Spontaneous Uterine Rupture Secondary to Pyometra in a Postmenopausal Patient
Oscar Antonio Regalado Morales, José Luis Herrera Alanís, Luis Alberto Solís García, Abraham Alejandro Zorrilla Silva, Marcelo Valdés Hernández

TL;DR
An 86-year-old postmenopausal woman experienced a life-threatening uterine rupture caused by pyometra, diagnosed using CT imaging.
Contribution
Highlights a rare but severe complication of pyometra in elderly women and emphasizes the role of CT in diagnosis.
Findings
Pyometra can lead to spontaneous uterine rupture in postmenopausal women.
CT imaging is critical for diagnosing pyometra and differentiating it from other abdominal conditions.
Prompt diagnosis and treatment are essential to reduce mortality from this complication.
Abstract
Pyometra is the accumulation of purulent material in the endometrial cavity. It is an uncommon condition in postmenopausal women that can lead to uterine rupture, a complication with high mortality if not treated promptly. Imaging studies, particularly computed tomography (CT), play a fundamental role in diagnosing this condition and excluding more common pathologies. We present the case of an 86-year-old female patient with an acute abdomen secondary to uterine rupture due to pyometra diagnosed via CT.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
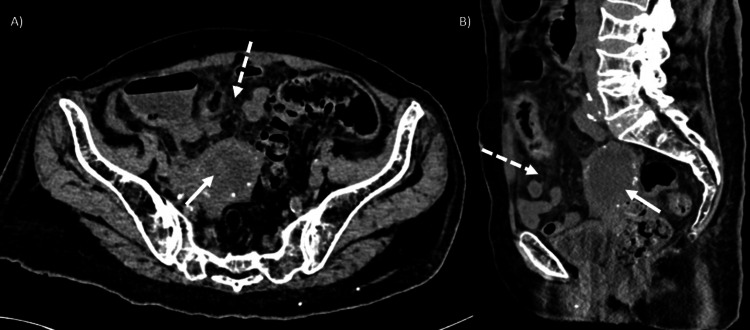 Figure 1
Figure 1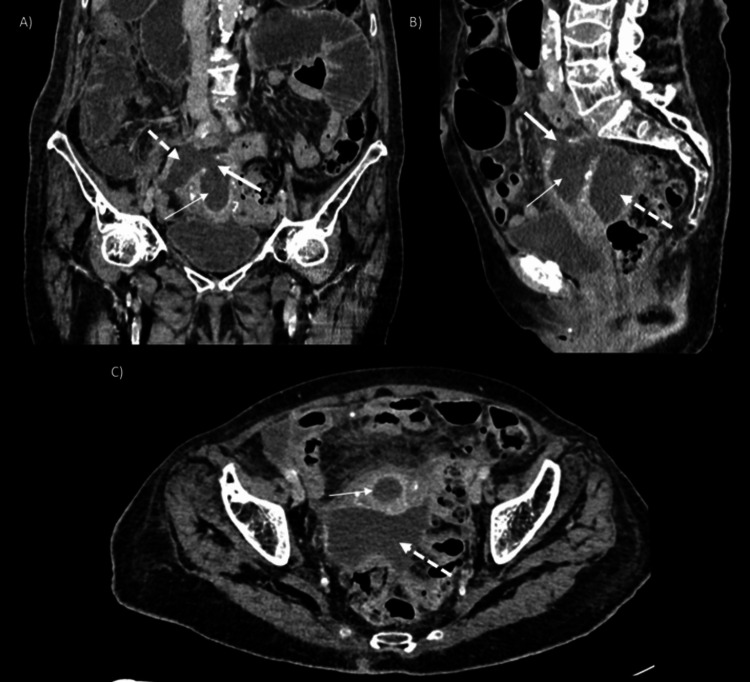 Figure 2
Figure 2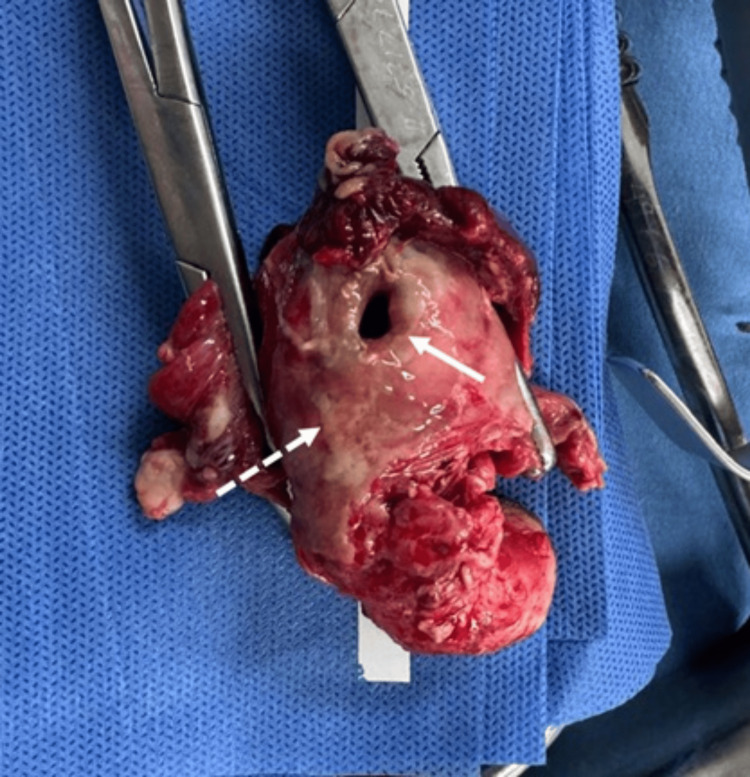 Figure 3
Figure 3| Laboratory Test | Result | Unit | Reference |
| Leukocytes | 28.1 | 10^3/uL | 4.5-10.5 |
| Neutrophils | 26.9 | 10^3/uL | 2.10-6.10 |
| Hemoglobin | 12.1 | g/dL | 12-16 |
| Hematocrit | 37 | % | 37-47 |
| Platelets | 368 | 10^3/uL | 140-400 |
| Glucose | 89 | mg/dL | 74-106 |
| Creatinina | 1.2 | mg/dL | 0.50-1.30 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Gynecological conditions and treatments · Endometriosis Research and Treatment
Introduction
Acute abdomen is one of the leading causes of hospital admission in elderly individuals, accounting for up to 25% of emergency visits [1]. Among its primary etiologies in the geriatric population, biliary tract diseases are the most frequent, followed by nonspecific abdominal pain, malignant neoplasms, intestinal obstruction, and complicated hernias [2]. However, due to the nonspecific nature of clinical findings, up to 40% of patients receive an incorrect diagnosis, delaying treatment and increasing mortality [3].
