Chilblains With Tumid Lupus Features in a Patient With Sjögren’s Syndrome: A Case Report
Thanda Aung, Mia Celestin

TL;DR
A young woman with Sjögren's syndrome developed chilblain-like skin lesions resembling tumid lupus and improved with B-cell-targeted therapy.
Contribution
Demonstrates the potential efficacy of belimumab in treating refractory cutaneous manifestations in autoimmune overlap syndromes.
Findings
The patient showed significant improvement with belimumab after conventional therapies failed.
Skin biopsy revealed interface dermatitis and lymphoplasmacytic infiltration consistent with tumid lupus.
The case highlights the overlap between Sjögren's syndrome and lupus spectrum disorders.
Abstract
Sjögren's syndrome is an autoimmune disorder characterized by lymphocytic infiltration of exocrine glands, primarily affecting the lacrimal and salivary glands, resulting in dry eyes and mouth. We report a case of a 22-year-old female with Sjögren's syndrome (diagnosed at age 14), who developed chilblain-like lesions with histopathological features of tumid lupus. The patient presented with low-grade fever and painful erythematous papules on the fingers, toes, ears, face, and trunk. Serological workup revealed multiple autoantibodies (anti-SSA (Sjögren's-syndrome-related antigen A), anti-SSB (Sjögren's-syndrome-related antigen B), anti-centromere, anti-U1RNP (anti-U1 ribonucleoprotein), ANA (antinuclear antibody), and rheumatoid factor). Skin biopsy demonstrated interface dermatitis with lymphoplasmacytic infiltration and increased dermal mucin. After an inadequate response to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3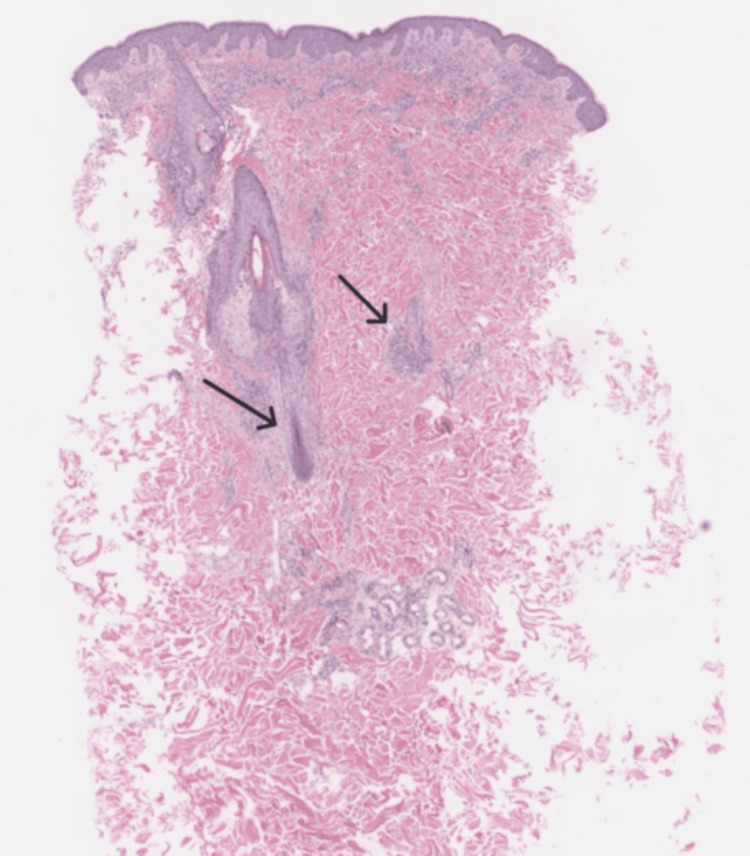 Figure 4
Figure 4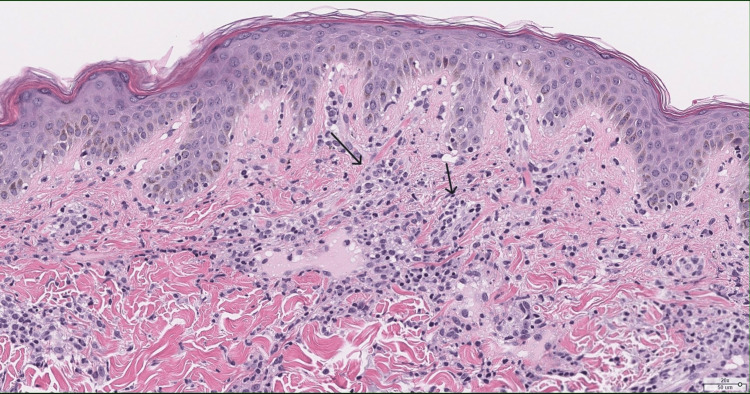 Figure 5
Figure 5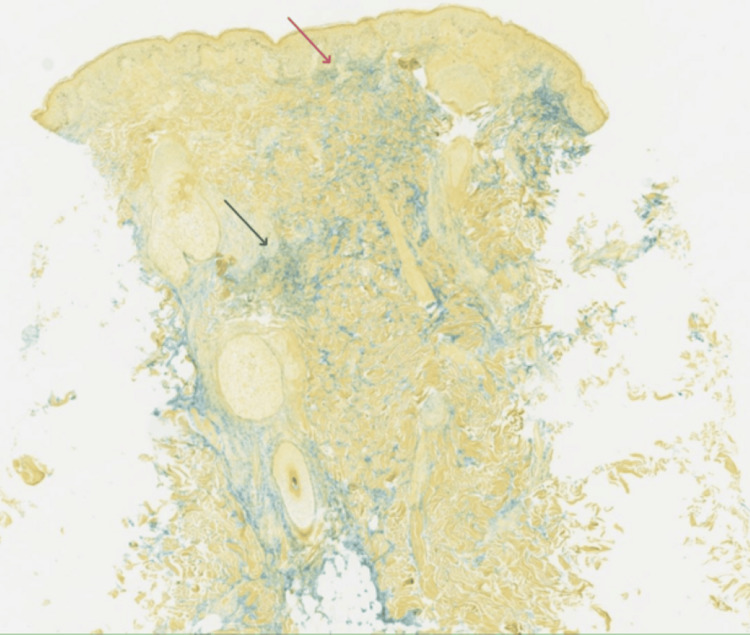 Figure 6
Figure 6| Pertinent Lab Data | Patient's Lab Values | Reference Range |
| ANA Ab Titer | 1:1280 | <1:40 |
| SSA (U) | >8.0 | <1.0 |
| SSB (U) | >8.0 | <1.0 |
| Rheumatoid Factor (IU/mL) | 16 | <14 |
