Index microvascular resistance (IMR) in heart transplant patients (IMR-HT study): Study protocol
Ainhoa Pérez-Guerrero, Jean Paul Vilchez-Tschischke, Luis Almenar Bonet, Jose Luis Diez Gil, Teresa Blasco Peiró, Salvatore Brugaletta, Josep Gomez-Lara, José González Costello, Paula Antuña, Vanesa Alonso Fernández, Fernando Sarnago Cebada, María Dolores García-Cosio

TL;DR
This study explores using a heart function measure called IMR to identify heart transplant patients at higher risk of rejection or complications, potentially reducing the need for invasive biopsies.
Contribution
The study introduces a novel approach to managing heart transplant patients by using IMR to guide clinical decisions and reduce endomyocardial biopsies.
Findings
IMR assessment is feasible and safe in heart transplant patients.
Early high IMR values are linked to acute rejection and worse outcomes.
IMR could guide personalized management and reduce invasive procedures.
Abstract
Acute allograft rejection (AAR) is an important cause of morbi mortality in heart transplant (HT) patients, particularly during the first year. Endomyocardial biopsy (EMB) is the “gold standard” to guide post- heart transplantation treatment. However, it is associated with complications that can be potentially serious. The index of microvascular resistance (IMR) is a specific physiological parameter used to assess microvascular function. Invasive coronary assessment has been shown to be both feasible and safe. Detection of coronary microvascular dysfunction (MCD) by IMR may help to identify high risk HT patients. In fact, an increased IMR measured early after HT has been associated with AAR, higher all-cause mortality and adverse cardiac events. A high IMR value early after HT may identify patients at higher risk who require increased surveillance or adjustments in immunosuppressive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
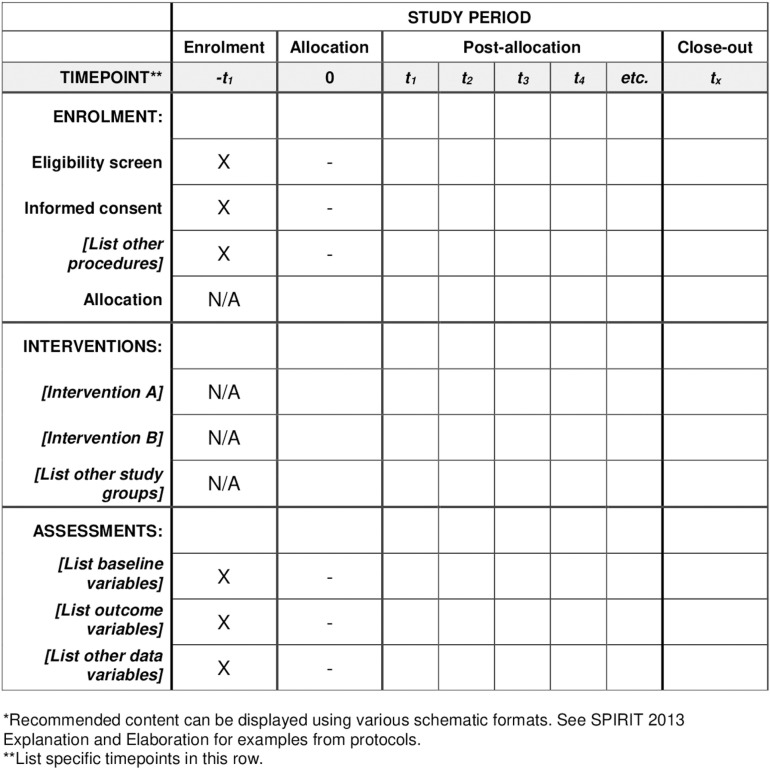 Fig 1
Fig 1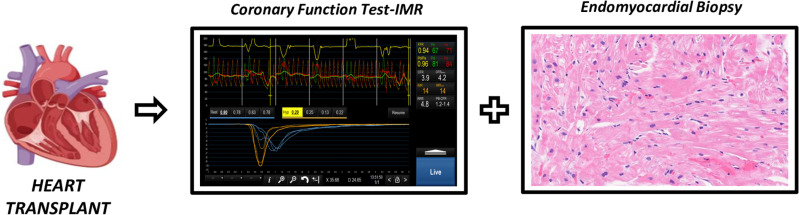 Fig 2
Fig 2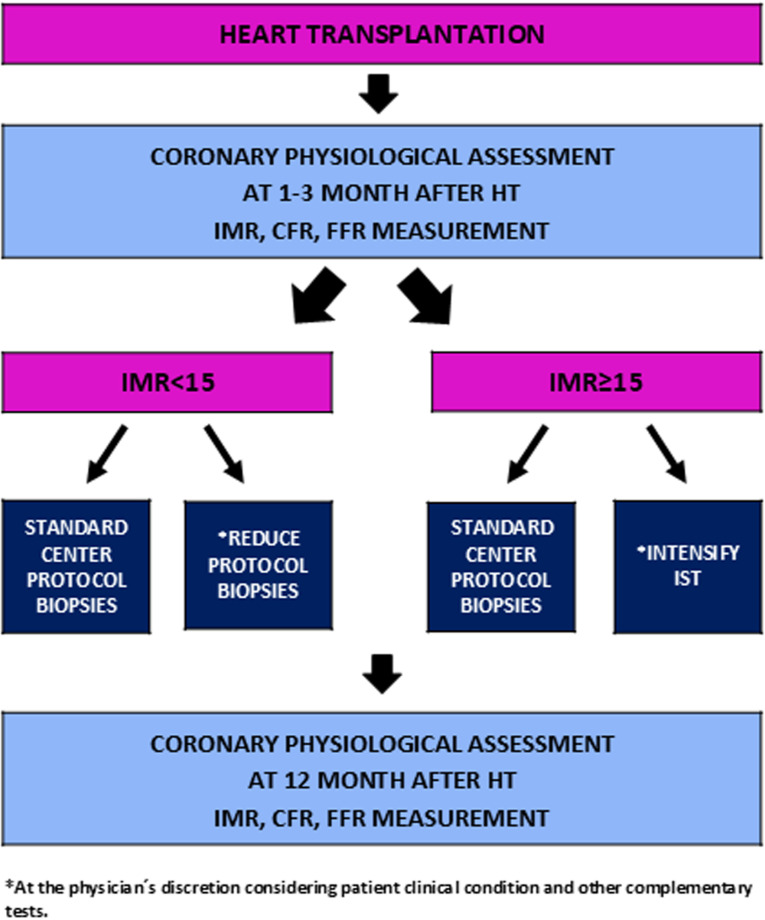 Fig 3
Fig 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Viral Infections and Immunology Research · Renal Transplantation Outcomes and Treatments
Introduction
