Prosthetic Management of an Exenterated, Irradiated Orbital Defect Reconstructed with a Perforator Flap
Sandeep Gurav, Gurkaran Preet Singh, Radhika Jain, Ameya Bindu, Sagar Kulthe

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1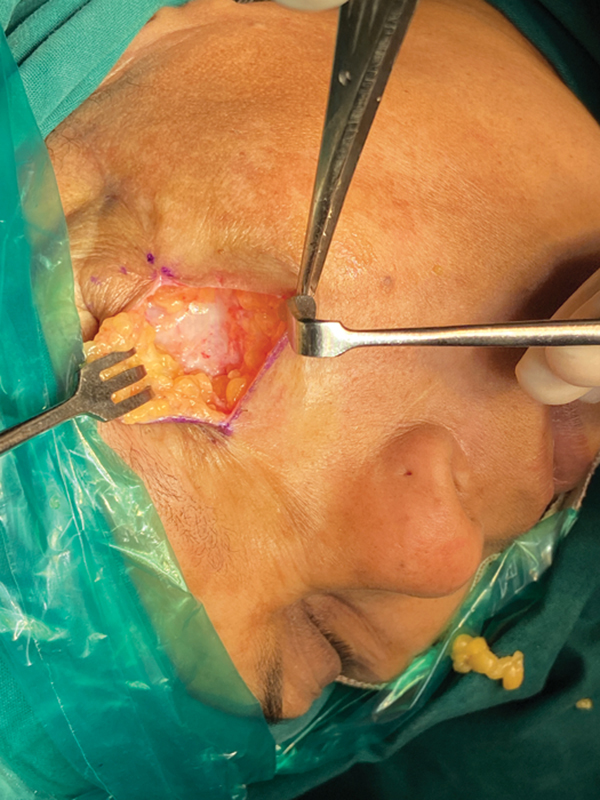 Fig. 2
Fig. 2 Fig. 3
Fig. 3 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Reconstructive Facial Surgery Techniques · Facial Trauma and Fracture Management
We describe a prosthetic procedure that involves secondary flap debulking of the medial sural artery perforator (MSAP) flap covering an exenterated orbital defect and eventual placement of a cosmetically acceptable silicone-based orbital prosthesis.
A 51-year-old woman underwent orbital exenteration along with left orbital wall excision for a recurrent adenoid cystic carcinoma (grade 3) of the left lacrimal gland in July 2022 ( Fig. 1 ). The defect was primarily reconstructed with MSAP. The patient received adjuvant radiation therapy to tumor bed at a dose of 64 Gy in 32 fractions 6 weeks postsurgery. The postoperative follow-up period was uneventful.
( A ) Preoperative image showing recurrent adenoid cystic carcinoma of the left lacrimal gland. ( B ) Postoperative image at 1.5 years of follow-up after surgical reconstruction. ( C ) Intraoperative image of the orbital surgical defect with the arrow pointing at the medial bony wall. ( D ) Reconstruction with the medial sural artery perforator flap.
She reported to our dental and prosthetic oncology unit 1 year postoperatively with a desire for an improved cosmesis. On assessment, a left exenterated defect was noted, covered with a healthy, bulky flap. The native skin was sagging at the inferior margin of the defect ( Fig. 1 ). One year had been completed postradiotherapy (PORT) and the patient was having a satisfactory Eastern Cooperative Oncology Group (ECOG-1) performance status. She was taken up for prosthetic space creation by a secondary flap thinning procedure, after corroboration with the department of plastic surgery. 1 Under general anesthesia, a midline incision was made and a subdermal full-thickness flap was raised. The adipose tissue was liberally removed, ensuring some fat was retained over the orbital bone ( Fig. 2 ). The end point of debulking was to obtain a depression similar to the depth of the contralateral normal eye. One week postoperatively, she was given a transitional acrylic conformer to ensure sustained gentle pressure on the healing tissues that served as a scaffold.
Highlight of the secondary flap thinning procedure where a midline incision was made and a subdermal full-thickness flap was raised. The adipose tissue was liberally removed, ensuring some fat is retained over the orbital bone.
One month later, when the final contours were achieved ( Fig. 3 ), we started with the fabrication of the final silicone orbital prosthesis. The prosthesis was processed from room temperature vulcanizing silicone (M511, Technovent) by our team of anaplastologists. Clinically, it was evaluated for fit, aesthetics, and comfort. The main mode of retention of the prosthesis was adhesive based as there were no anatomical undercuts to harness ( Fig. 4 ). Also, the fact that frontal bones were radiated precluded the possibility of orbital endosteal implants to aid in retention of the prosthesis.
The final well-settled, healed orbital cavity ready for placement of the final adhesive-retained silicone orbital prosthesis.
Final adhesive-retained silicone prosthesis with satisfactory aesthetics and retention.
MSAP flap is a versatile fasciocutaneous flap that is used for reconstruction of small to medium-sized head and neck defects. 2 As there was no muscle component in the MSAP flap, thickness of the resultant debulked tissue proved ideal for the prosthetic space creation. 3 We believe that careful planning regarding the appropriate time to intervene for various procedural steps such as time of debulking (1 year after PORT), time to place the conformer (1 week after initial healing), and duration of placement of conformer (at least 4 weeks) ensured sufficient time for healing and achieving satisfactory results. The fragile, irradiated tissue bed was cautiously manipulated by applying only gentle pressure with the use soft-tissue reline material under the acrylic conformer.
We could successfully demonstrate that it is possible to rehabilitate complex orbital defects by careful execution of soft-tissue procedures and use of innovative prosthetic techniques. The patient has been using her prosthesis regularly and attends her social and religious meetings with bolstered confidence.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hanasono M M Lee J C Yang J S Skoracki R J Reece G P Esmaeli B An algorithmic approach to reconstructive surgery and prosthetic rehabilitation after orbital exenteration Plast Reconstr Surg 2009123019810519116542 10.1097/PRS.0b 013e 3181904 b 95 · doi ↗ · pubmed ↗
- 2Agrawal G Gupta A Chaudhary V Qureshi F Choraria A Dubey H Medial sural artery perforator flap for head and neck reconstruction Ann Maxillofac Surg 2018801616529963426 10.4103/ams.ams_137_17PMC 6018300 · doi ↗ · pubmed ↗
- 3Al Omran Y Evans E Jordan C The medial sural artery perforator flap versus other free flaps in head and neck reconstruction: a systematic review Arch Plast Surg 2023500326427337256040 10.1055/a-2059-4009 PMC 10226800 · doi ↗ · pubmed ↗