Association between different types and characteristics of fetal deceleration during labour and neonatal acidemia at delivery: A case-control study
Maria Fogelberg, Charlotte Dahlbäck, Frida Ekengård, Gisela Rickle, Andreas Herbst

TL;DR
This study finds that certain types of fetal heart rate decelerations during labor are strongly linked to neonatal acidemia at birth.
Contribution
The study identifies specific deceleration patterns and their duration that are most strongly associated with acidemia, offering clearer clinical guidance.
Findings
Late and prolonged decelerations are strongly associated with acidemia.
Fetal heart rate below baseline for 50% of the time over 30 minutes is highly linked to acidemia.
Only duration >60s and loss of variability in variable decelerations are associated with acidemia.
Abstract
Classification of fetal heart rate (FHR) decelerations as suspicious or pathological differs between current interpretation templates for intrapartum cardiotocography. Decelerations are the most frequent FHR pattern irregularities during labour. The aim of this study was to assess the association between different types and characteristics of decelerations and acidemia at birth. This case-control study includes 365 cases with cord pH < 7.10 after 1st stage cesarean delivery or pH < 7.05 after vaginal delivery at > 34 + 0 weeks after induced or spontaneous labour, and 730 controls with pH ≥ 7.15. Cardiotocographic recordings from 60 min before birth were scrutinized and decelerations evaluated in detail. Odds ratios (OR) with 95 % confidence intervals for acidemia at birth were determined. The following types of decelerations were associated with acidemia: Late decelerations; OR 9.0…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
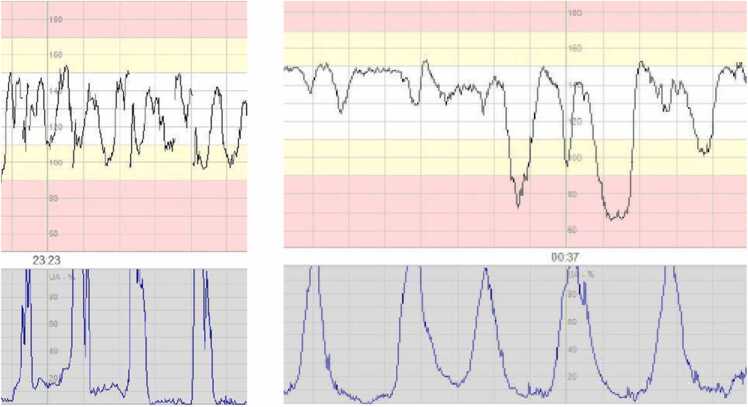 Figure 1
Figure 1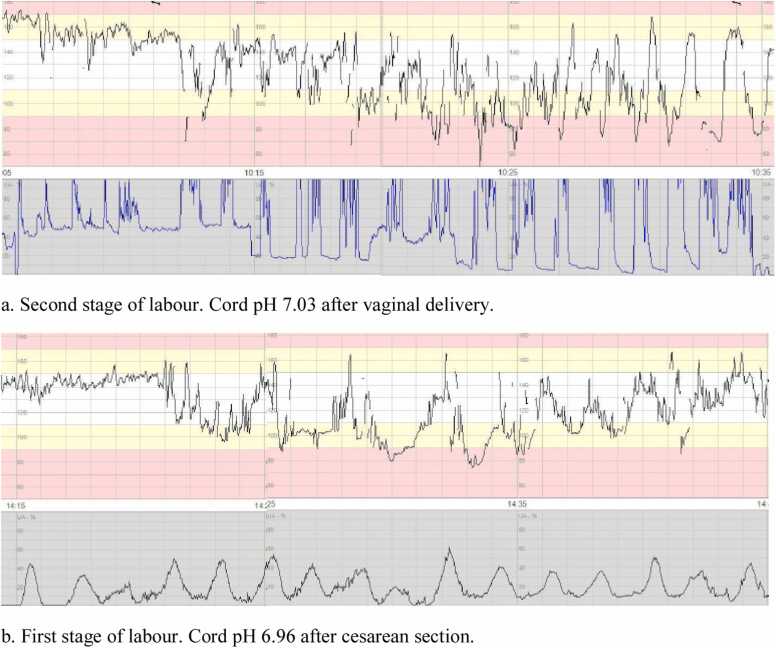 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and fetal brain pathology · Neonatal Respiratory Health Research · Cardiac Arrest and Resuscitation
Introduction
1
The purpose of cardiotocographic (CTG) monitoring during labour is to identify signs of fetal hypoxia before asphyxia ensues. Different guidelines with interpretation templates serve as decision aid for midwives and obstetricians [1], [2], [3], [4]. Since different CTG classification templates are restricted by either low sensitivity or low specificity [5], [6], [7], [8], efforts to improve the diagnostic precision are motivated.