Acute allograft rejection (AAR) is an important cause of morbi mortality after heart transplant (HT), particularly within the first year[1–3]. Advances in immunosuppression, donor heart evaluation, surgical techniques, and post-transplantation care have led to a gradual reduction in AAR and improved survival after HT over time. Endomyocardial biopsy (EMB) is the gold standard method to guide post-HT treatment, as it represents the best tool to identify rejection in orthotopic HT [4–5]. However, it is usually repeated up to 5 times during the first year - with some variations depending on each center protocol - and it is potentially associated with serious complications.
Several studies have presented the association between AAR, micro-vasculopathy and cardiac allograft epicardial vasculopathy (CAV) [6–9]. Index of microcirculatory resistance (IMR) measured early after heart transplantation has been significantly associated with the risk of acute cellular rejection (ACR), and patients with IMR ≥ 15 have higher risk of AAR for 2 years follow-up [10].
Our aim is to evaluate IMR in heart transplant patients within the first year. Changes in management after knowing IMR values and prognostic implications of IMR in a long term follow up will also be assessed.
Methods
Rationale and design
The IMR-HT study is a multicenter, prospective study aimed to assess IMR values within the first year after heart transplant.
Changes in HT patient management (number of EMBs, immunosuppressive therapy modifications) after knowing IMR values will also be assessed, as well as the prognostic implications of IMR baseline and annual values.
It will enroll consecutive eligible patients who undergo HT in each participation center.
Hypothesis
There are few studies that evaluate IMR after a heart transplant. High IMR baseline value will identify patients at higher risk and will lead to modifications in the number of biopsies and/or immunosuppressive therapy within one year. Patients with an increase in IMR over the first year will have a higher rate of cardiac events.
Patient selection
Patients undergoing HT will be screened for enrollment. To maximize patient inclusion, we apply broad inclusion criteria and strict exclusion criteria, as specified in Table 1. Eligible patients will be informed about the study and will have to provide written informed consent prior to being included. The recruitment begins on May 23^rd^, 2023, the expected recruitment period is two years. The study completion date is estimated in 2030. This study adhered to the principles outlined in the Declaration of Helsinki. The approval was granted by the Ethics Committee for Investigation of Aragon (CEICA). The study has been registered at Clinical-Trials.gov (NCT 06656065).
