contracta width of more than eight mm, a regurgitant volume of at least 30 ml, a regurgitant fraction of at least 50%, or at least two hospitalizations for acute heart failure during the 12 months before enrolment, left ventricular ejection fraction (LVEF) ≥ 20%, symptoms of heart failure (New York Heart Association [NYHA] class ≥ 2) despite guideline-directed therapy, and eligibility for both transcatheter edge-to-edge repair or mitral-valve surgery as determined by the local heart team.
Patients were randomized in a 1:1 ratio to either M-TEER with MitraClip device (Abbott Vascular) or surgical mitral valve repair or replacement (Figure 1). For mitral valve surgery, surgical access and technique, including concomitant ablation procedures or tricuspid valve surgery, were left to the discretion of the surgeon. Procedures were performed according to local best practice.
MATTERHORN trial.
Patients were evaluated at baseline, at hospital discharge, 30 days and 1 year after the procedure. Standardized transesophageal and transthoracic echocardiographic examinations were performed before the procedure, before discharge, and 12 months after the procedure.
Key exclusion criteria included severe tricuspid regurgitation, other concomitant severe valve disorders, and coronary revascularization or cardiac resynchronization device implantation within 1 month prior to enrolment.
The primary efficacy endpoint was the composite of death from any cause, hospitalization for heart failure, mitral valve re-intervention, left ventricular assist device implantation, or stroke within 1 year after the procedure.
The key secondary efficacy endpoint was the recurrence of MR grade ≥3 (mitral regurgitation grade 3+ (moderate-to-severe disease) or 4+ (severe disease) at 1 year.
Additional secondary endpoints included the change in the 6-minute walk distance, New York Heart Association functional class, and Minnesota Living with Heart Failure Questionnaire score.
The primary composite safety endpoint assessed at 30 days included death (all-cause), myocardial infarction, major bleeding, stroke or transient ischemic attack, rehospitalization (all-cause), all reintervention or nonelective cardiovascular surgery, renal failure, deep wound infection, mechanical ventilation >48 h, gastrointestinal complications requiring surgery, new-onset atrial fibrillation (AF), septicemia, and endocarditis.
Results
A total of 208 patients were randomized, with 104 patients allocated to each study arm.
The average age was 70.5 ± 7.9 years and 39.9% were female. The mean LVEF was 43.0 ± 11.7%, and heart failure was NYHA class III or IV in 85.7% of patients.
Mitral regurgitation grade ≥ 3 was present in 96.0% of the patients (n = 191), of which 38.2% was grade 4+. Median effective regurgitant orifice area was 0.22 cm^2^ (0.17 to 0.28); and the mean regurgitant fraction was 57.0 ± 21.0%.
The median Society of Thoracic Surgeons Predicted Risk of Mortality score (range of scores, 0 to 100%, with higher scores indicating a greater risk of death within 30 days after the procedure) was 2.0 (interquartile range, 1.1 to 3.7), the median European System for Cardiac Operative Risk Evaluation (EuroSCORE) II score (range of scores, 0 to 100%, with higher scores indicating a greater risk of in-hospital death) was 3.0 (interquartile range.7 to 4.3), and 13.1% of the patients had received previous cardiac resynchronization therapy.
In the intervention group, transcatheter edge-to-edge repair was successful and resulted in a mitral regurgitation grade of ≤2 in 96.1% of patients at 1 year, 48.5% of patients received one device and 40.6% received two devices.
In the surgical group, 72.0% underwent mitral valve repair, and 28.0% underwent mitral valve replacement. Mitral surgery resulted in a mitral regurgitation grade of ≤2 in 98.6% of patients at 1 year.
At hospital discharge, the percentage of patients receiving a renin–angiotensin–aldosterone system inhibitor and the percentage receiving triple heart failure therapy was 81.4% in the intervention group and 57.9% in the surgery group.
Primary endpoint
A total of 96 patients (92.3%) in the intervention group and 89 (85.6%) in the surgery group had data available at 1 year. The median follow-up time was 370 days (range: 366–374 days) in the intervention group and 368 days (range: 364–372 days) in the surgery group.
At 1 year, at least one primary endpoint event—death, hospitalization for heart failure, mitral valve re-intervention, implantation of an assist device, or stroke—occurred in 16.7% of the M-TEER group and in 22.5% of the surgery group (estimated mean difference, −6 percentage points; 95% confidence interval [CI], −17 to 6; P < 0.001 for non-inferiority). The relative risk ratio was 0.74 (95% CI, 0.41 to 1.34). All-cause death occurred in 8.3% and 10.3% of patients in the M-TEER and surgery groups, respectively.
