Bexagliflozin on Renal Outcomes in Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Marília Gobbo, Renan Y Ura Sudo, Tanize L Milbradt, Isabel Cristina Reinheimer, Matthew Min, Carlos E Poli-de-Figueiredo

TL;DR
This study reviews and analyzes the effects of bexagliflozin, a new SGLT2 inhibitor, on kidney-related outcomes in patients with type 2 diabetes.
Contribution
The study provides a meta-analysis of bexagliflozin's renal effects, which had not been previously systematically reviewed.
Findings
Bexagliflozin did not significantly change serum creatinine levels or estimated glomerular filtration rate.
It significantly reduced systolic blood pressure in patients.
No beneficial effect on kidney function was observed compared to other SGLT2 inhibitors.
Abstract
Sodium-glucose cotransporter-2 (SGLT2) inhibitors are important for treating type 2 diabetes mellitus (T2DM). However, it remains unclear whether the newest SGLT2 inhibitor, bexagliflozin, provides benefits for renal- or urinary-related outcomes. The ClinicalTrials.gov, PubMed, Embase, and Cochrane databases were searched for randomized controlled trials. Using R software version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria), a random-effects model was employed to compute mean differences (MD) and risk ratios for continuous and binary endpoints. The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach was used to rate the certainty of evidence. The International Prospective Register of Systematic Reviews (PROSPERO) identification number is CRD42023478336. Nine studies involving 4,352 patients were included. Over a follow-up that ranged…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