Table 1: Eligibility criteria.
The schedule of enrollment, interventions and assessments and the timeline of the study are detailed in Fig 1.
Schedule of enrolment, interventions, and assessments.
Clinical conditions, laboratory findings and clinical events will be assessed at one month and one year. Follow up will be extended for up to five years.
Invasive physiological evaluation of the coronary microcirculation.
Patients included will undergo a coronary angiography between the first and third month after HT. This coronary angiography is part of the follow-up protocol in most centers also including EMB (Fig 2**).**
Coronary function test and endomyocardial biopsy between the first and third month after heart transplant.
Assessment of IMR, coronary flow reserve (CFR) and fractional flow reserve (FFR) will be performed using the standard technique [11–13]. The left anterior descending coronary artery will be evaluated in all patients. Circumflex or right coronary artery could be additionally evaluated at operator’s discretion. An intracoronary pressure and temperature sensor-tipped guidewire (Pressure Wire ^TM^ X guide- wire 0.014’, Abbott, IL, USA) will be used to perform the measurements. The tip pressure sensor will be advanced into the mid-to-distal portion of the evaluated vessel (50 to 60 mm of the ostium of selected coronary artery). Baseline aortic pressure (Pa) and distal intracoronary pressure (Pd) will be obtained to calculate the resting index Pd/Pa. To measure the mean transit time (Tmn) under basal conditions, intracoronary administration of 3 mL of room-temperature saline will be manually injected three times in succession (3 mL/s). Then maximal hyperemia will be induced using adenosine iv (140 to 180 mg/kg/min) and three additional intracoronary room temperature saline boluses of 3 ml will be administered to determine the mean transit time at hyperemia (Tmnh). Deviations > 10% in some of the individual Tmn values will force their repetition. Both at rest and in hyperemia, the mean of the three individual determinations will be used for the calculations. Finally, fractional flow reserve (FFR), coronary flow reserve (CFR) and IMR will be calculated using the software Coroventis Coroflow (Abbott, Coroventis Uppsala, Sweden). Physiological indexes are listed in Table 2.
Table 2: Calculation FFR, IMR and CFR.
Fractional flow reserve (FFR) is defined as the ratio of maximal coronary blood flow in a diseased artery to the maximal coronary blood flow in the same artery without stenosis. FFR serves as a surrogate marker of inducible myocardial ischemia caused by epicardial coronary stenosis.Coronary flow reserve (CFR) is the ratio of hyperemic to baseline coronary blood flow and acts as a marker of the integrity of both epicardial and microvascular coronary circulation. Therefore, CFR reflects microvascular status in the absence of significant epicardial disease.Index of Microcirculatory Resistance (IMR) represents the minimum achievable resistance in the coronary microcirculation and is a more specific marker of microvascular function. IMR is defined as the distal coronary pressure divided by the inverse of the hyperemic mean transit time and is expressed in units of mmHg.s.
The physiological assessment of IMR, CFR, and FFR will be repeated one year after HT.
Biopsies and immunosuppressive treatment.
Based on previously published clinical data on IMR in heart transplant patients, a post-HT management algorithm is proposed:
IMR < 15: The frequency of biopsies could be reduced or maintained as per protocol. No changes to immunosuppressive therapy would be required.IMR ≥ 15: Biopsies would be performed at the standard frequency according to protocol. Immunosuppressive therapy could be intensified or maintained the same.
The number of biopsies performed by each center, as well as changes in immunosuppressive therapy after knowing IMR baseline values will be assessed. Of note, given the observational characteristics of the study, clinical management decisions will be made at the discretion of the treating physician, considering the patient’s clinical condition and other complementary tests.
Both groups (IMR < 15 vs IMR ≥ 15) will be compared in terms of cardiac events occurrence.
The prognostic implications of IMR variation (if that is the case) between the first three months and one year will also be analyzed.
The results of this observational trial will help in the conduct of a randomized trial in which an EMB will be spared based on the IMR value.
The proposed study algorithm is shown in Fig 3. Participating centers are listed in Supplementary Table 1.
Study proposed algorithm.
Data collection.
Sociodemographic, clinical, laboratory and follow-up data of each patient will be included in a database specifically designed for the study. All variables will be included in the online data collection platform Redcap (Research Electronic Data Capture). Each patient will be assigned a number; their identity will not be revealed in any case. All shared information will be anonymized.
Study endpoints.