One difference between current classification systems is that the fetal heart rate decelerations resulting in classification pathological differ [1], [2], [3], [4]. For example, according to the ACOG criteria, recurrent variable decelerations are classified as a category III pattern, whereas in the FIGO guidelines (2015) the presence of repetitive variable decelerations only results in a suspicious pattern. In the NICE guidelines (2022), a CTG pattern is classified as pathological if repetitive variable decelerations show additional concerning criteria for > 30 min.
The aim of this study was to determine the associations between acidemia at birth and fetal heart rate decelerations of different types and characteristics during labour. Our intention was to assess for which types of decelerations the association to acidemia is sufficiently high to motivate such a pattern to be included as “pathological” in a classification template.
The present study focused on FHR decelerations and only took other FHR variables into account when integrated in the assessment of variable decelerations in present classification templates, and in performing a sub-analysis including only traces with normal baseline and variability.
Methods
2
This is a retrospective case-control study including 365 cases with acidemia at birth and 730 controls. The studied CTG traces derive from births at Skåne University Hospital and Helsingborg Hospital in Region Skåne between 2012–2017. Part of the material has been used in previous studies [7], [8]. The material included singleton pregnancies with spontaneous or induced labour at > 34 completed gestational weeks. For inclusion, ≥ 30 min CTG recording before birth was required with a maximum gap of 30 min between end of recording and birth. A maximum of 10 min of non-interpretable CTG trace (due to poor contact, sequences of maternal heart rate or disconnected CTG) was accepted. All neonates born with acidemia during this period who met the inclusion criteria were included in the study.
In this study, acidemia was defined as cord artery or vein pH < 7.10 after cesarean delivery in the first stage of labour and pH < 7.05 after vaginal birth or second stage cesarean. The higher pH cut-off for the first stage of labour was motivated by the normal decrease of pH during the second stage of labour [9]. Severe acidosis at birth is often defined as pH < 7.0, but recent studies have shown that also pH between 7.00 and 7.19 and particularly pH < 7.10 increases the risk of adverse neonatal outcomes [10], [11]. Cord samples were taken immediately after birth by puncture of the intact cord, except in the case of cesarean section where the umbilical cord was clamped before samples were taken.
Controls were the first two eligible neonates born subsequently after each case in the same hospital. To be eligible as controls, umbilical artery and vein sampling needed to show an umbilical artery pH > 7.15 with an arterio-venous difference > 0.02, and Apgar scores 9 or 10 at five and ten min. Controls had to have > 30 min of CTG recording at the same cervical dilation as the trace from the corresponding case.
Totally 1095 CTG recordings were assessed during 2023–2025; 365 cases with acidemia and 730 controls. In the case group, 70 were delivered by cesarean in the first stage of labour, 24 by cesarean in the second stage, and 271 vaginally. Background data are presented in Table 1.Table 1. Summary of background data of cases and controls.Table 1. Cases n (%)Controls n (%)Missing data nTotal nTotal3647281092Primipara225 (61.0)356 (48.6)01092Instrumental delivery88 (24.2)45 (6.2)01092Cesarean section94 (25.8)12(1.6)01092Breech2 (0.5)1(0.1)01092Preterm birth < 37 + 08 (2.2)18 (2.5)01092Post-term birth ≥ 42 + 028 (7.7)50 (6.9)01092Birthweight < 2.5 kg5 (1.4)10 (1.4)31089Birthweight > 4.5 kg13 (3.6)18 (2.5)31089Epidural159 (43.7)215 (29.5)01092Oxytocin augmentation202 (55.5)252 (34.6)01092Fever/Infection11 (3.0)8 (1.1)01092Meconium stained amniotic fluid96 (26.4)137 (18.8)41088Diabetes22 (6.0)19 (2.6)01092Preeclampsia15 (4.1)16 (2.2)01092BMI < 25209 (57.4)433 (59.5)291063BMI > 3047 (12.9)80 (11.0)291063Smoking20 (5.5)54 (7.4)1810755-minute Apgar score < 747 (12.9)011091Cord artery pH available344 (94.5)728 (100)201072Cord vein pH available344 (94.5)728 (100)201072Both artery +vein pH available304 (83.5)728 (100)401052Cord artery or vein pH < 7.00104 (28.6)001092Cord artery or vein pH < 7.05328 (90.1)001092Cord artery or vein base deficit > 12 mmol/L96 (26.7)2 (0.3)131079
The CTG traces from the last hour before birth for cases and the corresponding period for controls were scrutinized and different decelerations were evaluated in detail categorizing each deceleration by type and characteristics. The total number of each type was assessed, as well as repetitivity (occurrence at ≥50 % of contractions).