Mitral valve reintervention occurred in 5% of the M-TEER group and 2% of the surgical group, while implantation of an LV-assist device was required in 2% and 4% of patients, respectively. Stroke occurred in 1% of the M-TEER group and 4% of the surgical group.
Secondary endpoints
Recurrence of MR grade ≥ 3 at 1 year occurred in 8.9% of patients in the TEER group vs. 1.5% in the surgical group (estimated mean difference, 7 percentage points; 95% CI, 0 to 14; P = 0.02 for noninferiority).
The median change in the 6-minute walk distance from baseline to 1 year was 31 m (−56 to 85) in the intervention group and 32 m (−51 to 80) in the surgery group. The linear regression model adjusted for site and 6-minute walk distance at baseline yielded a regression coefficient of 5.22 (95% CI, −42.39 to 52.82), with the surgery group as the reference group (R 2 = 0.318). This confidence interval remained above −50 m, meeting the non-inferiority criterion.
At 1 year, 23.3% of the patients in the intervention group and 18.2% in the surgery group had New York Heart Association functional class III or IV heart failure, compared to 82.4% and 89.1% at baseline, respectively.
The median change in the Minnesota Living with Heart Failure Questionnaire (range of scores, 0–105, with higher scores indicating lower quality of life) at 1 year was −10 (−20 to 0) in the intervention group and −5 (−19 to 4) in the surgical group. In-hospital staya after intervention were 4 days and 12 days in the M-TEER and surgery groups, respectively.
Safety and adverse events
The safety endpoint, which was a composite of major adverse events within 365 (± 30) days after the procedure, occurred in 36.5% of patients in the intervention group and 75.3% in the surgery group (estimated mean difference, −39 percentage points; 95% CI, −51 to −25).
Major events during intervention occurred in three patients, including intraprocedural partial detachment of the clip in one patient and chordae rupture in two patients leading to valve replacement. Reinterventions were needed in eight patients in the surgery group, three of which were related to thoracic bleeding and four to deep wound infections.
At 30 days, 2.0% of the patients in the intervention group and 4.3% of those in the surgery group died. Major bleeding (as defined by the Valve Academic Research Consortium (VARC)) occurred in 3.1% of patients in the intervention group and 24.4% in the surgery group (estimated difference, −21 percentage points; 95% CI, −31 to −12). New-onset atrial fibrillation occurred in 3.1% of the patients in the intervention group and 27.8% in the surgery group (estimated difference, −25 percentage points; 95% CI, −35 to −15). Stroke did not occur in the patients in the intervention group at 30 days, in contrast to the 4.4% occurrence rate in the surgery group.
Overall, 41.0% and 77.3% of the patients in the intervention and surgery groups, respectively, experienced at least one adverse event. Serious adverse events occurred in 35.0% and 66.0% of patients in the intervention and surgery groups, respectively.
Discussion
The MATTERHORN trial is the first randomized trial to directly compare mitral transcatheter edge-to-edge repair (M-TEER) with surgery in patients with heart failure and functional mitral regurgitation eligible for mitral valve surgery, showing noninferiority of M-TEER in this patient cohort.
At one-year, the study revealed at least one primary endpoint event (death, heart failure hospitalization, mitral valve re-intervention, assist device implantation, or stroke) in 16.7% of the patients in the M-TEER group, in contrast to 22.5% in the surgery group.
While the surgical group experienced higher rates of all-cause mortality, LV-assisted device implantation, and stroke, mitral valve reintervention was more prevalent in the M-TEER group (5% vs. 2%). The recurrence of moderate-to-severe MR was notably higher in the TEER group (8.9% vs. 1.5%), with a 3% crossover to surgery within 12 months among TEER patients.
Both groups exhibited improvements in NYHA functional class, with the surgical group showing greater symptom enhancement and the intervention group displaying more favorable scores on the Minnesota Living with Heart Failure Questionnaire. The in-hospital stay after the intervention was longer in the surgical group.
A composite of major adverse events, including surgical bleeding, new-onset atrial fibrillation, and stroke, which are common postoperative sequelae, occurred more often in the surgery group.
Although both treatments effectively reduced MR severity, the M-TEER group demonstrated lower rates of procedural complications and faster recovery, offering substantial advantages, particularly for high-risk surgical patients. The MATTERHORN trial demonstrated the non-inferiority of mitral TEER compared to surgery for the composite endpoint at one year, with a favorable safety profile in heart failure patients with FMR, consistent with previous research showing reduced HF hospitalizations and mortality rates^29–31^.