The main objective of the study is to evaluate IMR values in the first three months and one year after heart transplant. Secondary endpoints are detailed in Table 3. End-points will be evaluated at 1 year and annually thereafter for up to 5 years. Definition of events is detailed in Table 4.
Table 3: Secondary endpoints.
Table 4: Definition of events.
Statistical analysis and sample size considerations.
The characteristics of the study population will be summarized using standard descriptive statistics. Continuous variables will be expressed as mean ± standard deviation (SD) or median [interquartile range (IQR)], as appropriate. Categorical variables will be presented as absolute numbers and percentages. For the comparison of means, the Student’s t-test for independent samples or the non-parametric Mann-Whitney U test will be used for dichotomous qualitative variables. For non-dichotomous qualitative variables, the ANOVA test or the non-parametric Kruskal-Wallis test will be applied. For bivariate analysis of qualitative variables, the Chi-square test or Fisher’s exact test will be used, as appropriate. Event comparisons between groups will be performed using Kaplan-Meier curves, and a Cox regression analysis will be conducted to adjust for confounding factors and identify independent predictors of clinical events. A two-tailed p-value < 0.05 will be considered statistically significant. All statistical analyses will be performed using SPSS software.
Given the exploratory nature of the study, no formal power calculation is required. In 2023, approximately 325 heart transplants (HT) were performed in Spain. With a median of 10–15 HTs per center and considering the participation of eight centers that routinely perform invasive coronary physiology, data will be analyzed once 100 patients have completed their first-year follow-up [3]
Discussion
Heart transplant is considered the treatment of choice in patients with advanced heart failure refractory to medical treatment or devices [1–2].
AAR plays an important role in determining prognosis: up to 20% of HT patients experience at least one episode of ACR in the first-year post-transplant [1]. The immune response is classified into ACR when it is mediated by T lymphocytes and humoral rejection when the main mechanism involves B lymphocytes and antibody production [4,5,14]. Advances in immunosuppressive therapy (IST), donor heart evaluation, surgical techniques and post-HT care have led to a reduction in ACR, improving survival over time [4]. Post-transplant IST includes three basic components: a calcineurin inhibitor (currently preferred Tacrolimus), an antiproliferative agent (mycophenolate mofetil), and steroids. On the other hand, proliferation signal inhibitor (mTOR) drugs (everolimus and sirolimus) are primarily used for CAV [15]. CAV is the main cause of mortality after the first year of transplantation. It is characterized by diffuse intimal thickening affecting both coronary epicardial and microcirculation [4,15].
The vast majority of ACR occur asymptomatically, presenting normal ventricular function, and thus being detected through the routine EMB surveillance protocol [4]. The graduation of the RAC is detailed in the 2005 review of the ISHLT [14]. Due to intra- and inter-observer variabilities in determining different degrees of slight-moderate rejection, an update was published in the 2010 document. In the International Society of Heart and Lung Transplantation (ISHLT) guidelines, EMB was made a IIaC recommendation for the detection of rejection [16].
EMB is repeatedly performed during the first year after HT. It is often described as uncomfortable by patients, and is associated with complications that can be potentially serious, such is the case of cardiac perforation.
Moreover, EMB diagnostic yield is wide, with a high variability between observers and a non-negligible rate of false positives and negatives [17].
To avoid the inconveniences of EMB, non-invasive techniques such as cardiac magnetic resonance have been studied for detecting rejection. In recent years, advanced methods like gene expression profiling and plasma donor-derived cell-free DNA have also been introduced. However, their results have been highly variable, and these techniques have not been implemented in routine clinical practice in most of our centers [18,19]. For these reasons, none of these techniques has been able to replace EMB. IMR is a quantitative and specific index of coronary microcirculation that requires the use of a coronary guide and hyperemia to be analyzed. Both adenosine and the use of a coronary wire could cause adverse symptoms [20]. However, the rate of potential serious adverse events is equivalent to that of routine diagnostic coronary angiography (<1%) [21]. Particularly in heart transplant patients, Duran SR et al. showed no complications when using adenosine at a rate of 140 mcg/kg/min in 16 pediatric patients undergoing MR stress perfusion cardiac magnetic resonance [22]. There are no studies comparing IMR with other non-invasive tools for the detection of AAR. However, rather than a substitute, IMR may be a complementary technique for rejection surveillance in HT patients.
Some concerns may arise regarding the performance of an invasive microvascular function test, as it requires the use of a coronary guide and, consequently, heparin administration along with EMB extraction in the same procedure. However, this approach has been successfully implemented in other trials aimed at identifying CAV through intracoronary imaging techniques in HT patients, without any significant complications [23].
