Epithelial Ingrowth Following Pterygium Excision With Conjunctival Autograft: A Rare Complication
Loubna Mouhib, Othman Haddani, Mehdi Khamaily, Mohamed Elbelhadji, Abdelbarre Oubaaz

TL;DR
A rare eye complication called epithelial ingrowth occurred in a patient after pterygium surgery, confirmed using imaging techniques.
Contribution
This is the second documented case of epithelial ingrowth following pterygium surgery with conjunctival autograft.
Findings
Epithelial ingrowth was diagnosed clinically and confirmed with anterior optical coherence tomography.
The lesion appeared as a thin, grey-white band outside the visual axis in the inferior-temporal quadrant.
This case highlights the rare but possible complication of epithelial ingrowth after pterygium surgery.
Abstract
Pterygium is a common ocular condition characterized by a conjunctival growth over the cornea. Epithelial ingrowth (EI), a rare complication of ocular surgery, involves the proliferation of epithelial cells within the cornea or the anterior chamber. We report a case of EI in a male patient following pterygium surgery with conjunctival autograft. Slit lamp examination revealed a thin, grey-white, wave-like band beneath the corneal epithelium in the inferior-temporal quadrant, outside the visual axis and not crossing the corneal center. The diagnosis of epithelial ingrowth was made clinically and confirmed with anterior optical coherence tomography (OCT). This marks only the second documented occurrence of EI after pterygium surgery.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
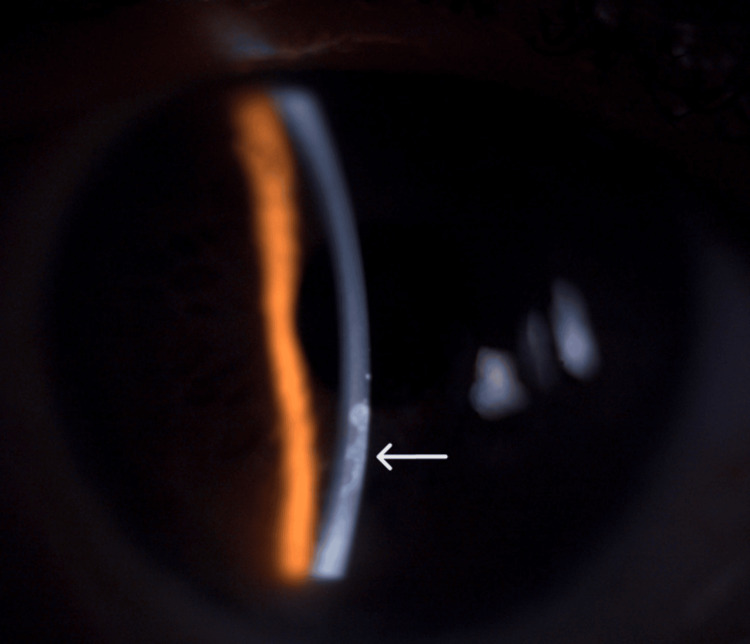 Figure 1
Figure 1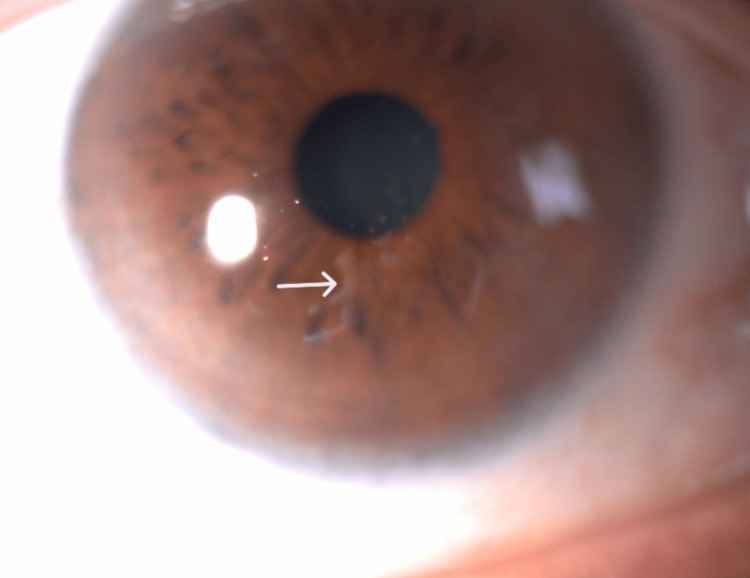 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4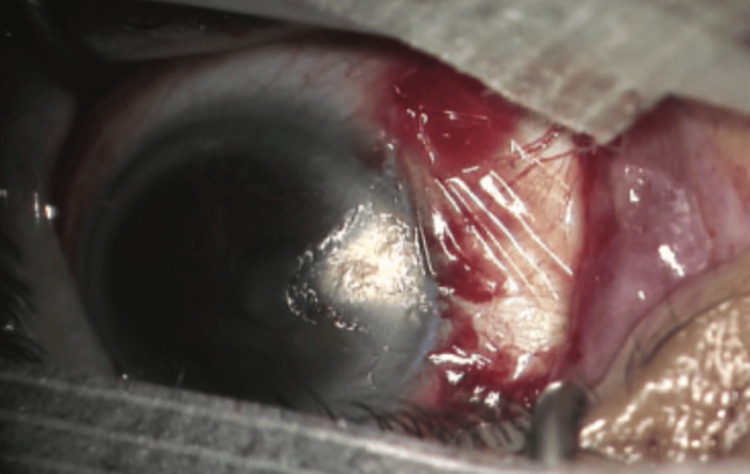 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCorneal Surgery and Treatments · Ocular Surface and Contact Lens · Ocular Disorders and Treatments
Introduction
Epithelial ingrowth (EI) is an abnormal epithelial membrane that develops within the eye; it can spread over the posterior surface of the cornea and infiltrate the anterior chamber angle [1], inside the cornea between the stroma and Bowman membrane or under a LASIK flap [2]. It can lead to significant clinical manifestations such as glaucoma or corneal edema [1]. This condition is a known complication of incisional ocular procedures and LASIK [2]. At the time of writing, only one prior case of epithelial ingrowth following pterygium surgery has been identified in the literature [1], marking this as the second documented occurrence.
Case presentation
A 63-year-old male attended an ophthalmic consultation due to monocular diplopia and blurred vision in his right eye. He had undergone temporal pterygium excision surgery with conjunctival autograft in the right eye eight weeks earlier with no perioperative complications. His best-corrected distance visual acuity was 20/22 OD (+1.50 (-1.50 at 115°)) and 20/20 OS (+1.50 (-1.50 at 115°)) with intraocular pressure of 18 and 19 mmHg, on-air tonometry confirmed by applanation. On slit-lamp biomicroscopic examination, a thin, grey-white band beneath the corneal epithelium with a wave-like shape was observed in the inferior-temporal quadrant of the cornea (Figure 1). The lesion was outside the visual axis and wasn’t crossing the center of the cornea (Figure 2).