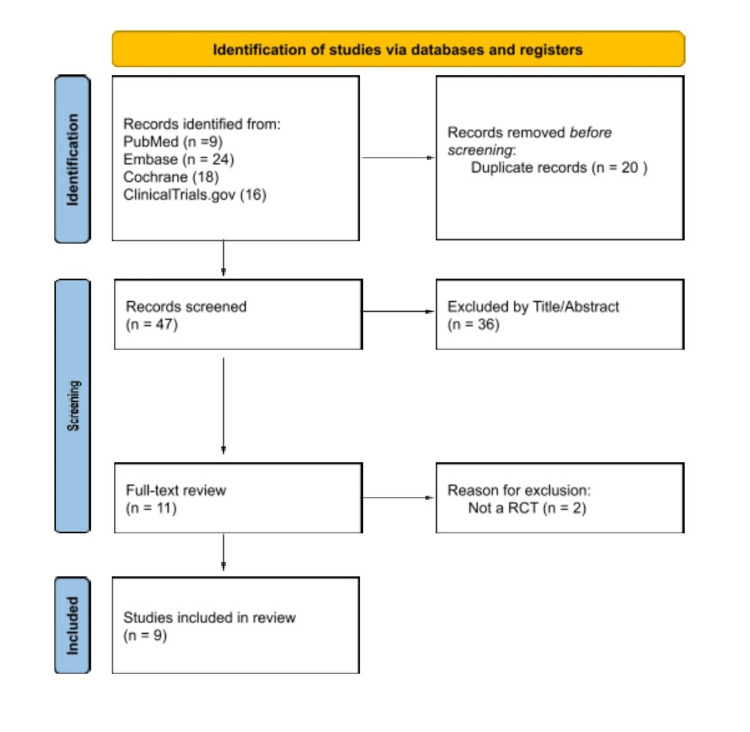 Figure 1
Figure 1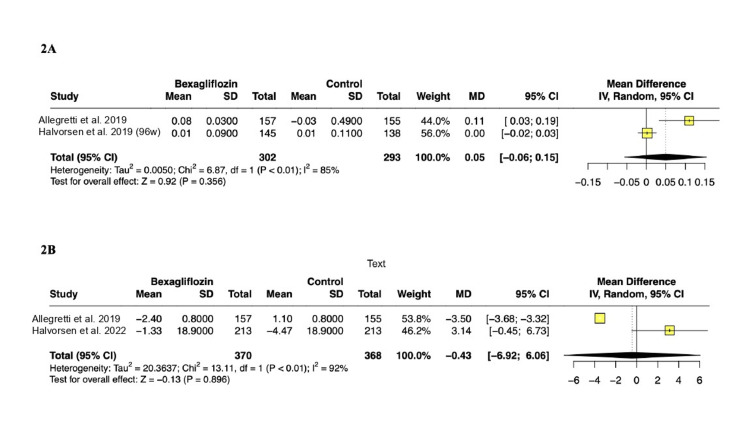 Figure 2
Figure 2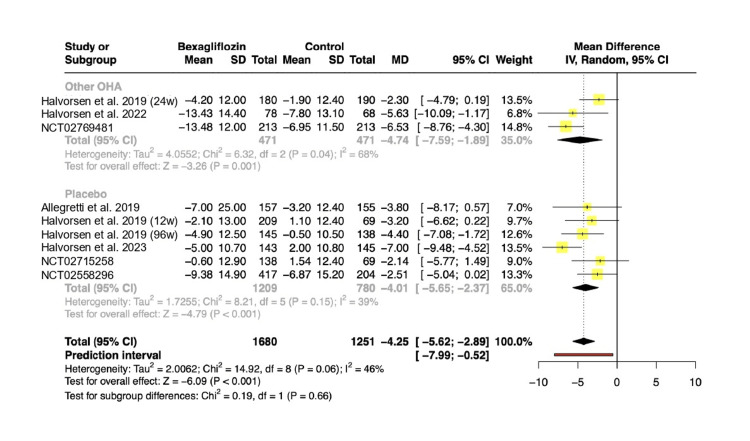 Figure 3
Figure 3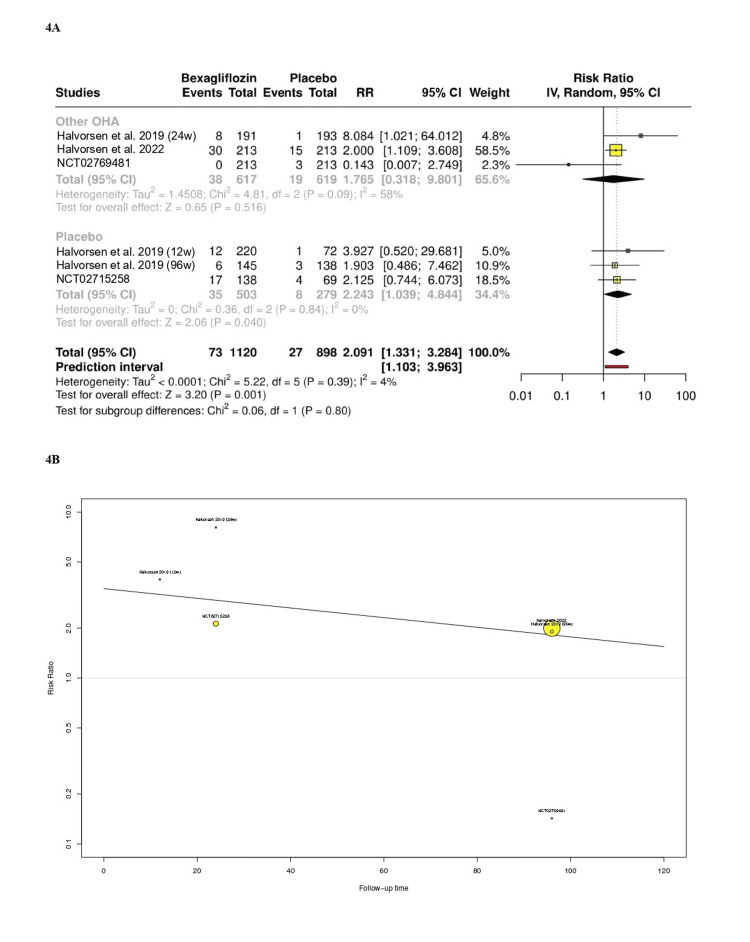 Figure 4
Figure 4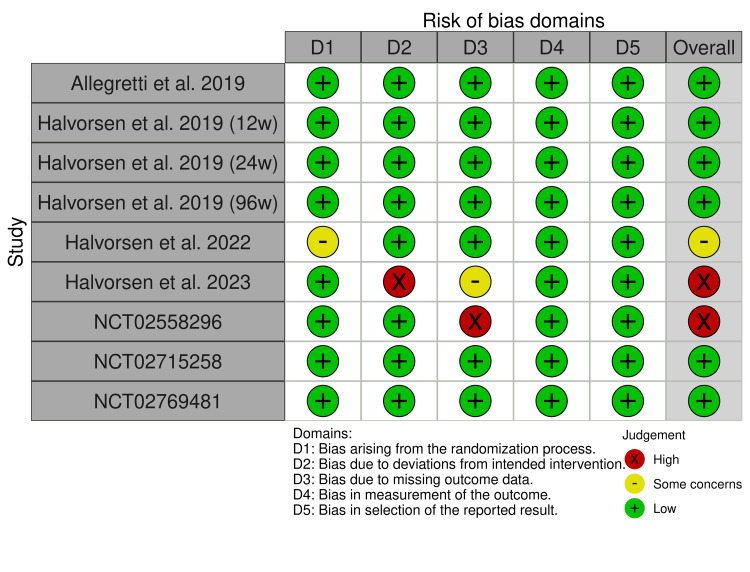 Figure 5
Figure 5| Study/characteristic | Allegretti et al. [ | Halvorsen et al. [ | Halvorsen et al. [ | Halvorsen et al. [ | Halvorsen et al. [ | Halvorsen et al. [ | |||
| Year of publication | 2019 | 2019 | 2019 | 2019 | 2022 | 2023 | 2021 | 2021 | 2021 |
| Intervention | Bexagliflozin | Bexagliflozin | Bexagliflozin and MTF | Bexagliflozin | Bexagliflozin | Bexagliflozin and MTF | Bexagliflozin and MTF | Bexagliflozin | Bexagliflozin |
| Intervention doses | 20 mg | 5 mg, 10 mg, and 20 mg | 20 mg | 20 mg | 20 mg | 20 mg | 20 mg | 20 mg | 20 mg |
| Control | PBO | PBO | Sitagliptin and MTF | PBO | Glimepiride | PBO and MTF | Glimepiride and MTF | PBO | PBO |
| Control doses | Not reported | Not reported | 100 mg | Not reported | 2-6 mg | Not reported | 2 mg, 4 mg, and 6 mg | Not reported | Not reported |
| Sample size, n (intervention) | 157 | 220 | 191 | 145 | 213 | 158 | 213 | 140 | 1133 |
| Sample size, n (control) | 155 | 72 | 193 | 138 | 213 | 159 | 213 | 70 | 567 |
| Follow-up, weeks | 24 | 12 | 24 | 96 | 96 | 24 | 96 | 24 | 24 |