Gynecological causes are not among the most common etiologies of acute abdomen in this age group; therefore, when they occur, their diagnosis presents a challenge that may lead to adverse health outcomes for patients [2].
In this study, we present the case of a postmenopausal patient with an acute abdomen secondary to uterine rupture due to pyometra.
Case presentation
An 86-year-old female patient presented to the emergency department with diffuse abdominal pain, rated 8/10 on the visual analog scale (VAS). Physical examination revealed tenderness on palpation and signs of peritoneal irritation. Laboratory studies showed leukocytosis with neutrophilic predominance (Table 1).
Due to the clinical presentation, an initial diagnosis of acute diverticulitis was considered. A non-contrast abdominal CT scan was performed, revealing a heterogeneous-appearing uterus with hypodense material in the endometrial cavity, associated with increased adjacent fat density (Figure 1). No signs of diverticulitis or intestinal perforation were identified.
Computerized tomography in a simple phase of the abdomen.Axial (A) and sagittal (B) CT scans show a heterogeneous-appearing uterus with hypodense material in the endometrial cavity (thick arrow), associated with increased adjacent fat density (thick arrow).
A conservative management approach was initially chosen; however, in the following days, the patient's abdominal pain worsened, prompting a new contrast-enhanced CT scan. This time, the scan showed distension of the endometrial cavity with a defect in the uterine wall at the fundus, communicating with an abscess in the pouch of Douglas, findings consistent with uterine perforation secondary to pyometra (Figure 2).
Computerized tomography in the venous phase of the abdomen.Coronal (A), sagittal (B) and axial (C) CT scans show distension of the endometrial cavity (thin arrow) with a 1.5-cm diameter defect in the uterine wall at the fundus (thick arrow) communicating with an abscess in the pouch of Douglas (dotted arrow).
Given these findings, an emergency laparotomy was performed, confirming a perforation at the uterine fundus associated with an abscess in the pelvic cavity. A total hysterectomy with bilateral salpingo-oophorectomy and abscess drainage was performed, with a total volume of 200 cc (Figure 3).
Gross photograph of the uterus after total hysterectomy with bilateral salpingo-oophorectomy.This image shows a defect in the uterine wall at the fundus, consistent with rupture (thick arrow). Additionally, purulent exudate is seen covering the uterine serosa (dotted arrow).