Epithelial ingrowth beneath the corneal epithelium on slit lamp with a 30° view (white arrow)
Epithelial ingrowth on the inferior-temporal quadrant of the cornea (white arrow)
The endothelium and anterior chamber structures were unremarkable. On gonioscopy, there were no epithelial cells in the angle. The fundus examination revealed no abnormalities in either eye. Anterior segment optical coherence tomography (OCT) showed multiple discrete hyper-reflective membranes beneath the corneal epithelium and the Bowman membrane inside the anterior stroma (Figure 3).
Anterior optical coherence tomography (OCT) showing hyper-reflective membrane between the stroma and the corneal epithelium (white arrow)
The anterior OCT and clinical examination confirmed the diagnosis of epithelial ingrowth. Various methods can be used to treat epithelial ingrowth. We recommended therapeutic photo keratectomy (TPK), but the patient declined because he was satisfied with his new optical correction and aware of the high recurrence rate associated with the treatment.
Discussion
Pterygium is a common ocular condition characterized by conjunctival growth over the cornea (Figure 4). It can develop on either the nasal or temporal side, potentially affecting the cornea and causing astigmatism. Several surgical techniques are available for the pterygium. After it is removed, it can be replaced by a conjunctival autograft, conjunctival suture, or amniotic membrane (Figure 5) [3].
Temporal pterygium with a corneal invasionReproduced under CC BY-NC 4.0 from [3]
Pterygium removal with amniotic membrane graftReproduced under CC BY-NC 4.0 from [3]
The conjunctival autograft is the most commonly used method, despite its reported recurrence rate of 31.3% [4]. Surgical complications associated with these procedures are uncommon. Rare instances of complications in pterygium treatment include scleral ulceration, corneal infection, graft rejection, poor epithelial healing, glaucoma, endophthalmitis, and superficial punctate keratitis have been reported [5]. Epithelial ingrowth is an infrequent complication following various types of ocular surgeries. Our case marks the second documented instance after pterygium surgery [1].
After surgery on the cornea, epithelial cells begin their healing process by releasing many cytokines such as interleukin-1, epidermal growth factor, and tumor necrosis factor-alpha (TNF-a) [6]. This healing process is the first step of the pathogenesis of the epithelial ingrowth [7]. Epithelial conjunctival cells then disseminate inside a space (intra-stromal or intraocular). These epithelial cells can multiply due to the cytokine storm inside a tissue without destroying it. It results in a membrane on the endothelium that can spread to the iridocorneal angle or inside a space in the cornea (Lasik flap, pterygium scar).