An increased IMR in the graft has been associated with higher all-cause mortality and adverse cardiac events regardless of epicardial vasculopathy. Several IMR cut-off (from 15 to > 20) have been associated with ACR within the first year after HT. Patients in whom IMR decreases or does not change one year after HT have a higher event-free rate than those patients in whom the IMR increases [8–10,24,25]. As far as we know, no study has evaluated IMR impact on post-HT management. A high IMR value early after HT may detect a higher risk patient that needs an increased surveillance or changes in immunosuppressive therapy (an earlier administration of mTor-inhibiting drugs or prescribing calcium antagonists, which are known to improve microvascular function). On the other hand, a low IMR value may lead to decrease the number of EMB.
Our aim will be to assess IMR values in heart transplant patients within one year and evaluate changes in management after knowing of IMR values. We believe it is important to move forward in AAR surveillance and reduce the number of endomyocardial biopsies. In addition to assessing their diagnostic capabilities, IMR should also be assessed based on clinical outcomes. Therefore, we are convinced the results of this trial will be very important for our HT patient population.
Conclusions
The IMR is a quantitative physiological parameter to evaluate coronary microcirculation. High IMR values have been associated with acute cellular rejection in heart transplant patients. The assessment of IMR may be useful for identifying high-risk heart transplant patients, leading to changes in management and prognosis.
Supporting information
S1 FileSPIRIT checklist(DOCX)
S2 TableSite centers and investigators.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lund LH, Edwards LB, Kucheryavaya AY, Benden C, Dipchand AI, Goldfarb S, et al. The registry of the international society for heart and lung transplantation: Thirty-second official adult heart transplantation report--2015; Focus theme: Early graft failure. J Heart Lung Transplant. 2015;34(10):1244–54. doi: 10.1016/j.healun.2015.08.003 26454738 · doi ↗ · pubmed ↗
- 2Khush KK, Cherikh WS, Chambers DC. The international thoracic organ transplant registry of the international society for heart and lung transplantation: Thirty-sixth adult heart transplantation report—2019; focus theme: donor and recipient size match. J Heart Lung Transplant. 2019;38(10):1056–66.31548031 10.1016/j.healun.2019.08.004PMC 6816343 · doi ↗ · pubmed ↗
- 3González Vílchez F, Almenar-Bonet L, Mitroi C, Crespo-Leiro MG, López-Granados A, et al. . Registro Español de Trasplante Cardiaco. Rev Esp Cardiol. 2024;77(11):926–35.39032818 10.1016/j.rec.2024.05.015 · doi ↗ · pubmed ↗
- 4Costanzo MR, Dipchand A, Starling R, Anderson A, Chan M, Desai S, et al. The international society of heart and lung transplantation guidelines for the care of heart transplant recipients. J Heart Lung Transplant. 2010;29(8):914–56. doi: 10.1016/j.healun.2010.05.034 20643330 · doi ↗ · pubmed ↗
- 5Marboe CC, Billingham M, Eisen H, Deng MC, Baron H, Mehra M, et al. Nodular endocardial infiltrates (Quilty lesions) cause significant variability in diagnosis of ISHLT Grade 2 and 3A rejection in cardiac allograft recipients. J Heart Lung Transplant. 2005;24(7 Suppl):S 219-26. doi: 10.1016/j.healun.2005.04.001 15993777 · doi ↗ · pubmed ↗
- 6Hartmann NE, Wellnhofer E, Knosalla C. Prognostic impact of microvasculopathy on survival after heart transplantation: evidence from 9713 endomyocardial biopsies. Circulation. 2007;116(11):1274–82.17709643 10.1161/CIRCULATIONAHA.106.647149 · doi ↗ · pubmed ↗
- 7Fearon WF, Balsam LB, Farouque HMO, Caffarelli AD, Robbins RC, Fitzgerald PJ, et al. Novel index for invasively assessing the coronary microcirculation. Circulation. 2003;107(25):3129–32.12821539 10.1161/01.CIR.0000080700.98607.D 1 · doi ↗ · pubmed ↗
- 8Ahn J-M, Zimmermann FM, Gullestad L, Angerås O, Karason K, Russell K, et al. Microcirculatory resistance predicts allograft rejection and cardiac events after heart transplantation. J Am Coll Cardiol. 2021;78(24):2425–35. doi: 10.1016/j.jacc.2021.10.009 34886963 · doi ↗ · pubmed ↗