| Centromere B Antibody | 6.5 | <1.0 |
| ESR (mm/hr) | 40 | <=25 |
| U1 SNRNP IgG (U) | 21 | 0-19 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatological and COVID-19 studies · Salivary Gland Disorders and Functions · Skin Diseases and Diabetes
Introduction
Sjögren's syndrome is a chronic autoimmune inflammatory disorder characterized by lymphocytic infiltration of exocrine glands, primarily affecting salivary and lacrimal glands [1]. While glandular manifestations are the hallmark of the disease, extra-glandular involvement, including cutaneous manifestations, occurs in approximately 55% of patients [2,3]. Various dermatological presentations have been reported in Sjögren's syndrome, including xerosis, annular erythema, vasculitis, and less commonly, chilblains [4,5].
Chilblains (perniosis) present as inflammatory, erythematous to violaceous papules or nodules, typically affecting acral sites in response to cold exposure. Its pathophysiology involves abnormal vascular responses to cold, resulting in vasospasm followed by reactive vasodilation, with subsequent inflammation [6,7]. While primary chilblains often occur in otherwise healthy individuals, secondary chilblains can be associated with various autoimmune conditions, particularly lupus erythematosus (chilblain lupus) [7,8].
Tumid lupus erythematosus represents a distinct subtype of cutaneous lupus characterized by photosensitive, edematous, indurated plaques without epidermal involvement. Histopathologically, it features prominent dermal mucin deposition with perivascular and periadnexal lymphocytic infiltration [8,9]. The overlap between tumid lupus and chilblains in patients with Sjögren's syndrome has been rarely reported and presents diagnostic and therapeutic challenges.
We present a case of chilblain-like lesions with histopathological features of tumid lupus in a young woman with Sjögren's syndrome, who demonstrated significant improvement with belimumab therapy after inadequate response to conventional treatments.
