Facial follicular porokeratosis simulating discoid lupus erythematosus in an African American woman
Pritika Singh, Layna Mager, Jeffrey Y. Liu, Jason B. Lee, Sylvia Hsu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
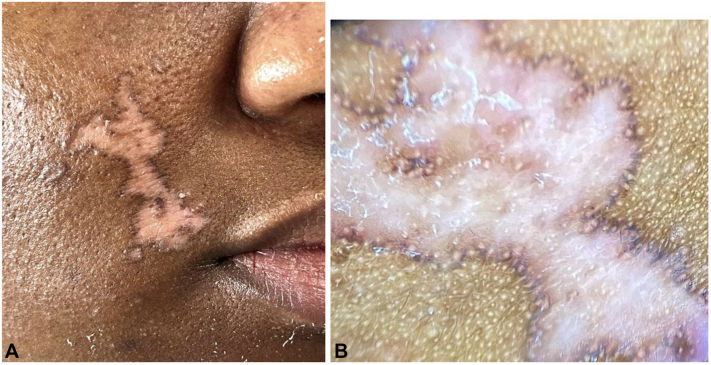 Figure 1
Figure 1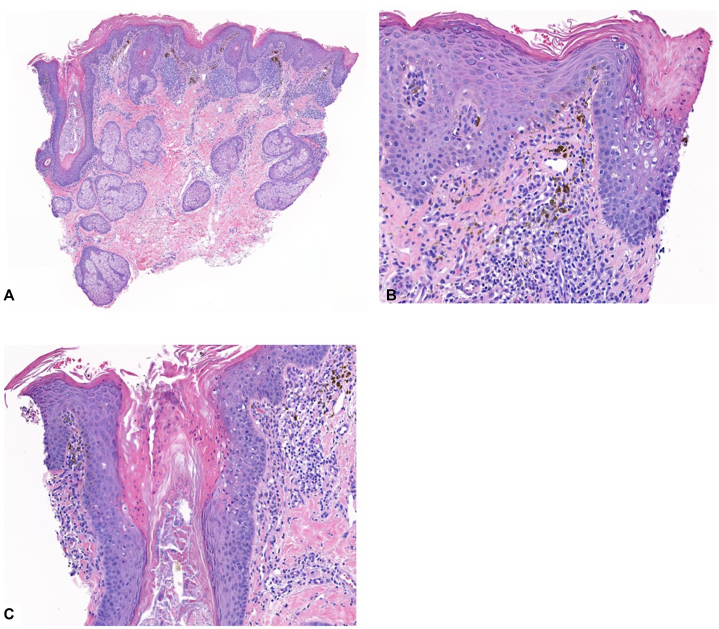 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetic and rare skin diseases. · Dermatologic Treatments and Research
Introduction
Porokeratosis is a disorder of abnormal keratinization that often presents with keratotic papules to annular plaques with elevated borders. The lesions typically occur on sun-exposed skin with most presenting in the fifth decade of life but can occur at any age.1 Lesions are most often distributed on the extremities and trunk. Though facial involvement can be seen in up to 15% of patients with disseminated superficial actinic porokeratosis, single, solitary lesions are rare.2, 3, 4 Follicular involvement of porokeratosis is infrequently seen, though it has been reported in cases of various variants of porokeratosis.5, 6, 7, 8, 9 In this report, we highlight a case of a single, solitary, atrophic lesion on the face of a 32-year-old African American female patient that was previously diagnosed and treated as discoid lupus erythematosus (DLE) with histology showing cornoid lamella within the follicle.
Case presentation
An African American woman in her 30s with no significant past medical history presented to our outpatient clinic with concern for a lesion on her right cheek. The patient reports that the lesion was present for 5 years with no associated symptoms. This lesion was previously diagnosed as DLE by a rheumatologist and was started on hydroxychloroquine at that time. Serology was negative for antinuclear, antidouble-stranded DNA, anticentromere, anti-Smith/ribonucleoproteins, anti-Sjogren antibodies anti-Sjögren's syndrome A (Ro) and anti-Sjögren's syndrome B (La) antibodies, anti-Jo1, anticardiolipin, and antibeta-2 glycoprotein 1 antibodies. Complement levels were normal. She was referred to dermatology for further management. On clinical examination, the patient presented with an atrophic patch with central hypopigmentation and a brown raised border on the right medial cheek (Fig 1, A and B).Fig 1A, Atrophic patch with central hypopigmentation and a brown raised border on the right medial cheek. B, Same patch under 4× magnification.
A 3-mm punch biopsy of the raised border showed moderately dense superficial perivascular lymphocytes and melanophages without active vacuolar interface changes of the epidermis and infundibula (Fig 2, A). In 2 of the 4 follicles, multiple dyskeratotic cells were seen within the infundibula. In the other 2, there were characteristic histopathologic changes of follicular porokeratosis: a column of parakeratosis with dyskeratotic cells surrounded by vacuolated and pale epithelial cells (Fig 2, B and C). With the histopathologic findings, the patient was given the diagnosis of porokeratosis and advised to discontinue hydroxychloroquine. The patient was subsequently treated with 2% topical lovastatin twice daily in the affected area, with a planned follow-up 3 months after the visit.Fig 2A, Moderately dense superficial perivascular lymphocytes and melanophages without active vacuolar interface changes of the epidermis and infundibula. B and C, In 2 of the 4 follicles, multiple dyskeratotic cells were seen within the infundibula. In the other 2, there were characteristic histopathologic changes of follicular porokeratosis: a column of parakeratosis with dyskeratotic cells surrounded by vacuolated and pale epithelial cells.
