A mature T-cell neoplasm with features of peripheral T-cell lymphoma, not otherwise specified presenting with multiple cutaneous tumors on the scalp in a patient with long-standing lichen planopilaris
Brittani A. Jones, Wesley T. Hodges, Mahta Salehi, Georgeanne Cornell, Sagun Goyal, John L. Frater, M. Yadira Hurley

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1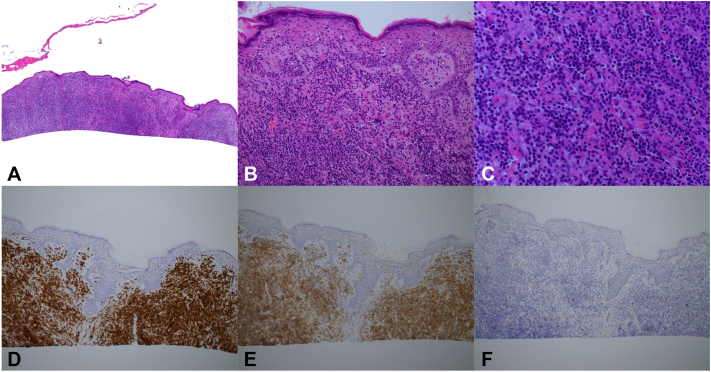 Figure 2
Figure 2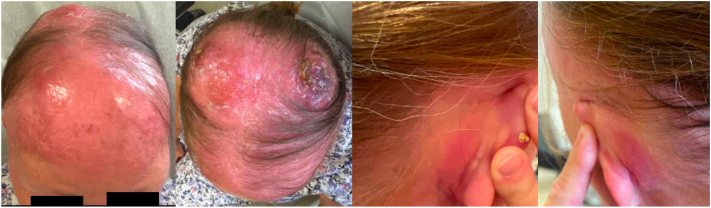 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Lymphoma Diagnosis and Treatment · Nail Diseases and Treatments
Introduction
Mature T-cell neoplasms (MTCNs) are diverse, with highly variable clinical presentation, natural history, and outcomes.1 Peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS) is the most commonly seen subtype, comprising ∼25% of mature T-cell neoplasms and ∼10 to 12% of all lymphoid malignancies, and is encountered in lymph nodes and extranodal sites, including the skin.2^,^3
Lymphocytic infiltration of the skin can also be seen in benign inflammatory conditions. Lichen planopilaris (LPP), considered a variant of lichen planus, is a scarring alopecia characterized histologically by dense perifollicular infiltration of lymphocytes along the upper third of the hair follicle. LPP has been associated with other inflammatory conditions such as autoimmune thyroid diseases,4 but to the best of our knowledge, no association has been established between LPP and the development of leukemias/lymphomas. Herein, we report a case of MTCN with features of PTCL-NOS presenting with multiple cutaneous tumors in a patient with long-standing LPP.
Case
A 70-year-old White woman with a past medical history notable for severe LPP treated with hydroxychloroquine for 10 years was referred to our dermatology and combined dermatology/oncology clinics for rapidly enlarging scalp nodules. At the time of evaluation, she had bilateral parietal and frontal scalp tumors (Fig 1) that evolved from a singular lesion 3 months prior. She likewise reported progressive hair loss and tenderness during this time. The tumors and associated symptoms were only minimally responsive to treatment with clobetasol and a concomitant prednisone taper.Fig 1. Cutaneous tumors of the scalp with diffuse thickening and erythema of the scalp.
Biopsies of the bilateral vertex scalp revealed a striking superficial and deep dermal subcutaneous infiltrate of small to medium-sized lymphoid cells arranged in sheets. The lymphoid cells demonstrated minimal eosinophilic cytoplasm, regular nuclear contours, and inconspicuous nucleoli. Only rare lymphocytes were seen at the dermal-epidermal junction and the hair follicles were spared. The atypical lymphoid infiltrate was characterized by CD3, CD4, CD5, and TCRBetaF1 positivity, as well as CD30, CD10, CD56, CD123, and TCRDelta negativity. EBER in situ hybridization and PD1 were negative. The CD4:CD8 ratio was 20:1. T cell receptor beta and gamma gene rearrangements were also positive and showed the same clone at 2 separate sites (Fig 2). Of note, the tissue block and slides from the patient’s historical diagnostic LPP biopsy were no longer available for comparative analysis.Fig 2. Representative histology images from shave biopsies of the rapidly enlarging scalp tumors of the vertex scalp shown in Fig 1. Shown are hematoxylin and eosin (H&E) stained slides at 40× (A), 200× (B), and 400× (C) magnification, respectively. A superficial and deep dermal subcutaneous infiltrate of lymphoid cells are appreciable with rare involvement at the dermal-epidermal junction and sparing of the hair follicles. CD3 (D), CD4 (E), and CD8 (F) stains are also shown and demonstrate strong CD3 and CD4 positivity of the lymphoid infiltrate with a CD4:CD8 ratio of approximately 20:1.
A complete workup was conducted to assess extracutaneous involvement and rule out systemic lymphoma. Laboratory workup was notable for a mild stable normocytic anemia, normal metabolic panel, and normal lactate dehydrogenase. Uric acid was mildy elevated at 7.1 mg/dL. Human T-cell lymphotropic virus type 1, HIV, and hepatitis panels were all negative. Peripheral blood flow cytometry demonstrated an aberrant CD4+ T-cell population which compromised 5.3% of the total population. PET-CT was notable for fluorodeoxyglucose avidity of the bilateral parietal scalp but showed no evidence of lymph node or other organ involvement. Bone marrow biopsy demonstrated a hypercellular core with maturing trilineage hematopoiesis and involvement of a peripheral T-cell lymphoma representing 50% to 60% of the marrow cellularity. Fluorescence in-situ hybridization analysis revealed a MYC gain-of-function mutation. Clinicopathologic correlation led to a diagnosis of MTCN.