| Study design | DB RCT | DB RCT | DB RCT | DB RCT | DB RCT | DB RCT | DB RCT | DB RCT | DB RCT |
| Mean age, years | 69.6 | 59.2 | 59.4 | 55.6 | 59.6 | 55.8 | 59.6 | 55.4 | 64.4 |
| Male sex, % | 62.8 | 61.6 | 64.1 | 41 | 58.2 | 61.2 | 58.2 | 48.3 | 69.5 |
| eGFR, ml/min per 1.73 m² | 45.1 | >60 | >60 | Not reported | Not reported | >60 | Not reported | >60 | 77.8 |
| BMI, kg/m² | 30.2 | 28.6 | 31.7 | 30.1 | 31.8 | 29.8 | 31.8 | 32.0 | 32.6 |
| Diabetes duration, years | 15.9 | 6.2 | 8.7 | 7.4 | 8.6 | 9 | Not reported | 6.1 | 14.9 |
| HbA1c, % | 7.9 | 7.7 | 7.9 | Not reported | 8.01 | 8.6 | Not reported | 8.02 | 8.3 |
| Systolic blood pressure, mmHg | 137 | 128.4 | 135.3 | 127.2 | 133.8 | 129.3 | 133.8 | 129.2 | 134 |
| Diastolic blood pressure, mmHg | Not reported | 78.5 | 81 | 76.9 | 79.9 | 81.1 | Not reported | Not reported | 77 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Pancreatic function and diabetes · Diabetes Management and Research
Introduction and background
Diabetes is a leading cause of death worldwide, responsible for 6.7 million fatalities in 2021 and establishing itself as a major risk factor for the development of cardiovascular and kidney diseases. Particularly noteworthy is the widespread prevalence of type 2 diabetes mellitus (T2DM), accounting for over 90% of all cases globally [1-4]. Careful blood glucose control and targeted pharmacological intervention can slow the progression of macrovascular and microvascular complications associated with diabetes and lead to better management of this condition [5,6].
