The significance of serum sST2 and cfDNA in children with severe pneumonia complicated by myocardial damage
Tingting Zhao, Ye Liu, Haoran Jia, Dexing Wang, Meng Du, Weiwei Wang

TL;DR
This study explores how serum sST2 and cfDNA levels can predict heart function in children with severe pneumonia and heart damage.
Contribution
The study identifies sST2 and cfDNA as potential biomarkers for predicting cardiac outcomes in children with severe pneumonia and myocardial damage.
Findings
Elevated sST2 and cfDNA levels correlate with cardiac function parameters like LVEDd and LVESd.
Higher biomarker levels are linked to lower likelihood of improvement and higher readmission rates.
Multivariate analysis confirms the association between biomarkers and cardiac outcomes.
Abstract
The paper aimed to explore the significance of serum soluble ST2 (sST2) and circulating cell-free DNA (cfDNA) in predicting cardiac functions in children with severe pneumonia complicated by myocardial damage. This case series study evaluated the serum sST2 and cfDNA levels of 60 children with severe pneumonia complicated by myocardial damage, assessing clinical data, biomarker levels, and cardiac function. We analyzed data from a cohort of 60 patients with a mean age of 4.47±1.88 years and a male: female ratio of 28:32. At baseline, patients had elevated levels of serum biomarkers, including sST2 and cfDNA, which were associated with cardiac function parameters and clinical outcomes. After 6 months, patients showed significant correlations between sST2, cfDNA, and cardiac function parameters, including left ventricular end-diastolic diameter (LVEDd), left ventricular end-systolic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
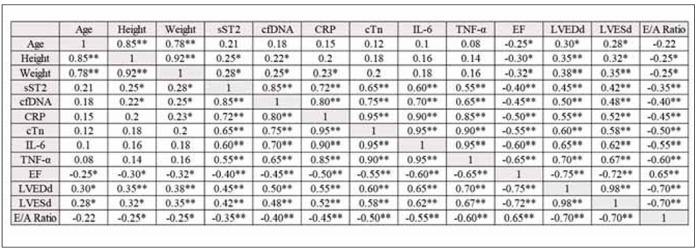 Figure 1
Figure 1| Category | Unit | Baseline | 6 month follow up |
|---|---|---|---|
| Gender | Male:<br>Female | 1.188889 | |
| Age | years | 4.47±1.88 | |
| Height | cm | 118.49±3.52 | |
| Weight | kg | 24.46±2.69 | |
| Family History of Heart Disease | % | 3 (5.00%) | |
| Past Medical History of Heart and Lung | % | 1 (1.66%) | |
| sST2 | ng/mL | 30.46±3.21 | 28.71±2.65 |
| cfDNA | ng/mL | 11.45±1.37 | 10.33±1.20 |
| CRP | mg/L | 21.45±1.63 | 18.61±1.44 |
| cTn | ng/mL | 0.06±0.01 | 0.05±0.02 |
| IL-6 | pg/mL | 26.38±2.59 | 23.28±2.16 |
| TNF-α | pg/mL | 28.57±3.11 | 24.31±2.55 |
| EF | % | 55.49±3.51 | |
| LVEDd | mm | 40.63±2.88 | |
| LVESd | mm | 29.56±2.35 | |
| E/A Ratio | ratio | 1.27±0.10 | |
| Improvement Rate of Cardiac Function | % | 0.5 | |
| Remission Rate of Cardiac Functions | % | 0.45 | |
| 6-month Readmission Rate | % | 0.2833 |
| LVEDd (mm) | LVESd (mm) | E/A Ratio | Improvement Rate | 6-month Readmission | |
|---|---|---|---|---|---|
| β (95% CI) | β (95% CI) | β (95% CI) | Odds Ratio (95% CI) | Odds Ratio (95% CI) | |
| Serum sST2 (ng/mL) | 0.43 (0.21–0.65)* | 0.31 (0.12–0.50)* | 0.21 (0.08–0.34)* | 1.23 (1.05–1.44)* | 1.50 (1.20–1.88)* |
| cfDNA (ng/mL) | 0.35 (0.15–0.55)* | 0.26 (0.09–0.43)* | 0.18 (0.05–0.31)* | 1.18 (1.02–1.36)* | 1.38 (1.12–1.70) |
- —Baoding Hospital of Beijing Children's Hospital Affiliated to Capital Medical University, supports the research: The value of serum sST2 and cfDNA in predicting myocardial damage in children with seve
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIL-33, ST2, and ILC Pathways · Inflammasome and immune disorders · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