The patient’s scalp lesions continued to rapidly worsen, and she developed diffuse thickening of the entire scalp (Fig 3) prompting urgent initiation of chemotherapy. She was started on cyclophosphamide, hydroxydanorubicin, oncovin, and prednisone (CHOP) chemotherapy regimen (cyclophosphamide, doxorubicin, vincristine, and prednisone) with a goal of 6 cycles total. Prophylactic care with granulocyte colony-stimulating factor (Neulasta) and valacyclovir was also initiated. The patient responded rapidly to CHOP therapy with significant decreases in tumor size and healing with black/brown crust after the first 2 treatment cycles (Fig 4). Of note, the patient’s medical course was complicated by eyelid pruritis and edema, neutropenic fever and port infection, axillary nodules, and septic shock secondary to Pseudomonas bacteremia due to ecthyma gangrenosum arising from infected scalp tumors. Following the multiple infections, she was started on prophylactic levofloxacin and her chemotherapy dose was temporarily reduced by 25%. The patient will continue with CHOP therapy and future consolidative autologous stem cell transplant is being considered.Fig 3. New tumor development with worsening erythema and enlarged pre-existing nodules at follow-up appointment 20 days from initial.Fig 4. Image of lesional improvement following initiation of chemotherapy with CHOP.
Discussion
To the best of our knowledge, there are no previously reported cases of concurrent MTCN and LPP. Based on the pathologic features, this lymphoma is best classified as PTCL-NOS. The current (2024) World Health Organization classification of hematolymphoid tumors recognizes 2 categories of PTCL-NOS: nodal and primary cutaneous.5 Primary cutaneous PTCL-NOS is rare and appears to have an aggressive clinical course similar to its nodal counterpart.6^,^7 The distribution of lymphoma in this patient, with involvement of the skin and bone marrow and lack of nodal disease, is unusual, and would not be typical of either nodal or primary cutaneous PTCL-NOS.
The striking accumulation of malignant lymphocytes localized at the site of the patient’s long-standing LPP is notable, and because of this feature we propose that this patient’s lymphoma is likely related to her previously diagnosed LPP. Many lymphoma types appear to be associated with concurrent inflammation. These include the following:
- -Lymphomas associated with chronic infection. The most conclusively proved link between chronic infection and lymphoma is the association of gastric marginal zone lymphoma with Helicobacter pylori infection, although infection by Chlamydia psittaci, Borrelia burgdorferi, and Campylobacter jejuni have also been proposed as inciting agents in other lymphoma types.8
- -Lymphomas such as classic Hodgkin lymphoma and anaplastic large cell lymphoma, in which the malignant cells are often present in an inflammatory cell antitumoral milieu.9
- -Differing lymphoma types arising in patients with chronic inflammatory/autoimmune disorders such as rheumatoid arthritis and inflammatory bowel disease.10
Because of its aggressive clinical behavior, anthracycline-based chemotherapy regimens are the standard of care for PTCL-NOS.7 For better outcomes, most experts recommend adding etoposide (cyclophosphamide, hydroxydanorubicin, oncovin, etopside, and prednisone) for patients who are medically fit and younger than 60 years old. Our patient responded rapidly to CHOP, though complete clinical resolution of the patient’s tumors has not been achieved following 2 cycles. Many patients with PTCL-NOS may require autologous stem cell transplants, especially in refractory or relapsed disease.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bigas A.Rodriguez-Sevilla J.J.Espinosa L.Gallardo F.Recent advances in T-cell lymphoid neoplasms Exp Hematol 10620223183487925810.1016/j.exphem.2021.12.191 · doi ↗ · pubmed ↗
- 2Pileri S.A.Tabanelli V.Fiori S.Peripheral T-cell lymphoma, not otherwise specified: clinical manifestations, diagnosis, and future treatment Cancers (Basel)13202145353457276310.3390/cancers 13184535 PMC 8472517 · doi ↗ · pubmed ↗
- 3Horwitz S.M.Ansell S.Ai W.Z.T-cell lymphomas, version 2.2022, NCCN clinical practice guidelines in oncology J Natl Compr Canc Netw 2020222853083527667410.6004/jnccn.2022.0015 · doi ↗ · pubmed ↗
- 4Brankov N.Conic R.Z.Atanaskova-Mesinkovska N.Piliang M.Bergfeld W.F.Comorbid conditions in lichen planopilaris: a retrospective data analysis of 334 patients Int J Womens Dermatol 420181801843017522410.1016/j.ijwd.2018.04.001PMC 6116820 · doi ↗ · pubmed ↗
- 5WHO Classification of Haematolymphoid Tumours 5th ed.2024 IARC Press 708709
- 6Pileri A.Agostinelli C.Fuligni F.Primary cutaneous peripheral T-cell lymphoma not otherwise specified a rare and aggressive lymphoma J Eur Acad Dermatol Venereol 322018 e 373e 3762957347710.1111/jdv.14942 · doi ↗ · pubmed ↗
- 7Kempf W.Mitteldorf C.Battistella M.Primary cutaneous peripheral T-cell lymphoma, not otherwise specified: results of a multicentre European Organization for Research and Treatment of Cancer (EORTC) cutaneous lymphoma taskforce study on the clinico-pathological and prognostic features J Eur Acad Dermatol Venereol 3520216586683299783910.1111/jdv.16969 · doi ↗ · pubmed ↗
- 8Vannata B.Pirosa M.C.Bertoni F.Rossi D.Zucca E.Bacterial infection-driven lymphomagenesis Curr Opin Oncol 3420224544633588046310.1097/CCO.0000000000000886 · doi ↗ · pubmed ↗