Case presentation
A 22-year-old female with Sjögren's syndrome, diagnosed at age 14, presented with low-grade fever and painful erythematous papules affecting the fingers, toes, and ears, as well as similar lesions on the face and trunk. Her medical history was significant for Raynaud's phenomenon. Physical examination revealed well-demarcated, erythematous to violaceous papules and plaques on the distal aspects of the fingers and toes, with similar lesions on the helices of both ears (Figures 1-3). Additional examination showed scattered erythematous, edematous plaques on the malar region of the face, and the upper back and chest. The lesions were tender to palpation, and the acral lesions became more prominent with cold exposure.
Lesion on the right ear before treatment with belimumab (left side), vs. resolution of lesions after treatment with belimumab (right side)
Lesion on the left cheek before treatment with belimumab (left side), vs. resolution of lesions after treatment with belimumab (right side)
Lesion on the right hand before treatment with belimumab (left side), vs. resolution of lesions after treatment with belimumab (right side)
Laboratory investigations revealed a normal complete blood count, as well as normal renal and liver function tests. Serological studies showed positive anti-SSA (Sjögren's-syndrome-related antigen A) (Ro) and anti-SSB (Sjögren's-syndrome-related antigen B) (La) antibodies, consistent with her established diagnosis of Sjögren's syndrome. Additional serologies revealed positive anti-centromere antibodies, anti-U1 SNRNP (small nuclear ribonucleoprotein) antibodies, positive antinuclear antibody (ANA) (1:1280, homogeneous pattern), and positive rheumatoid factor (16 IU/mL). Anti-cyclic citrullinated peptide (anti-CCP) antibodies, antineutrophil cytoplasmic antibody (ANCA), angiotensin-converting enzyme (ACE), and immunoglobulin G4 (IgG4) levels were negative or within normal limits (Table 1).
A punch biopsy from a representative lesion on the right paraspinal back demonstrated interface dermatitis with superficial and deep dermal perivascular and perifollicular lymphoplasmacytic inflammation (Figures 4-5). Special stains (alcian blue and colloidal iron) revealed increased dermal mucin deposition (Figure 6). No evidence of malignancy was identified. The pathologist commented that the findings supported a diagnosis of connective tissue disease, most consistent with tumid lupus.
A 2x low-power hematoxylin & eosin staining - interface dermatitis, with arrows showing deep perivascular and periadnexal lymphoplasmacytic inflammation
A 20x power hematoxylin & eosin staining - interface dermatitis, with arrows showing superficial perivascular and periadnexal lymphoplasmacytic inflammation
A 3x power colloidal iron special stain highlighting superficial (red arrow) and deep dermal (black arrow) mucin, alcian blue, and colloidal iron stain
Initial management included hydroxychloroquine (Plaquenil) 400 mg daily, methotrexate 15 mg weekly, prednisone 20 mg daily (tapered over eight weeks), topical tacrolimus 0.1% ointment twice daily, and intralesional triamcinolone (Kenalog) injections (5 mg/mL) for persistent lesions. Despite this multimodal approach for two months, the patient continued to develop new lesions, with only partial improvement in existing lesions.
Given the inadequate response to conventional therapy, belimumab was initiated at a dose of 10 mg/kg intravenously every two weeks for the first three doses, followed by monthly infusions. Significant improvement was observed after the third infusion, with resolution of fever, marked reduction in the number and intensity of skin lesions, and decreased pain. After six months of belimumab therapy, the patient maintained substantial clinical improvement, with only occasional mild flares associated with cold exposure.
Discussion
This case presents several interesting diagnostic and therapeutic considerations. The clinical presentation of chilblain-like lesions in a patient with established Sjögren's syndrome, together with histopathological features of tumid lupus, illustrates the complex overlap that can occur within the spectrum of autoimmune rheumatic diseases [6,10].
The distribution of lesions in our patient is noteworthy, with involvement of both acral sites (characteristic of chilblains) and photo-distributed areas on the face and trunk (typical of tumid lupus). This mixed distribution pattern further supports the concept of an overlap syndrome, with features of both conditions [4,8].
The coexistence of multiple autoantibodies in our patient is also significant. While anti-SSA and anti-SSB antibodies are characteristic of Sjögren's syndrome, the presence of anti-centromere antibodies (typically associated with limited systemic sclerosis) and anti-U1RNP (anti-U1 ribonucleoprotein) antibodies (associated with mixed connective tissue disease) suggests an autoimmune overlap syndrome. This serological profile has been reported to correlate with a higher risk of extra-glandular manifestations in Sjögren's syndrome patients, including cutaneous involvement [10-12].