Decelerations were defined as temporary slowing of the fetal heart rate (FHR) of > 15 beats per minute (bpm) below the baseline, except for late decelerations in a trace with reduced variability where an amplitude of 10 bpm was sufficient.
Early decelerations were defined as uniform periodic slowing of FHR with gradual onset before the contraction peak, ≥ 30 s from beginning to nadir, nadir within 20 s after the contraction peak, and gradual recovery. Late decelerations were defined as uniform periodic slowing of FHR with onset after mid of the contraction and nadir > 20 s after the contraction peak and ending after the contraction [1], [2].
Variable decelerations were defined as intermittent slowing of FHR with rapid onset, less than 30 s from beginning to nadir. Duration was determined as time from start of deceleration (pre-accelerations not included) to return to baseline. They were stratified into two groups depending on duration: ≤ 60 s or > 60 s. The following characteristics were also evaluated: amplitude ≥ 60 bpm, nadir below 60 bpm, absent variability within decelerations, overshoot (exaggerated elevation of the FHR immediately after the deceleration), slow (>2 min) or incomplete return to baseline, loss of previous shouldering and baseline > 160 bpm or variability < 5 bpm between decelerations.
When decelerations had rapid onset but repeatedly had the timing described above for late decelerations, these were classified as late decelerations.
Combined decelerations were defined as two decelerations identified per contraction, occurring repeatedly with complete or incomplete recovery of the baseline fetal heart rate between the two decelerations (Fig. 1). This is typically a combination of variable and late decelerations [4], [12].Fig. 1. Combined decelerations, defined in study as two decelerations per contraction, occurring repeatedly with complete or incomplete recovery of the fetal heart rate baseline between the two decelerations.Fig. 1
Prolonged decelerations were divided, based on duration, into two groups, 3–5 min or > 5 min. Prolonged decelerations > 5 min were stratified into occurring only during the last 10 min before vaginal birth or occurring (beginning) earlier.
We also evaluated if the FHR, due to decelerations, was below the baseline ≥ 50 % of the time for more than 30 min (Fig. 2). When assessing this, a stable baseline was first identified, then the number of min that the FHR was below this baseline, due to decelerations, and the number of min above or at the baseline were counted.Fig. 2. Examples of CTG with fetal heart rate below the baseline ≥ 50 % of the time, due to decelerations.Fig. 2
All CTG traces were independently scrutinized by two of the authors (MF, AH). When the assessors did not agree regarding the type or number of decelerations, a further assessment was made by a third assessor (CD, FE, GSR). The majority assessment of type and median assessment of number of decelerations was used for the final classification.
The association between each type of deceleration and acidemia at birth was analysed. In a sub-analysis, these associations were determined for traces with normal baseline (110−160) and variability (5–25 bpm).
Statistical analyses
3
Statistical analyses were performed using MedCalc for Windows, version 23.1.7 (MedCalc Software, Ostend, Belgium). Odds ratios (OR) with 95 % confidence intervals were calculated for the association of different fetal heart rate patterns to acidosis. For the categorical comparisons, a chi-square test was used for calculation of statistical significance. Since multiple comparisons were made, only differences with a p-value less than 0.01 were considered statistically significant. Significant associations with OR > 10 was considered strong, OR 5–9 as moderate, and OR below 5 as weak.
Results
4
Of the 1095 studied cardiotocographic recordings, one case was excluded due to registration of maternal pulse instead of the FHR. The corresponding two controls were also excluded, leaving 1092 CTG traces for analysis. A full assessment of 60 min was met by 77 % of CTGs. The mean was 56 min.