Severe pneumonia is a common serious respiratory disease in paediatrics, and one of its complications is myocardial damage, which not only increases the mortality of children but also affects their long-term health [1] [2]. Therefore, effective prevention and treatment of severe pneumonia complicated with myocardial damage is of great significance in advancing children’s therapeutic effect and mass of life [3] [4]. It also causes a series of diseases like arrhythmia, increasing the risk of heart failure and sudden death in children [5]. Therefore, monitoring and preventing cardiac function decrease in children with severe pneumonia is of great clinical value. Serum sST2 and cfDNA, as emerging biomarkers in recent years, have shown important potential applications in the diagnosis and prognosis evaluation of heart diseases [6]. SST2 is a marker related to cardiac stress and inflammatory reaction, and the increase in its level is closely related to the increased risk of myocardial injury and heart failure [7]. CfDNA is a free DNA fragment released into the blood by apoptosis or necrosis, and its level in myocardial injury is also of great significance [8] [9]. Severe pneumonia complicated with myocardial damage is a serious clinical situation, and when it happens, the prognosis of patients is often more unfavourable [10] [11] [12]. In the context of severe pneumonia, the atrium may be damaged by an inflammatory reaction, which can be detected by changes in the electrocardiogram, increased cardiac biomarkers, or changes in cardiac imaging technology (such as echocardiography) [13] [14]. Severe pneumonia affects the lungs and causes a systemic inflammatory reaction, which affects the heart function and then leads to myocardial damage [15]. In this case, the level changes of sST2 and cfDNA can provide important information for the clinic. SST2 is a biomarker closely related to cardiac stress and inflammation, which rises during myocardial stress and can reflect myocardial cells’ stress state and degree of inflammation. The increase in sST2 level is closely related to the prognosis of heart diseases, so monitoring sST2 level in children with severe pneumonia complicated with myocardial damage can help evaluate cardiac involvement’s degree and prognosis [16] [17]. The combined monitoring of these two markers provides a new perspective and method for assessing myocardial damage and cardiac functions. Against this background, this study aimed to explore the influence of serum sST2 and cfDNA on predicting cardiac functions in children with severe pneumonia complicated with myocardial damage.
Materials and methods
This was a case series study from April 2021 to December 2023 in which 60 children with severe pneumonia complicated with myocardial damage were recruited as the research object before being included in the study. The patient or their guardian informed consent and signed the study consent form.
Entry criteria were as follows: participants are between 1 and 15 years old; a diagnosis of severe pneumonia confirmed by a doctor; cardiac ultrasound or other related examination confirmed the existence of myocardial damage. We obtained the written informed consent of parents or legal guardians. There were no other major acute or chronic medical conditions except severe pneumonia and myocardial damage. Parents or guardians agreed and could make children participate in long-term follow-up.
Exclusion criteria were: known chronic heart disease or myocarditis diagnosed before; at the same time, there were other serious systemic diseases, such as advanced nephropathy, severe liver disease or malignant tumour; recently (within 3 months) received treatment from other clinical trials; unable to obtain reliable blood samples or imaging data.
Our hospital’s Ethics Committee approved this study. The patient or their guardian was informed of the research content and was willing to cooperate with the doctor.
Outcomes and measures
ELISA was used to test the serum sST2 and cfDNA levels and the markers of troponin, IL-6 and TNF-α. These data helped to evaluate the inflammatory state and its changes after interventions. Cardiac function parameters such as LVEDd, LVESd and E/A ratio were collected by echocardiography to assess patients’ cardiac function changes after treatments. In addition, this study also compared the improvement rate of cardiac function, the remission rate of cardiac functions and the hospitalization rate within 6 months.