Distinguishing chilblains from tumid lupus can be challenging, as both conditions may demonstrate lymphocytic infiltration and dermal mucin deposition. However, the prominent interface dermatitis and significant mucin accumulation in our patient’s biopsy are more characteristic of tumid lupus [8,13]. The literature suggests that chilblains associated with autoimmune conditions often show histological features that overlap with lupus erythematosus, supporting the concept of a spectrum rather than distinct entities [7,8].
The therapeutic approach to chilblains in the setting of autoimmune disease typically includes conservative measures, calcium channel blockers, antimalarials, and immunosuppressants. Tumid lupus generally responds well to antimalarials and photoprotection [8,9]. However, the patient demonstrated only a partial response to conventional therapy, necessitating escalation to biologic therapy.
Belimumab, a monoclonal antibody targeting B-lymphocyte stimulator (BLyS), is FDA-approved for systemic lupus erythematosus and has shown efficacy in Sjögren's syndrome in small studies [14,15]. The significant clinical improvement observed with belimumab in our patient suggests that B-cell-targeted therapy may be particularly effective in managing cutaneous manifestations at the intersection of Sjögren's syndrome and lupus. Recent literature supports the efficacy of belimumab in various cutaneous lupus subtypes, though data specifically for tumid lupus or chilblains in Sjögren's syndrome remain limited [15].
This case adds to the growing body of evidence suggesting that targeting the B-cell pathway may be beneficial in autoimmune overlap syndromes with prominent cutaneous manifestations. It also highlights the importance of recognizing the potential overlap between chilblains and tumid lupus in patients with underlying autoimmune disorders.
Conclusions
This case explores a rare instance of chilblain-like lesions with histopathological features of tumid lupus in a young woman with Sjögren's syndrome and serological evidence of autoimmune overlap. It illustrates the diagnostic challenges in characterizing cutaneous manifestations in autoimmune disorders and demonstrates the potential efficacy of belimumab in managing refractory skin lesions. The favorable response to B-cell-targeted therapy suggests that dysregulated B-cell pathways play a significant role in the pathogenesis of these overlapping conditions. Further research is warranted to better understand the relationship between Sjögren's syndrome, chilblains, and tumid lupus, and to establish optimal therapeutic strategies for patients with similar presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sjögren's syndrome Annu Rev Pathol Mavragani CP Moutsopoulos HM 273285920142405062310.1146/annurev-pathol-012513-104728 · doi ↗ · pubmed ↗
- 2Primary Sjogren syndrome BMJ Ramos-Casals M Brito-Zerón P Sisó-Almirall A Bosch X 0344201210.1136/bmj.e 382122700787 · doi ↗ · pubmed ↗
- 3The diagnosis and treatment of Sjögren's syndrome Dtsch Arztebl Int Stefanski AL Tomiak C Pleyer U Dietrich T Burmester GR Dörner T 35436111420172861065510.3238/arztebl.2017.0354 PMC 5471601 · doi ↗ · pubmed ↗
- 4Dermatologic manifestations of Sjögren syndrome J Cutan Med Surg Kittridge A Routhouska SB Korman NJ 8141520112129165010.2310/7750.2010.09033 · doi ↗ · pubmed ↗
- 5Cutaneous findings in patients with primary Sjogren's syndrome Clin Rheumatol Soy M Piskin S 135013522620071691535810.1007/s 10067-006-0374-3 · doi ↗ · pubmed ↗
- 6Characterization of systemic disease in primary Sjögren's syndrome: EULAR-SS Task Force recommendations for articular, cutaneous, pulmonary and renal involvements Rheumatology (Oxford) Ramos-Casals M Brito-Zerón P Seror R 223022385420152623134510.1093/rheumatology/kev 200PMC 6281074 · doi ↗ · pubmed ↗
- 7Clinical characteristics, etiologic associations, laboratory findings, treatment, and proposal of diagnostic criteria of pernio (chilblains) in a series of 104 patients at Mayo Clinic, 2000 to 2011 Mayo Clin Proc Cappel JA Wetter DA 2072158920142448513410.1016/j.mayocp.2013.09.020 · doi ↗ · pubmed ↗
- 8The cutaneous spectrum of lupus erythematosus Clin Rev Allergy Immunol Ribero S Sciascia S Borradori L Lipsker D 2913055320172875237210.1007/s 12016-017-8627-2 · doi ↗ · pubmed ↗