Table 2 presents associations between acidemia at birth and decelerations of different characteristics, during (30-) 60 min in the first and second stage of labour. Neither early uniform decelerations nor variable decelerations < 60 s were associated with acidemia.Table 2. Association between acidemia at birth and different types of decelerations in the first and second stage of labour. Figures are presented as numbers (%) and odds ratios with 95 % confidence intervals.Table 21st stage2nd stage1st and 2nd stageAcidemiaN = 70ControlsN = 140OR (95 % CI)p-valueAcidemiaN = 294ControlsN = 588OR (95 % CI)p-valueAcidemia N = 364Controls N = 728OR (95 % CI)p-valueEarly decelerations< 565 (92.9)130 (92.9)Reference293 (99.7)576 (98.0)Reference358 (98.4)706 (97.0)Reference≥ 55 (7.1)10 (7.1)1.0 (0.3–3.0)p = 1.0001 (0.3)12 (2.0)0.2 (0.02–1.3)p = 0.0836 (1.6)22 (3.0)0.5 (0.2–1.3)P = 0.18Late decelerations< 542 (60.0)139 (99.3)Reference193 (65.6)547 (93.0)Reference235 (64.6)686 (94.2)Reference5–915 (21.4)0102 (6.0–1736)p = 0.00147 (16.0)28 (4.8)4.8 (2.9–7.8)p < 0.000162 (17.0)28 (3.8)6.5 (4.0–10)p < 0.0001≥ 1013 (18.6)1 (0.7)43 (5.5–339)p = 0.000454 (18.4)13 (2.2)12 (6.3–22)p < 0.000167 (18.4)14 (1.9)14 (7.7–25)p < 0.0001≥ 528 (40.0)1 (0.7)93 (12–702)p < 0.0001101 (34.4)41 (7.0)7.0 (4.7–10)p < 0.0001129 (35.4)42 (5.8)9.0 (6.1–13)p < 0.0001Repetitive > 20 minNo49 (70.0)140 (100)Reference239 (81.3)578 (98.3)Reference288 (79.1)718 (98.6)ReferenceYes21 (30.0)0122 (7.2–2053)p = 0.000855 (18.7)10 (1.7)13 (6.7–27)p < 0.000176 (20.9)10 (1.4)19 (9.7–37)p < 0.0001Combined decelerations< 559 (84.3)140 (100)Reference240 (81.6)551 (93.7)Reference299 (82.1)691 (94.9)Reference5–99 (12.9)045 (2.6–783)p = 0.00928 (9.5)29 (4.9)2.2 (1.3–3.8)37 (10.2)29 (4.0)2.9 (1.8–4.9)p < 0.0001≥ 102 (2.9)012 (0.6–250)p = 0.1126 (8.8)8 (1.4)7.5 (3.3–17)p < 0.000128 (7.7)8 (1.1)8.1 (3.6–18)p < 0.0001≥ 511 (15.7)054 (3.2–937)p = 0.00654 (18.4)36 (6.1)3.4 (2.2–5.4)p < 0.000165 (17.9)36 (4.9)4.2 (2.7–6.4)p < 0.0001Repetitive > 20 minNo66 (94.3)140 (100)Reference268 (91.2)578 (98.2)Reference334 (91.8)718 (98.6)ReferenceYes4 (5.7)019 (1.01–358)p = 0.04926 (8.8)10 (1.7)5.6 (2.7–12)p < 0.000130 (8.2)10 (1.4)6.4 (3.1–13)p < 0.0001Variable decelerations < 60 s< 551 (72.9)119 (85.0)Reference108 (36.7)170 (28.9)Reference159 (43.7)289 (39.7)Reference5–914 (20.0)15 (10.7)2.2 (1.0–4.8)p = 0.05675 (25.5)190 (32.3)0.6 (0.4–0.9)p = 0.009689 (24.5)205 (28.2)0.8 (0.6–1.1)P = 0.14≥ 105 (7.1)6 (4.3)1.9 (0.6–6.7)p = 0.28111 (37.8)228 (38.8)0.8 (0.6–1.1)p = 0.11116 (31.9)234 (32.1)0.9 (0.7–1.2)P = 0.49≥ 519 (27.1)21 (15.0)2.1 (1.0–4.3)p = 0.036186 (63.3)418 (71.1)0.7 (0.5–0.9)p = 0.018205 (56.3)439 (60.3)0.8 (0.7–1.1)P = 0.21Variable