Statistical analysis
In this study, all the data were processed by SPSS20.0 statistical analysis software (IBM); the measurement data were measured by »mean ± standard deviation« (± s), one-way analysis of variance or repeated measures, LSD-t-test, the count data were calculated by percentage (%), and χ^2^; P<0.05 represents statistical significance.
Results
Our cohort of patients had male:female ratio of 28:32, the mean age was 4.47±1.88 years, the mean height was 118.49±3.52 cm, and the average weight was 24.46±2.69 kg, among which 3 patients had a family history of heart disease, and 1 case had previous heart and lung history (Table 1). Figure 1
*Correlation matrix of study variables (r values of Pearson correlation is shown).<br>**: p < 0.01, : p < 0.05
The correlation matrix shows several significant relationships between the variables. Age, Height, and Weight are highly correlated with each other (r>0.85), indicating that they tend to increase together. sST2, cfDNA, CRP, cTn, IL-6, and TNF-α are highly correlated (r>0.60), suggesting that they tend to increase together. These variables are all related to inflammation and cardiac function. EF is negatively correlated with LVEDd, LVESd, and E/A Ratio (r<-0.65), indicating that these variables tend to decrease as EF increases. Table 2
**Table 2: Multiple Linear Regression Analysis of Serum sST2 and cfDNA on Cardiac Function Parameters at 6-Month Follow-up and Logistic Regression of Serum sST2 and cfDNA on Improvement and Readmission Rates.Significant at p<0.05
We found significant associations between serum biomarkers, echocardiographic parameters, and clinical outcomes. For every 1 ng/mL increase in serum soluble ST2 (sST2), there were significant increases in left ventricular end-diastolic diameter (LVEDd, β=0.43, 95% CI: 0.21–0.65, p<0.05), left ventricular end-systolic diameter (LVESd, β=0.31, 95% CI: 0.12–0.50, p<0.05), and E/A ratio (β=0.21, 95% CI: 0.08–0.34, p<0.05). Similarly, every 1 ng/mL increase in circulating cell-free DNA (cfDNA) was associated with significant increases in LVEDd (β=0.35, 95% CI: 0.15–0.55, p<0.05), LVESd (β=0.26, 95% CI: 0.09–0.43, p<0.05), and E/A ratio (β=0.18, 95% CI: 0.05–0.31, p<0.05). Furthermore, higher levels of sST2 and cfDNA were associated with a lower likelihood of improvement (sST2: odds ratio = 1.23, 95% CI: 1.05-1.44, p<0.05; cfDNA: odds ratio = 1.18, 95% CI: 1.02–1.36, p<0.05) and a higher likelihood of 6-month readmission (sST2: odds ratio = 1.50, 95% CI: 1.20–1.88, p<0.05; cfDNA: odds ratio = 1.38, 95% CI: 1.12–1.70, p<0.05).
Discussion
Our results showed that higher levels of sST2 and cfDNA were associated with increased left ventricular end-diastolic diameter (LVEDd), left ventricular end-systolic diameter (LVESd), and E/A ratio, as well as a lower likelihood of improvement and a higher likelihood of 6-month readmission.
Our results align with previous studies demonstrating the prognostic value of sST2 in pediatric cardiac diseases. For instance, elevated sST2 levels have been associated with an increased risk of adverse events in pediatric dilated cardiomyopathy (PDCM) [17] Similarly, sST2 is a useful biomarker for predicting cardiac outcomes in adult patients with complex congenital heart disease [17]. Our study extends these findings by demonstrating the potential of sST2 as a biomarker in children with severe pneumonia complicated by myocardial damage.
The analytical performances of sST2 assays have been previously evaluated, and reference intervals have been established for children and adolescents [18]. Our study highlights the clinical application of sST2 as a biomarker, demonstrating its potential in predicting cardiac function and outcomes in pediatric patients.
The mechanisms underlying the association between sST2 and cardiac outcomes are not fully understood. However, it is thought that sST2 may reflect the degree of cardiac stress and inflammation, which are common in pediatric cardiac diseases [19]. Further studies are needed to fully elucidate the mechanisms underlying the association between sST2 and cardiac outcomes.