In this context, sodium-glucose cotransporter 2 (SGLT2) inhibitors have emerged as a promising therapeutic alternative by blocking sodium and glucose cotransportation, promoting glucosuria and natriuresis, particularly in hyperglycemic patients. In addition to their antidiabetic effects, they offer cardiovascular and renal benefits by increasing sodium delivery to the macula densa, leading to the constriction of afferent arterioles, which reduces glomerular hypertension and albuminuria, thereby slowing the progression of renal damage [7-10]. Bexagliflozin was the latest SGLT2 inhibitor approved by the Food and Drug Administration (FDA) in 2023. Studies have shown that it reduces glycated hemoglobin (HbA1c) similarly to other SGLT2 inhibitors in patients with T2DM. While sharing the core mechanism of action with other SGLT2 inhibitors, bexagliflozin exhibits distinct pharmacokinetic properties that set it apart. It has a longer half-life, allowing for once-daily dosing with sustained glycemic control. Additionally, unlike some other SGLT2 inhibitors, bexagliflozin demonstrates minimal off-target inhibition of SGLT1, which may contribute to a more favorable side-effect profile [11-19].
Despite the benefits in renal function and long-term albuminuria observed with other gliflozins, such as canagliflozin, dapagliflozin, and empagliflozin [20-23], the effects of bexagliflozin on renal outcomes remain uncertain. Therefore, this systematic review and meta-analysis aim to conduct a comprehensive analysis of clinical trials examining the effect of bexagliflozin on renal outcomes in adults with T2DM compared to placebo or other oral hypoglycemic agents (OHA).
Review
Methods
Search Strategy and Eligibility Criteria
This systematic review and meta-analysis follow the recommendations of the Cochrane Collaboration and are reported in accordance with the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Prior to literature screening, the protocol for this study was recorded prospectively in November 2023 in the International Prospective Register of Systematic Reviews (PROSPERO) database under the identification number CRD42023478336.
We searched the PubMed, Embase, and Cochrane Library electronic databases for studies published from inception to November 2023. To ensure a comprehensive search, we also hand-searched the ClinicalTrials.gov databases. The complete and detailed search strategy used was Bexagliflozin AND (RCT OR randomized OR randomised) AND ("type 2" OR diabetes OR diabetic OR DM OR T2DM).
Reviewers (M.G. and R.S.) independently evaluated titles, abstracts, and full-text articles. Any discrepancies were settled with the help of a third reviewer (T.M.). Studies were deemed eligible if they fulfilled the following inclusion criteria: randomized controlled trial (RCT); comparison of bexagliflozin to matched placebo or other OHA; patients diagnosed with T2DM; and reports on renal outcomes. Studies involving patients with type 1 DM, those lacking a control group, or those published in non-English languages were excluded.
Individual patient-level data were requested from the original authors and sponsors of the included studies. Because the required data were unavailable, a meta-analysis of summary data from published reports was conducted.
Statistical Analysis
Data were extracted independently from the included studies by three authors (R.S., M.G., T.M.) using a standardized structured form. Disagreements were resolved through discussion and, if necessary, by consulting with the senior author (C.E.P.F.).