decelerations > 60 s< 563 (90.0)140 (100)Reference189 (64.3)464 (78.9)Reference252 (69.2)604 (83.0)Reference5–96 (8.6)029 (1.6–518)p = 0.02278 (26.5)99 (16.8)1.9 (1.4–2.7)p = 0.000284 (23.0)99 (13.6)2.0 (1.5–2.8)p < 0.0001≥ 101 (1.4)06.6 (0.3–165)p = 0.2527 (9.2)25 (4.3)2.7 (1.5–4.7)p = 0.000828 (7.7)25 (3.4)2.7 (1.5–4.7)p = 0.0003≥ 57 (10.0)033 (1.9–590)p = 0.017105 (35.7)124 (21.1)2.1 (1.5–2.8)p < 0.0001112 (30.8)124 (17.0)2.2 (1.6–2.9)p < 0.0001Repetitive ≥ 30 minNo69 (98.7)140 (100)Reference272 (92.5)560 (95.2)Reference341 (93.7)700 (96.1)ReferenceYes1 (1.4)06.1 (0.2–150)p = 0.2722 (7.5)28 (4.8)1.6 (0.9–2.9)p = 0.1023 (6.3)28 (3.8)1.7 (1.0–3.0)p = 0.0707Prolonged decelerations ≥ 5 min041 (58.6)138 (98.6)Reference185 (62.9)517 (87.9)Reference226 (62.1)655 (90.0)Reference≥ 1 only last 10 min----23 (7.8)46 (7.8)1.4 (0.8–2.4)p = 0.2123 (6.3)46 (6.3)1.4 (0.9–2.4)p = 0.16≥ 1 before last 10 min29 (41.4)2 (1.4)49 (11–213)p < 0.000186 (29.2)25 (4.3)9.6 (6.0–15)p < 0.0001115 (31.6)27 (3.7)12 (7.9–19)p < 0.0001Prolonged decelerations 3–5 min< 368 (97.1)139 (99.3)Reference267 (90.8)583 (99.1)Reference335 (92.0)722 (99.2)Reference≥ 32 (2.9)1 (0.7)4.1 (0.4–46)p = 0.2527 (9.2)5 (0.9)12 (4.5–31)p < 0.000129 (8.0)6 (0.8)10 (4.3–25)p < 0.0001**≥ 50 % below the baseline**No42 (60.0)140 (100)Reference95 (32.3)510 (86.7)Reference137 (37.6)650 (89.3)ReferenceYes28 (40.0)0188 (11–3152)p = 0.0003199 (67.7)78 (13.3)14 (9.7–19)p < 0.0001227 (62.4)78 (10.7)14 (10-19)p < 0.0001
Late decelerations were strongly associated with acidemia; OR 14 (7.7–25) when ten or more were identified, and 19 (9.7–37) if they were repetitive > 20 min.
Variable decelerations > 60 s were weakly associated with acidemia with an OR 2.7 (1.5–4.7) when > 10 were identified. For repetitive variable decelerations no significant association with acidemia was found.
For combined decelerations the association to acidemia was moderate with OR 8.1 (3.6–18) for a count > 10, and OR 6.4 (3.1–13) if they were repetitive for 20 min.
Associations with acidemia were strong for one prolonged deceleration > 5 min (OR 12; 7.9–19), unless occurring last 10 min before birth, and for three or more prolonged decelerations of 3–5 min (OR 10; 4.3–25).
Fetal heart rate below the baseline ≥ 50 % of the time for more than 30 min was strongly associated with acidemia (OR 14; 10–19).
Most deceleration patterns associated with acidemia were considerably less frequent in controls during the first than in the second stage, resulting in higher OR estimates in the first stage. In the first stage only one control had five late decelerations, none had five variable decelerations > 60 s or combined decelerations, and three had prolonged decelerations.