The use of cfDNA as a biomarker in pediatric cardiac diseases is a growing area of research. A recent Tanem et al. [20] study demonstrated that nuclear cell-free DNA (ncfDNA) kinetics can predict adverse events after pediatric cardiothoracic surgery. The study found elevated preoperative ncfDNA was strongly associated with postoperative arrest and extracorporeal membrane oxygenation. Our study builds on this research by investigating the role of cfDNA in predicting cardiac functions in children with severe pneumonia complicated by myocardial damage. Another study by Richmond et al. [21] validated donor fraction cell-free DNA as a noninvasive test to assess the risk of acute cellular rejection and antibody-mediated rejection after heart transplantation in pediatric and adult recipients. The study found that donor fraction cell-free DNA at a threshold of 0.14% had excellent negative predictive value for detecting rejection. While our study focused on the use of cfDNA in predicting cardiac functions, these studies collectively highlight the potential of cfDNA as a biomarker in pediatric cardiac diseases.
Dodatak
Funding
Baoding Hospital of Beijing Children’s Hospital Affiliated to Capital Medical University, supports the research: The value of serum sST2 and cfDNA in predicting myocardial damage in children with severe pneumonia (No. 2341ZF390).
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S 124suppl_231Apr 1; 54201210.1093/cid/cir 1067 Wonodi C B Deloria-Knoll M Feikin D R Deluca A N Driscoll A J Moïsi J C Johnson H L Murdoch D R O'Brien K L Levine O S Scott J A Clinical Infectious Diseases Evaluation of risk factors for severe pneumonia in children: The pneumonia etiology research for child health study 22403226 PMC 3297552 · doi ↗ · pubmed ↗
- 210361039 Nov; 58202110.1007/s 13312-021-2369-1 Goyal J P Kumar P Mukherjee A Das R R Bhat J I Ratageri V Vyas B Lodha R Charoo B A Khera D Singhal D Indian Pediatrics Risk factors for the development of pneumonia and severe pneumonia in children 34837363 · doi ↗ · pubmed ↗
- 317165172341201310.1177/0300060513497559 Li C M Gu L Yin S J Yang R Xie Y Guo X Z Fu Y X Cheng D Journal of International Medical Research Age-specific mycoplasma pneumoniae pneumonia-associated myocardial damage in children 24026772 · doi ↗ · pubmed ↗
- 48956905 Mar 15; 205201210.1093/infdis/jir 861 Paddock C D Liu L Denison A M Bartlett J H Holman R C De Leon-Carnes M Emery S L Drew C P Shieh W J Uyeki T M Zaki S R Journal of Infectious Diseases Myocardial injury and bacterial pneumonia contribute to the pathogenesis of fatal influenza B virus infection 22291193 · doi ↗ · pubmed ↗
- 57516774 Mar 17; 132202310.1161/circresaha.122.321636 Stotts C Corrales-Medina V F Rayner K J Circulation Research Pneumonia-induced inflammation, resolution and cardiovascular disease: Causes, consequences and clinical opportunities 36927184 · doi ↗ · pubmed ↗
- 63064309 Oct; 40200510.1002/ppul.20233 Haviv M Haver E Lichtstein D Hurvitz H Klar A Pediatric Pulmonology Atrial natriuretic peptide in children with pneumonia 15830390 · doi ↗ · pubmed ↗
- 7721423 Nov 21; 12202310.3390/jcm 12237214 Crisci G Bobbio E Gentile P Bromage D I Bollano E Ferone E Israr M Z Heaney L M Polte C L CannatàA Salzano A Journal of Clinical Medicine Biomarkers in acute myocarditis and chronic inflammatory cardiomyopathy: An updated review of the literature 38068265 PMC 10706911 · doi ↗ · pubmed ↗
- 834024 Feb 8; 24202310.3390/ijms 24043402 Melamud M M Buneva V N Ermakov E A International Journal of Molecular Sciences Circulating cell-free DNA Levels in psychiatric diseases: A systematic review and meta-analysis 36834811 PMC 9963116 · doi ↗ · pubmed ↗