We synthesized the data using a random-effects meta-analysis with a restricted maximum likelihood estimator. Binary outcomes were calculated using risk ratio (RR), while continuous endpoints were summarized with mean difference (MD). A 95% confidence interval (CI) with a p-value below 0.05 indicated statistical significance. Some heterogeneity due to limited data was anticipated, and analysis was performed by calculating the prediction interval (PI) associated with I-squared statistics, Cochran's Q test, p-value, and Tau. Additionally, subgroup analysis of placebo-controlled trials and meta-regression to evaluate the study-level impact of follow-up time were conducted. All statistical analyses were executed in R software version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria).
Quality Assessment
Two independent reviewers (T.M. and M.G.) assessed the risk of bias using Cochrane's Risk of Bias 2 (RoB 2) software. Each RCT was assigned a score (low, some concerns, or high) in each of the five domains: selection, performance, detection, attrition, and reporting biases. Disagreements were resolved by consensus. Authors (R.S. and T.M.) adhered to the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) handbook guidelines to evaluate the certainty level of the evidence, categorizing it from high to very low. The authors utilized the GRADEpro Guideline Development Tool and assessed the following outcomes: serum creatinine concentration and estimated glomerular filtration rate (eGFR).
Results
As shown in Figure 1, the first search yielded 47 papers. After the initial screening and removal of duplicates, an additional 36 articles were independently excluded by paired reviewers based on title and abstract evaluations. Subsequently, 11 articles underwent full evaluation. In this comprehensive review, two more were excluded due to their non-randomized design. Ultimately, we included nine RCTs, of which three were unpublished National Clinical Trials (NCT), involving 4,352 patients with T2DM [11-19].
PRISMA 2020 flow diagram.PRISMA 2020 flow diagram for new systematic reviews, which included searches of databases and registers only.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT: randomized controlled trial
Overview of Included Studies
The studies ranged from 2019 to 2023. The interventions across all studies included the administration of oral bexagliflozin, with dosages ranging from 5 mg to 20 mg daily. Therapeutic approaches exhibit variations: six trials used bexagliflozin as a monotherapy [11,12,14,15,18,19], while three studies incorporated metformin as a supplementary medication [13,16,17]. Additionally, five studies compared the intervention to a placebo [11,12,14,18,19], whereas four compared it to other oral antidiabetic drugs [13,15-17]. The follow-up duration ranged from 12 to 96 weeks. The baseline characteristics of all included studies are reported in Table 1.
Pooled Analysis of Outcomes
Creatinine levels and eGFR:Two RCTs involving 595 patients reported changes in serum creatinine levels among participants. In the pooled analysis, the treatment group showed no significant change in creatinine levels (MD: 0.05 mg/dL; 95% CI: -0.06 to 0.15; p = 0.35; PI: -0.18 to 0.12; Figure 2A). Two RCTs with 738 patients reported changes in eGFR among participants. The pooled analysis indicated no difference between groups (MD: -0.43 mL/min per 1.73 m²; 95% CI: -6.92 to 6.06; p = 0.896; PI: -4.94 to 4.08; Figure 2B).
(A) Change in serum creatinine from baseline. (B) Change in eGFR from baseline.References: (A) Allegretti et al. [11]; Halvorsen et al. [14]. (B) Allegretti et al. [11]; Halvorsen et al. [15].eGFR: estimated glomerular filtration rate; MD: mean difference; SD: standard deviation; CI: confidence interval
Systolic blood pressure (SBP): Nine RCTs encompassing 2,370 patients reported changes in SBP from baseline among participants. The pooled analysis revealed a statistically significant reduction in SBP in the treatment group (MD: -4.25 mmHg; 95% CI: -5.62 to -2.89; p < 0.01; PI: -7.99 to -0.52; Figure 3). There was no statistically significant difference in effect sizes between the subgroups (p = 0.66).