For decelerations associated with acidemia at birth, we performed a sub-analysis including only traces with normal baseline and variability (Table 3). Significant associations to acidemia remained for late decelerations, combined decelerations, variable decelerations > 60 s, prolonged decelerations and FHR 50 % below baseline.Table 3. Association between different type of decelerations and acidemia at birth, in fetal heart rate traces with baseline 110–160 and variability 5–25 bpm.Table 3. Cases with acidemia (%)Controls (%)OR (95 % CI)P-valueN = 204N =661Late decelerations< 5143 (70.1)626 (94.7)reference> 561 (29.9)35 (5.3)7.6 (4.8-12)>0.00015–935 (17.1)24 (3.6)6.4 (3.7–11)<0.0001> 1026 (12.7)11 (1.7)10 (5.0–21)<0.0001Not repetitive > 20 min172 (84.3)651 (98.5)referenceRepetitive > 20 min32 (15.7)10 (1.5)12 (5.8–25)<0.0001Combined decelerations< 5159 (77.9)630 (95.5)reference> 545 (22.1)30 (4.5)5.9 (3.6-9.7)<0.00015–925 (12.3)25 (3.8)4.0 (2.2–7.1)<0.0001> 1020 (9.8)6 (0.9)13 (5.2–33)<0.0001Not repetitive > 20 min182 (89.2)653 (98.8)referenceRepetitive > 20 min22 (10.8)8 (1.2)9.9 (4.3–23)<0.0001Variable decelerations > 60 seconds< 5129 (63.2)551 (83.4)reference> 575 (36.8)110 (16.6)2.9 (2.0–4.1)<0.00015–955 (27.0)90 (13.6)2.6 (1.8–3.8)<0.0001> 1020 (9.8)20 (3.0)4.3 (2.2–8.2)<0.0001Not repetitive > 30 min189 (92.6)639 (96.7)referenceRepetitive > 30 min15 (7.4)22 (3.3)2.3 (1.2–4.5)0.01Prolonged deceleration(s) 3–5min< 3185 (90.7)656 (99.2)reference> 319 (9.3)5 (0.8)13 (5.0–37)<0.0001Prolonged deceleration(s) > 5minNone139 (68.1)599 (90.6)referenceLast 10 min before birth14 (6.9)43 (6.5)1.4 (0.75–2.6)0.29Before last 10 min51 (25.0)19 (2.8)12 (6.6–20)<0.0001Fetal heart rate > 50 % below baseline during > 30minNo79 (38.7)595 (90.0)referenceYes125 (61.3)66 (10.0)14 (9.8–21)<0.0001
For variable decelerations > 60 s, a further analysis was performed comparing those with and without additional potentially concerning characteristics (Table 4). Of the examined characteristics, loss of variability within decelerations was significantly associated with acidemia (OR 5.8; 2.1–16), whereas amplitude > 60 beats, nadir below 60 bpm, failed return to baseline, duration > 2 min (slow return), loss of shouldering, overshoot and baseline > 160 bpm or variability < 5 bpm between the decelerations were not.Table 4. Association between other potentially concerning characteristics of variable decelerations with duration > 60 seconds and acidemia at birth. Only traces with > 5 variable decelerations were included, and each potentially concerning factor had to be present in > 3 decelerations to be accounted for.Table 4Acidemia (%)Controls (%)OR (95 % CI)P-valueN = 112N = 124Amplitude > 60 bpmNo41 (36.6)54 (43.5)referenceYes71 (63.4)70 (56.5)1.3 (0.79–2.3)0.28Nadir at < 60 bpmNo96 (85.7)104 (83.9)referenceYes16 (14.3)20 (16.1)0.87 (0.42–1.8)0.69Slow or failed return to baselineNo74 (66.1)90 (72.6)referenceYes38 (33.9)34 (27.4)1.4 (0.78–2.4)0.28Loss of previously present shoulderingNo111 (99.1)120 (96.8)referenceYes1 (0.8)4 (3.2)0.27 (0.03–2.5)0.25Absent variability within decelerationsNo90 (80.4)119 (96.0)referenceYes22 (19.6)5 (4.0)5.8 (2.1–16)0.0006OvershootNo110 (98.2)123 (99.2)referenceYes2 (1.8)1 (0.8)2.2 (0.20–25)0.51Baseline > 160 between decelerationsNo98 (87.5)117 (94.4)referenceYes14 (12.5)7 (5.6)2.4 (0.93–6.2)0.07Variability < 5 between decelerationsNo106 (94.6)119 (96.0)referenceYes6 (5.4)5 (4.0)1.3 (0.40–4.5)0.63
For NICE-22 concerning criteria for variable decelerations, we found a significant association for both amber, OR 2.3 (1.5–3.3) and red criteria, OR 3.9 (2.5–5.9) patterns and acidemia at birth (Table 5). For SWE17 we found a significant association for variable decelerations > 60 s with concomitant tachycardia or reduced variability, OR 3.3 (1.5–7.5).Table 5. The associations between amber/suspicious and red/pathological criteria for variable declarations according to NICE −22 and SWE-17 and acidemia at birth.Table 5Acidemia (%)Controls (%)OR (95 % CI)P-valueN = 364N = 728Variable decelerations with concerning characteristics (NICE−22)No244 (67.0)622 (85.4)referenceRepetitive < 30 min or non-repetitive > 30 min58 (16.0)65 (9.0)2.3 (1.5–3.3)<0.0001Repetitive > 30 min62 (17.0)41 (5.6)3.9 (2.5–5.9)<0.0001Repetitive variable decelerations > 60 sNo332 (91.2)695 (95.5)referenceYes, with normal baseline and variability16 (4.4)23 (3.1)1.5 (0.76–2.8)0.26Yes, with baseline > 160 bpm or variability < 5 bpm16 (4.4)10 (1.4)3.3 (1.5–7.5)0.003