Discussion
Uterine perforation or rupture refers to a defect in the myometrium that creates communication between the endometrial and abdominal cavities. While both terms can be used interchangeably, "rupture" is typically preferred when the cause is non-iatrogenic. The etiology is classified into gravid and non-gravid causes, with pyometra being one of the rarest non-gravid causes. This condition is characterized by the accumulation of purulent material within the endometrial cavity [4]. Uterine rupture secondary to pyometra is an extremely rare complication, with an estimated incidence of 0.01% to 0.05% [5].
This condition primarily affects elderly women, with a mean age of 75 years [6]. It results from obstruction of the uterine drainage pathway, which may be secondary to benign or malignant pathologies, including cervical stenosis, post-radiation changes, pelvic inflammatory disease, polyps, and leiomyomas [7]. The obstruction leads to endometrial cavity distension, ultimately causing necrosis of the uterine wall and subsequent perforation, with the uterine fundus being the most affected site due to its lower vascularity [4]. The main isolated microorganisms are Escherichia coli, Staphylococcus aureus, and Streptococcus species [8].
Clinically, pyometra is associated with a classic triad of purulent vaginal discharge, postmenopausal bleeding, and abdominal pain. However, up to 50% of cases may be asymptomatic [9]. When uterine rupture occurs, patients present with signs of an acute abdomen and peritoneal irritation [4].
The preoperative diagnosis of uterine rupture is complex, often requiring emergency laparotomy for confirmation due to the nonspecific nature of clinical findings [8]. Imaging studies play a fundamental role in evaluating this pathology, with ultrasound and computed tomography being the most commonly used modalities. On ultrasound, pyometra appears as a heterogeneous collection within the endometrial cavity, occasionally containing echogenic foci in the non-dependent portion of the uterus with posterior dirty shadowing, indicative of gas. On CT, findings are similar, with distension of the endometrial cavity and possible presence of intrauterine gas. Uterine rupture is identified as a defect in the uterine wall, frequently associated with abscess formation in the abdominal cavity and, in some cases, the presence of free air [4].
The treatment of pyometra involves drainage of the endometrial cavity along with antibiotic therapy. However, if uterine rupture is suspected, emergency laparotomy is essential, as this condition carries a mortality rate of up to 31% [10].
Conclusions
Uterine rupture secondary to pyometra is a rare cause of abdominal pain in elderly patients. Its clinical manifestations and physical examination findings are often nonspecific, leading to potential misdiagnosis with more common pathologies and delayed treatment. Imaging studies, particularly abdominal computed tomography, play a key role in diagnosis, allowing not only the identification of this entity but also the exclusion of other possible causes. Characteristic findings include discontinuity of the endometrial wall associated with abscess formation, guiding prompt diagnosis and appropriate management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Factors associated with serious abdominal conditions in geriatric patients visiting the emergency department BMC Emerg Med Dadeh AA Uppakarnnuntakul W 162420243827325010.1186/s 12873-024-00934-x PMC 10809639 · doi ↗ · pubmed ↗
- 2Abdominal pain in the elderly Emerg Med Clin North Am Martinez JP Mattu A 3710371-88, vii 2420061658496210.1016/j.emc.2006.01.010 · doi ↗ · pubmed ↗
- 3Acute abdominal pain in the elderly Geriatric Diseases Nagaratnam N Nagaratnam K Cheuk G 169177 Sydney Springer 2017
- 4Imaging evaluation of uterine perforation and rupture Abdom Radiol (NY) Aboughalia H Basavalingu D Revzin MV Sienas LE Katz DS Moshiri M 494649664620213412905510.1007/s 00261-021-03171-z · doi ↗ · pubmed ↗
- 5Uterine rupture due to pyometra and imperforate hymen in a 7-year-old girl: a case report J Pediatr Surg Case Rep Mahmood U Aziz MU Munawar M Amjad L Azmat CE Siddique S 1029211122025
- 6Spontaneous uterine perforation of pyometra presenting as acute abdomen Case Rep Obstet Gynecol Kitai T Okuno K Ugaki H Komoto Y Fujimi S Takemura M 738568201420142505742010.1155/2014/738568 PMC 4095732 · doi ↗ · pubmed ↗
- 7Computed tomography findings in a case of uterine rupture as a complication of pyometra Cureus Mohd Hanapiah F Ismail ZK Puteh O Aziz ME 016202410.7759/cureus.53154 PMC 1090103638420051 · doi ↗ · pubmed ↗
- 8Spontaneous uterine perforation due to pyometra: A rare cause of acute abdomen in a postmenopausal woman Int J Surg Case Rep Kishe A William D Moshi PG Marandu AA Mremi A Kimario AA 11115712920254010158410.1016/j.ijscr.2025.111157 PMC 11964646 · doi ↗ · pubmed ↗