Change in systolic blood pressure from baseline.References: Halvorsen et al. [13]; Halvorsen et al. [15]; NCT02769481 [17]; Allegretti et al. [11]; Halvorsen et al. [12]; Halvorsen et al. [14]; Halvorsen et al. [16]; NCT02715258 [18]; NCT02558296 [19].OHA: oral hypoglycemic agents; MD: mean difference; SD: standard deviation; CI: confidence interval
Renal and urinary adverse events: Six RCTs including 2,018 patients reported renal and urinary adverse events as a single composite outcome among participants. In the pooled analysis, the bexagliflozin arm increased the risk of renal or urinary adverse events (RR: 2.09; 95% CI: 1.33 to 3.28; p < 0.01; PI: 1.1 to 3.9; Figure 4A). There was no statistically significant difference in effect sizes between the subgroups of placebo and other oral antidiabetics (p = 0.8). The linear impact of follow-up time on renal and urinary adverse events did not reach statistical significance in the meta-regression analysis, although a trend toward correlation can be observed through eye inspection (p = 0.3; Figure 4B).
(A) Renal and urinary adverse events reported as a single composite outcome. (B) Meta-regression analysis: impact of follow-up time on renal and urinary adverse events.References: Halvorsen et al. [13]; Halvorsen et al. [15]; NCT02769481 [17]; Halvorsen et al. [12]; Halvorsen et al. [14]; NCT02715258 [18].OHA: oral hypoglycemic agents; CI: confidence interval
Risk of bias assessment: Figure 5 outlines a comprehensive assessment of each RCT across all five domains of risk of bias. Among the included studies, one of the studies by Halvorsen et al. [16] and the NCT02558296 [19] were identified as being at high risk of bias due to missing outcome data, while the 2022 study by Halvorsen et al. [15] was categorized as having some concerns, primarily related to the randomization process.
Risk of bias assessment of the included studies.References: Allegretti et al. [11]; Halvorsen et al. [12]; Halvorsen et al. [13]; Halvorsen et al. [14]; Halvorsen et al. [15]; Halvorsen et al. [16]; NCT02769481 [17]; NCT02715258 [18]; NCT02558296 [19].
Certainty of evidence and GRADE assessment: The overall certainty of the evidence regarding the examined outcomes was downgraded in specific cases, depending on the severity of imprecision and bias effects. Appendix 1 includes a comprehensive GRADE assessment and a summary of findings.
Discussion
In this systematic review and meta-analysis of nine RCTs involving 4,352 patients, bexagliflozin was compared to either a placebo or OHA in individuals with T2DM. A statistically significant difference was observed between the two groups in SBP and renal and urinary adverse events as a single composite outcome; however, there was no significant difference in eGFR and serum creatinine levels.
Current guidelines recommend using SGLT2 inhibitors in patients with an eGFR above 30 mL/min/1.73 m² or higher, regardless of glucose levels. This recommendation is based on the observed benefits in composite cardiovascular and renal outcomes in large placebo-controlled trials [20,21,23,24] and a meta-analysis [25]. However, the results of the pooled analysis indicated no changes in creatinine and eGFR from baseline compared to the control group. It's important to note that only one study was conducted in the context of chronic renal failure [9], which reported a slight increase in serum creatinine concentration and a decrease in eGFR. These findings raise questions about whether bexagliflozin would have any positive renal effects, as benefits on renal function were not consistently observed across the various studies [9,15,16].
Trials examining SGLT2 inhibitors, such as canagliflozin, dapagliflozin, and empagliflozin, have shown consistent benefits in slowing the progressive decline of renal function and reducing albuminuria [20,22,23]. In contrast, bexagliflozin was linked to an increase in renal adverse events in individual studies and showed no benefits for renal function after initial administration. This difference may be related to the shorter follow-up duration and smaller cohort size compared to larger SGLT2 inhibitor trials.