Discussion
5
Since acidemia at birth is a relatively rare event, the positive predictive value of any indicator will be low unless the OR is very high. Therefore, only markers with an OR about 5 or more may have a sufficiently strong association to acidemia by itself to be considered as a ´pathological´ sign, indicating intervention.
This study showed that late, combined, and prolonged decelerations were strongly or moderately associated with acidemia at birth. This is consistent with previous studies [13], [14], [15]. We could also evaluate how the total number of decelerations during one hour of recording, and repetitivity influenced the risk of acidemia. As expected, the OR for acidemia increased with increasing number of decelerations. For late and combined decelerations, we also saw OR for repetitive decelerations that corresponded to OR for a higher number of decelerations. For variable decelerations > 60 s, no association between repetitive decelerations and acidemia was found, while a frequency of 10 or more showed a weak association with acidemia. Since the confidence intervals for these comparisons overlapped, this difference is probably coincidental. Moreover, we found a strong association between > 50 % total duration of decelerations for 30 min and acidemia at birth.
Previous studies have shown varying results regarding variable decelerations. Low et al. found that variable and early decelerations were not associated to asphyxia when the last 4 hours before birth was examined [14]. Holzmann et al. found that variable decelerations > 60 s increased the risk of elevated fetal scalp blood lactate, particularly in combination with tachycardia [13]. We found a weak relationship between variable decelerations > 60 s and acidemia, that remained also among traces with normal baseline and variability.
Since the NICE guidelines assess the risk of hypoxia in case of variable decelerations based on several different concerning characteristics [2], we performed a subanalysis of these and other characteristics for variable decelerations > 60 s. Only one characteristic, absent variability within the decelerations, showed a significant association to acidemia with OR 5.8 compared to those with variable decelerations > 60 s without this characteristic. Given the small number of recordings with decelerations with overshoot, loss of shouldering, absent variability within the deceleration and baseline > 160 bpm or variability < 5 bpm between the decelerations, these estimated ORs should be interpreted cautiously. Cahill et al. investigated the association between shoulders, overshoots, slow returns and variability in variable decelerations and did not find any association with metabolic acidemia [16]. Hamilton et al. reported an association to acidemia for variable decelerations with prolonged duration > 120 seconds, loss of internal variability or with two “sixties” criteria present: depth > 60 bpm or more, nadir < 60 bpm, or duration > 60 s or longer [17]. Martí Gamboa et al. reported an increased risk of acidemia for variable decelerations with "slow return" or loss of moderate variability within decelerations [18].
We considered it of interest to evaluate the association of NICE-22 and SWE-17 criteria for the assessment of variable decelerations as suspicious or pathological and acidemia at birth. Repetitive variable decelerations with any concerning characteristics (NICE-22) showed only a weak association with acidemia both for durations over and under 30 min. Variable decelerations > 60 s with baseline > 160 bpm or variability < 5 bpm (pathological in SWE-17) were also weakly associated with acidemia.
The criterion “50 % below baseline during 30 min” was associated with a high OR for acidemia without considering of the type of decelerations behind. None of current guidelines include this as a suspicious or pathological pattern. Considering our result, and previous studies [19], [20], this criterion might be useful when evaluating CTG in labour.