This trial highlights M-TEER as a secure and efficient alternative to surgery for individuals with heart failure and functional mitral regurgitation, with a superior safety profile and non-inferior efficacy compared with conventional surgical methods, particularly beneficial for elderly populations and those unsuitable for surgery.
However, it is important to note that 1 year of follow-up is insufficient to determine the long-term outcomes of intervention or surgery, and extended follow-up is essential for both groups. As the patients were enrolled in the trial for more than seven years, a longer follow-up time should have been available. The noninferiority margin of 17.5% used in this study was also deemed too high. Furthermore, the loss to follow-up and consent withdrawal were significant, possibly affecting the results.
It is also essential to determine whether intervention (M-TEER or surgery) improves disease prognosis, as most of these patients have very poor survival due to ventricular disease and more than 70% die at 5 years, regardless of the procedure ^1^. Therefore, it is crucial to compare the results presented in this study to those of a medical therapy arm, especially since almost half of the cohort had an LVEF greater than 40%, to determine the benefits and clinical significance of both strategies.
Conclusion
In patients with heart failure and functional MR, transcatheter edge-to-edge repair demonstrated non-inferiority to surgery for a composite of death, rehospitalization for heart failure, stroke, reintervention, or assist device implantation at one year.
M-TEER exhibited significantly fewer major adverse events within 30 days post-procedure, albeit with a slightly higher MR recurrence rate at one year. This study highlights the potential of M-TEER as a less invasive yet effective alternative to surgery for functional mitral regurgitation, mitigating surgical risks, and offering faster recovery, especially in patients deemed unsuitable for surgery. However, long-term data is crucial for guiding policies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Asgar AW Mack MJ Stone GW 2015 Secondary mitral regurgitation in heart failure: Pathophysiology, prognosis, and therapeutic considerations J Am Coll Cardiol 651212311248 doi: 10.1016/j.jacc.2015.02.00925814231 · doi ↗ · pubmed ↗
- 2Robbins JD Maniar PB Cotts W Parker MA Bonow RO Gheorghiade M 2003 Prevalence and severity of mitral regurgitation in chronic systolic heart failure Am J Cardiol 913360362 doi: 10.1016/s 0002-9149(02)03172-712565101 · doi ↗ · pubmed ↗
- 3Bartko PE Hülsmann M Hung J 2020 Secondary valve regurgitation in patients with heart failure with preserved ejection fraction, heart failure with mid-range ejection fraction, and heart failure with reduced ejection fraction Eur Heart J 412927992810 doi: 10.1093/eurheartj/ehaa 12932350503 PMC 8453270 · doi ↗ · pubmed ↗
- 4Chioncel O Lainscak M Seferovic PM 2017 Epidemiology and one-year outcomes in patients with chronic heart failure and preserved, mid-range and reduced ejection fraction: an analysis of the ESC Heart Failure Long-Term Registry Eur J Heart Fail 191215741585 doi: 10.1002/ejhf.81328386917 · doi ↗ · pubmed ↗
- 5Rossi A Dini FL Faggiano P 2011 Independent prognostic value of functional mitral regurgitation in patients with heart failure. A quantitative analysis of 1256 patients with ischaemic and non-ischaemic dilated cardiomyopathy Heart 972016751680 doi: 10.1136/hrt.2011.22578921807656 · doi ↗ · pubmed ↗
- 6Coats AJS Anker SD Baumbach A 2021 The management of secondary mitral regurgitation in patients with heart failure: a joint position statement from the Heart Failure Association (HFA), European Association of Cardiovascular Imaging (EACVI), European Heart Rhythm Association (EHRA), and Eu Eur Heart J 421312541269 doi: 10.1093/eurheartj/ehab 08633734354 PMC 8014526 · doi ↗ · pubmed ↗
- 7Camaj A Thourani VH Gillam LD Stone GW 2023 Heart failure and secondary mitral regurgitation: A contemporary review J Soc Cardiovasc Angiogr Interv 26, Part Bdoi: 10.1016/j.jscai.2023.10119510119539131058 PMC 11308134 · doi ↗ · pubmed ↗
- 8Perez de Isla L Zamorano J Quezada M 2006 Prognostic significance of functional mitral regurgitation after a first non-ST-segment elevation acute coronary syndrome Eur Heart J 272226552660 doi: 10.1093/eurheartj/ehl 28717015403 · doi ↗ · pubmed ↗