Discussion
Porokeratosis often presents as keratotic papules or annular plaques that expand centrifugally with an elevated keratotic border. Centrally, the lesion can appear slightly atrophic with raised borders. Lesions are more frequently distributed to photo-exposed areas, including the extremities, trunk, and face. The etiology and pathology of porokeratosis is unclear. UV light exposure, as well as repeated frictional trauma, has been suggested.1 There are multiple clinical variants of porokeratosis that can look clinically distinct from one another, but all share the classic histological finding of cornoid lamella, a column of compact parakeratosis with a focal absence of the granular layer, and the concomitant presence of dyskeratotic cells.2^,^10
Follicular porokeratosis is suggested to be a histopathological variant of porokeratosis with cornoid lamella restricted to follicles.4^,^5 Clinically, follicular porokeratosis can present with isolated facial involvement. DLE can have a similar clinical presentation with most lesions also localized to the face, ears, and scalp. Lesions of DLE may also exhibit a photodistribution, as sun exposure may also play a role in the development of lesions.6 DLE lesions appear as well-defined, annular erythematous patches or plaques of varying sizes followed by follicular hyperkeratosis. These lesions slowly expand with active inflammation and hyperpigmentation at the periphery, leaving depressed central atrophy, scarring, telangiectasia, and hypopigmentation, which can simulate the atrophic lesions of porokeratosis on the face.7^,^8
Histopathologic findings can also be similar in both entities, as follicular porokeratosis can simulate follicular plugging seen in DLE. The latter consists of compact orthokeratosis that can lead to columns of parakeratosis if the interface dermatitis is brisk around the infundibulum. These findings are indistinguishable from cornoid lamella in follicular porokeratosis.8 However, follicular porokeratosis usually lacks vacuolar interface changes involving the infundibulum. Another distinguishing histopathologic finding of porokeratosis is the presence of vacuolated or pale infundibular epithelial cells, which were observed in our case.9 Of the few cases reported, one was reported in a White patient that was initially treated for DLE with hydroxychloroquine.7 Only one other case was reported in an African American patient.8
Without medical or surgical intervention, porokeratosis will remain indefinitely. Spontaneous regression of these lesions is extremely rare. Treatments with variable results have been used for porokeratosis, including topical 5-fluorouracil, keratolytics, retinoids, vitamin D-3 analogs, and excision. There are no international guidelines on treatment standards. However, marginal improvements in lesion size have been reported with the use of topical lovastatin.1
Conclusions
Our case presents a rare clinical subtype of porokeratosis with follicular involvement on the face of an African American woman. This entity simulates DLE and is rarely reported in skin of color patients. Taken together, it is important for dermatologists to recognize this presentation to avoid misdiagnosis and unnecessary treatment. Histopathological evaluation is necessary to establish a definitive diagnosis.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sertznig P.von Felbert V.Megahed M.Porokeratosis: present concepts J Eur Acad Dermatol Venereol 26420124044122192954810.1111/j.1468-3083.2011.04275.x · doi ↗ · pubmed ↗
- 2Pietkiewicz P.Korecka K.Salwowska N.Porokeratoses—a comprehensive review on the genetics and metabolomics, imaging methods and management of common clinical variants Metabolites 13122023117610.3390/metabo 1312117638132857 PMC 10744643 · doi ↗ · pubmed ↗
- 3Paolino G.Nicola M.R.Yarygina M.Exclusive and solitary facial porokeratosis: pathogenesis and literature reappraisal of a rare entity Case Rep Dermatol 151202314715110.1159/00053093637899946 PMC 10601618 · doi ↗ · pubmed ↗
- 4Tallon B.Emanuel P.Follicular porokeratosis, a porokeratosis variant Am J Dermatopathol 3982017 e 107e 10910.1097/DAD.000000000000085028266938 · doi ↗ · pubmed ↗
- 5Keller L.P.Halim K.Abedi S.M.Liu W.Gottesman S.P.Cluster of vacuolated spinous keratinocytes: a clue to cornoid lamellation and a case of porokeratosis disseminata Am J Dermatopathol 429202067367610.1097/DAD.000000000000161432000214 · doi ↗ · pubmed ↗
- 6Kuhn A.Ruland V.Bonsmann G.Photosensitivity, phototesting, and photoprotection in cutaneous lupus erythematosus Lupus 19920101036104610.1177/096120331037034420693197 · doi ↗ · pubmed ↗
- 7Pongpudpunth M.Farber J.Mahalingam M.Follicular porokeratosis: distinct clinical entity or histologic variant?J Cutan Pathol 361120091195119910.1111/j.1600-0560.2009.01266.x 19519877 · doi ↗ · pubmed ↗
- 8Bembry R.Louie E.Overholser E.Tirado M.Exclusive facial porokeratosis with follicular involvement in an African American female J Cutan Pathol 505202338338410.1111/cup.1442436928597 · doi ↗ · pubmed ↗