In the first stage of labour, late, combined, prolonged decelerations > 5 min, and variable decelerations > 60 s were rarely seen in controls and strongly associated with acidemia. This finding may indicate that the threshold for intervention should be lower in the first stage of labour, and that the only decelerations that should be accepted as a normal pattern in the first stage are early uniform decelerations and variable decelerations < 60 s.
To our knowledge, this study is the first to assess the associations between acidemia at birth and characteristics and numbers of different deceleration in such detail in a material including a relatively large number of traces from neonates with acidemia. Limitations are that the size of the material does not allow firm conclusions about fetal heart rate patterns that are infrequent also in cases with acidemia and that only the last hour of CTG recordings were analysed. A scientific limit, but ethical prerequisite, is that, like most studies of CTG, we did not study the natural course for fetuses with different heart rate patterns; interventions had been undertaken when patterns were recognized as pathological.
We consider that the results of the present study may be useful in endeavors to increase the diagnostic precision of CTG interpretation templates.
Conclusion
6
Intrapartum fetal heart rate patterns with repetitive late or combined decelerations, three or more 3–5 min prolonged decelerations or one deceleration prolonged for > 5 min entail a strongly increased risk for acidemia at birth. An equally elevated risk exists if the fetal heart rate is below the baseline more than 50 % of the time for 30 min. This variable may be valuable to include when assessing CTG during labour.
Ethical approval
Ethical approval was obtained from the Regional Ethical Review Board in Lund, Dnr 2016/371, 24 May 2016.
Funding
The study is part of a project supported by research grants from the Public Health Care Region Skåne and LÖF, the Swedish Patient Insurance Company.
CRediT authorship contribution statement
Fogelberg Maria: Writing – original draft, Visualization, Methodology, Investigation, Formal analysis. Dahlbäck Charlotte: Writing – review & editing, Investigation. Ekengård Frida: Writing – review & editing, Resources, Investigation. Rickle Gisela: Writing – review & editing, Investigation. Herbst Andreas: Writing – review & editing, Visualization, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Conceptualization.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ayres-de-Campos D.Spong C.Y.Chandraharan E.FIGO consensus guidelines on intrapartum fetal monitoring: cardiotocography Int J Gynaecol Obstet 1311201513242643340110.1016/j.ijgo.2015.06.020 · doi ↗ · pubmed ↗
- 2〈www.nice.org.uk/guidance/ng 229〉. Fetal monitoring in labour 2022.
- 3American College of O, Gynecologists. Practice bulletin no. 116: Management of intrapartum fetal heart rate tracings. Obstet Gynecol. 2010;116(5):1232-1240.10.1097/AOG.0b 013e 3182004 fa 920966730 · doi ↗ · pubmed ↗
- 4Santo S.Ayres-de-Campos D.Costa-Santos C.Schnettler W.Ugwumadu A.Da Graca L.M.Agreement and accuracy using the FIGO, ACOG and NICE cardiotocography interpretation guidelines Acta Obstet Gynecol Scand 9622017166175(Collaboration FM-C.)2786998510.1111/aogs.13064 · doi ↗ · pubmed ↗
- 5Zamora Del Pozo C.Chóliz Ezquerro M.Mejía I.Díaz de Terán Martínez-Berganza E.Esteban L.M.Rivero Alonso A.Diagnostic capacity and interobserver variability in FIGO, ACOG, NICE and Chandraharan cardiotocographic guidelines to predict neonatal acidemia J Matern Fetal Neonatal Med 35252022849885063465224910.1080/14767058.2021.1986479 · doi ↗ · pubmed ↗
- 6Ekengard F.Cardell M.Herbst A.Impaired validity of the new FIGO and Swedish CTG classification templates to identify fetal acidosis in the first stage of labor J Matern Fetal Neonatal Med 35252022485348603340694610.1080/14767058.2020.1869931 · doi ↗ · pubmed ↗
- 7Ekengard F.Cardell M.Herbst A.Low sensitivity of the new FIGO classification system for electronic fetal monitoring to identify fetal acidosis in the second stage of labor Eur J Obstet Gynecol Reprod Biol X 9202110012010.1016/j.eurox.2020.100120 PMC 772415933319210 · doi ↗ · pubmed ↗
- 8Yoon B.H.Kim S.W.The effect of labor on the normal values of umbilical blood acid-base status Acta Obstet Gynecol Scand 7371994555561807960610.3109/00016349409006272 · doi ↗ · pubmed ↗