The hypothesized mechanism in our case was likely an overly deep excision of the pterygium at the corneal level, reaching the anterior stroma, where epithelial cells adhered and proliferated on this newly created space. This condition can cause decreased vision by secondary astigmatism or by affecting the visual axis [8]. It is not the case with our patient.
Khurana et al. reported a case of epithelial ingrowth following cataract surgery and recommended avoiding incisions at the pterygium site [8]. Besides cataract and pterygium surgery, epithelial ingrowth is a well-known complication in the refractive surgery field [2]. There are reports of post-Lasik epithelium ingrowth (PLEI) [2] in the early postoperative period. The incidence is between 0-3.9% [9] for the first LASIK treatment, and more around 10-20% in cases of re-treatment [10].
For diagnostic purposes, confocal microscopy can help confirm that the epithelial cells exhibit characteristics consistent with conjunctival cells [8].
EI treatment methods vary based on the location of the epithelial cells. If the cells invade the iridocorneal angle and give rebel hypertonia to medical treatment, a trabeculectomy with mitomycin C should be performed to help lower the hypertonia [1]. When the EI invades a significant portion of the corneal endothelium resulting in various symptoms, a penetrating keratoplasty [1] or a Descemet membrane endothelial keratoplasty (DMEK) can be performed. If the cells develop on the anterior layers such as the anterior stroma or Bowman membrane, less invasive techniques can be used, such as anterior lamellar keratoplasty (ALK) or therapeutic photokeratectomy (TPK) [10].
Monitoring the patient is recommended if the EI doesn’t reach the visual axis and doesn’t have significant symptoms, like in our case. In PLEI, it is suggested that the best method is the flap opening with mechanical debridement of the cells [11]. Closing the flap with a 10-0 suture or fibrin glue may reduce the recurrence risk [2]. Another technique for the PLEI that has been reported and tested involves noninvasive neodymium-doped yttrium aluminum garnet (Nd:YAG) [12], with low energy in an average of 0.6 MJ. Various other methods appear in the literature including approaches such as wide excision with a corneoscleral patch graft, transcorneal cryotherapy, 5-fluorouracil, or mitomycin-C [13-15]. With all these therapeutic options, it is advised to keep in mind that EI has a high rate of recurrence after treatment [8].
Conclusions
Epithelial ingrowth is an infrequent complication following pterygium surgery. It has been described in other conditions such as post-LASIK or incisional surgeries. Therapeutical options are non-codified, and should be evaluated on an individual basis, taking into account the symptoms, clinical characteristics, and cell location.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epithelial ingrowth following surgery of recurrent pterygium Int Ophthalmol Ghosh S Mukhopadhyay S 6365282008 https://doi.org/10.1007/s 10792-007-9107-01758537410.1007/s 10792-007-9107-0 · doi ↗ · pubmed ↗
- 2Epithelial ingrowth following laser in situ keratomileusis (LASIK): prevalence, risk factors, management and visual outcomes BMJ Open Ophthalmol Ting DS Srinivasan S Danjoux JP 03201810.1136/bmjophth-2017-000133 PMC 589597529657982 · doi ↗ · pubmed ↗
- 3Dehydrated amniotic membrane in pterygium surgery Eur J Med Health Sci Khamaily M Haddani O Mouhib L 192462024
- 4Outcome of pterygium surgery: analysis over 14 years Eye (Lond) Fernandes M Sangwan VS Bansal AK 118211901920051554319010.1038/sj.eye.6701728 · doi ↗ · pubmed ↗
- 5Treatment of early pterygium recurrence with topical administration of interferon alpha-2b Can J Ophthalmol Esquenazi S 1851874020051604953310.1016/S 0008-4182(05)80031-6 · doi ↗ · pubmed ↗
- 6Epithelial ingrowth after laser in situ keratomileusis Am J Ophthalmol Wang MY Maloney RK 74675112920001092698310.1016/s 0002-9394(00)00357-3 · doi ↗ · pubmed ↗
- 7Wound healing in the cornea: a review of refractive surgery complications and new prospects for therapy Cornea Netto MV Mohan RR Ambrósio R Jr Hutcheon AE Zieske JD Wilson SE 5095222420051596815410.1097/01.ico.0000151544.23360.17 · doi ↗ · pubmed ↗
- 8Epithelial ingrowth post phacoemulsification in a case of recurrent pterygium Cornea Khurana S Gupta PC RB Sharma VK Ram J 1291313920203157405010.1097/ICO.0000000000002158 · doi ↗ · pubmed ↗