The Effect of Sotagliflozin on Cardiovascular and Renal Events in Patients with Type 2 Diabetes and Moderate Renal Impairment Who Are at Cardiovascular Risk (SCORED) [26] and Effect of Sotagliflozin on Cardiovascular Events in Patients with Type 2 Diabetes Post Worsening Heart Failure (SOLOIST-WHF) [27] trials did not demonstrate differences in renal outcomes with sotagliflozin compared to placebo. However, these trials were prematurely halted due to a lack of funding and were limited to a mean duration of nine and 16 months. Addressing the significance of extended follow-up, the Kidney Outcomes Associated With Use of SGLT2 Inhibitors in Real-World Clinical Practice (CVD-REAL III) [28], a propensity-matching observational cohort of 35,561 patients, highlighted the renal benefits of gliflozins in diabetic patients, which became evident only after 12 months of follow-up. Similarly, the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) [21] and Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) [22] studies noted a lower risk of progression of chronic kidney disease with a beneficial effect on eGFR, compared to placebo, only after 12 months of follow-up. The Empagliflozin Outcome Trial in Patients with Chronic Heart Failure and a Reduced Ejection Fraction (EMPEROR-Reduced) [29], which compared empagliflozin to placebo, observed improved eGFR levels after 100 weeks of randomization. In the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF)/Renal [30], the benefit to renal function in diabetic patients became apparent only after 720 days of randomization. The Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial (VERTIS-CV) [31] noted a crossover between ertugliflozin and the placebo only after 36-48 weeks of randomization. Remarkably, the Dapagliflozin Effect on Cardiovascular Events-Thrombolysis in Myocardial Infarction 58 (DECLARE-TIMI 58) [32], which compared dapagliflozin to placebo, observed a crossover in renal composite outcomes after 540 days of randomization. Likewise, in a pooled analysis on SGLT2 inhibitors' impact on renal outcomes at the longest follow-ups, the risk of progressive kidney disease was lower in the treatment group regardless of baseline eGFR values [25]. Therefore, the potential detrimental and neutral effects of bexagliflozin on renal outcomes and renal function, respectively, raise questions about its impact during prolonged follow-up periods.
Regular screening for urine albumin-to-creatinine ratio (UACR) is recommended for individuals with T2DM to detect kidney disease in its early stages [33], as its elevation is often an early sign of diabetic nephropathy. Other SGLT2 inhibitors have demonstrated a reduction in UACR levels that is associated with slowing the progression of kidney disease. For instance, the DECLARE-TIMI 58 trial [32] showed an improved UACR from baseline across all eGFR categories when dapagliflozin was compared to placebo over a four-year follow-up period. Additionally, a post hoc analysis of the CREDENCE trial [21] indicated an early 30% reduction in albuminuria with canagliflozin during a 26-week follow-up, which correlated with fewer kidney outcomes. However, it is noteworthy that the studies included in this meta-analysis did not provide explicit information regarding changes in UACR levels. The lack of consistent reporting of UACR outcomes across these studies presents a significant data gap in our assessment of the impact of these interventions on renal health. Several factors may contribute to the development of elevated UACR in T2DM, including prolonged high blood glucose levels and hypertension. Further studies on the effect of bexagliflozin on UACR levels are warranted.
Among the included trials, bexagliflozin was significantly associated with a reduction in HbA1c levels, reflecting the effects on glucose parameters similar to other SGLT2 inhibitors [34]. However, the underlying mechanisms of the renal outcomes related to SGLT2 inhibitors are not fully understood. Increasing evidence suggests that hemodynamic factors, such as reduced blood pressure, play a key role, without a clear link between glucose levels and kidney events [24]. In our pooled analysis, bexagliflozin was associated with a four-point mean reduction in SBP. Although there was no data to pool diastolic blood pressure (DBP) values, individual studies [9,13,14] reported a nonsignificant difference between groups. Similarly, an updated meta-analysis [34] indicated a notable reduction in SBP levels, which was not linked to worsening renal function or increased renal adverse events.
The strengths of our study include the large sample size derived exclusively from RCTs and the focus on a recently FDA-approved drug, providing valuable insights in an area where evidence from cohort studies is currently limited. However, limitations should be noted. First, the short follow-up duration in the included studies limits the ability to fully assess the long-term effects of bexagliflozin on renal function and related outcomes. This temporal constraint likely precludes the observation of meaningful changes in key renal endpoints, such as sustained declines in eGFR, initiation of dialysis, or progression to kidney failure. Second, limited availability of outcome data prevented a more granular stratification of results, particularly by baseline eGFR levels. Stratified analyses could have provided deeper insights into the efficacy and safety of bexagliflozin in specific subgroups, such as patients with varying degrees of chronic kidney disease, or using different anti-hypertensive drugs. Third, the meta-analysis highlights a significant increase in the risk of a composite outcome encompassing renal and urinary adverse events. However, this approach, adopted from the included studies, raises interpretative challenges, as it combines fundamentally distinct clinical entities. Grouping renal and urinary outcomes together may obscure the specific risks and benefits associated with each, complicating clinical decision-making. Fourth, while incorporating registered trials and only English published trials can enhance the comprehensiveness of the evidence base, it also introduces the risk of selective reporting, especially when results from these studies remain unpublished or are only partially disclosed. Consequently, the presence of publication bias should be acknowledged as a limitation that may affect the validity of the conclusions. Finally, the inability to perform an individual patient data (IPD) analysis due to the unavailability of detailed data from study authors or sponsors represents a further limitation. Access to IPD could have allowed for more precise adjustments, subgroup analyses, and exploration of additional confounding factors, thereby enhancing the robustness of our findings.
These limitations underscore the need for future research with longer follow-up durations, standardized outcome definitions, and access to individual patient-level data to provide a more comprehensive understanding of bexagliflozin's renal safety and efficacy.
Conclusions
This investigation has not identified a beneficial effect of bexagliflozin on kidney disease progression, as observed with other SGLT2 inhibitors like empagliflozin, canagliflozin, and dapagliflozin. Future studies should prioritize long-term evaluations and include a broader range of patient populations, reflecting the diverse real-world settings where these medications are used. Additionally, comparative trials directly assessing bexagliflozin against established SGLT2 inhibitor agents will provide critical insights into its efficacy and safety, particularly in terms of renal outcomes. Such research will be essential for clarifying its role in clinical practice and determining whether it can match the benefits demonstrated by its counterparts. Ultimately, the use of bexagliflozin should be tailored to the patient's clinical profile and risk factors, guided by the evolving evidence in the field of SGLT2 inhibitors and considering each agent's potential advantages and limitations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Classification and diagnosis of diabetes: standards of medical care in diabetes-2018 Diabetes Care 02741201810.2337/dc 18-S 00229222373 · doi ↗ · pubmed ↗
- 2IDF Diabetes Atlas 11 2023 2025 https://diabetesatlas.org/
- 3Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies Lancet Sarwar N Gao P Seshasai SR 2215222237520102060996710.1016/S 0140-6736(10)60484-9PMC 2904878 · doi ↗ · pubmed ↗
- 4The heart failure burden of type 2 diabetes mellitus-a review of pathophysiology and interventions Heart Fail Rev Ofstad AP Atar D Gullestad L Langslet G Johansen OE 3033232320182951623010.1007/s 10741-018-9685-0PMC 5937871 · doi ↗ · pubmed ↗
- 5The effect of RAAS blockade on the progression of diabetic nephropathy Nat Rev Nephrol Roscioni SS Heerspink HJ de Zeeuw D 77871020142429662310.1038/nrneph.2013.251 · doi ↗ · pubmed ↗
- 6Diabetes as a cardiovascular risk factor: an overview of global trends of macro and micro vascular complications Eur J Prev Cardiol Dal Canto E Ceriello A Rydén L 25322620193172256210.1177/2047487319878371 · doi ↗ · pubmed ↗
- 7EGT 1442, a potent and selective SGLT 2 inhibitor, attenuates blood glucose and Hb A 1c levels in db/db mice and prolongs the survival of stroke-prone rats Pharmacol Res Zhang W Welihinda A Mechanic J 2842936320112121531410.1016/j.phrs.2011.01.001 · doi ↗ · pubmed ↗
- 8SGLT 2 inhibitors: nephroprotective efficacy and side effects Medicina (Kaunas) Garofalo C Borrelli S Liberti ME 2685520193121263810.3390/medicina 55060268 PMC 6630922 · doi ↗ · pubmed ↗