Antibody Responses to SARS-CoV-2 among Health Care Workers in North-Eastern Tanzania
Pendo Ibrahim, Felix Anthony, Happiness Mshana, Never Zekeya, Hadija Semvua, Jaffu Chilongola

TL;DR
This study found that most healthcare workers in Tanzania had SARS-CoV-2 antibodies, suggesting high exposure to the virus despite low vaccination rates.
Contribution
The study provides new data on SARS-CoV-2 antibody prevalence among healthcare workers in a low-vaccination setting in Africa.
Findings
99.6% of healthcare workers had positive SARS-CoV-2 IgG antibodies, with 64.5% showing strong seropositivity.
Factors like cadre, sex, and hand hygiene practices significantly influenced antibody concentrations.
Only 37.9% of participants reported being vaccinated against COVID-19.
Abstract
Health Care Workers (HCWs) have been playing crucial role in treating patient with COVID-19. They have a higher occupational risk of contracting the disease than the general population, and a greater chance of them transmitting the disease to vulnerable patients under their care. Given the scarcity of HCWs and low COVID-19 vaccine acceptance in Africa, it is essential that HCWs are seroprotected and their exposure to COVID-19 minimized Objective: To determine IgG antibody response to SARS-CoV-2 among HCWs of a tertiary hospital in North Eastern, Tanzania. This cross-sectional study was carried out among 273 HCWs at Kilimanjaro Christian Medical Centre (KCMC), a tertiary, zonal referral hospital in Tanzania’s North Eastern region. Stratified sampling was used to select study participants. Data were obtained from each consenting participant using a validated questionnaire. Blood samples…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
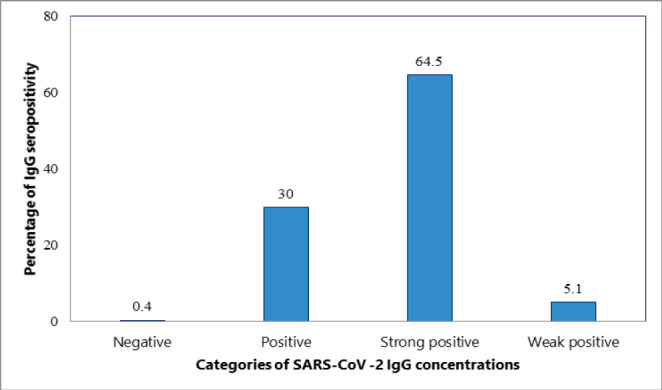 Figure 1
Figure 1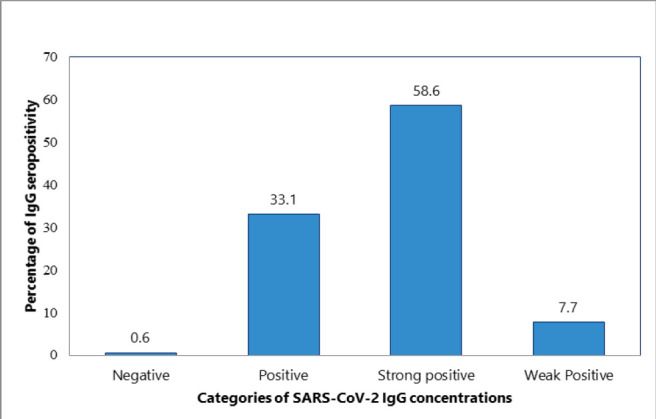 Figure 2
Figure 2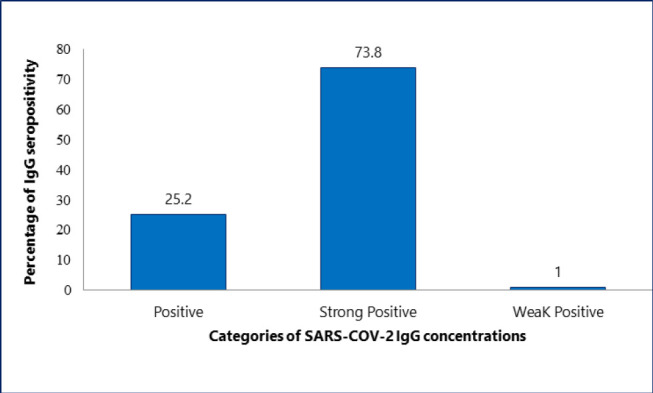 Figure 3
Figure 3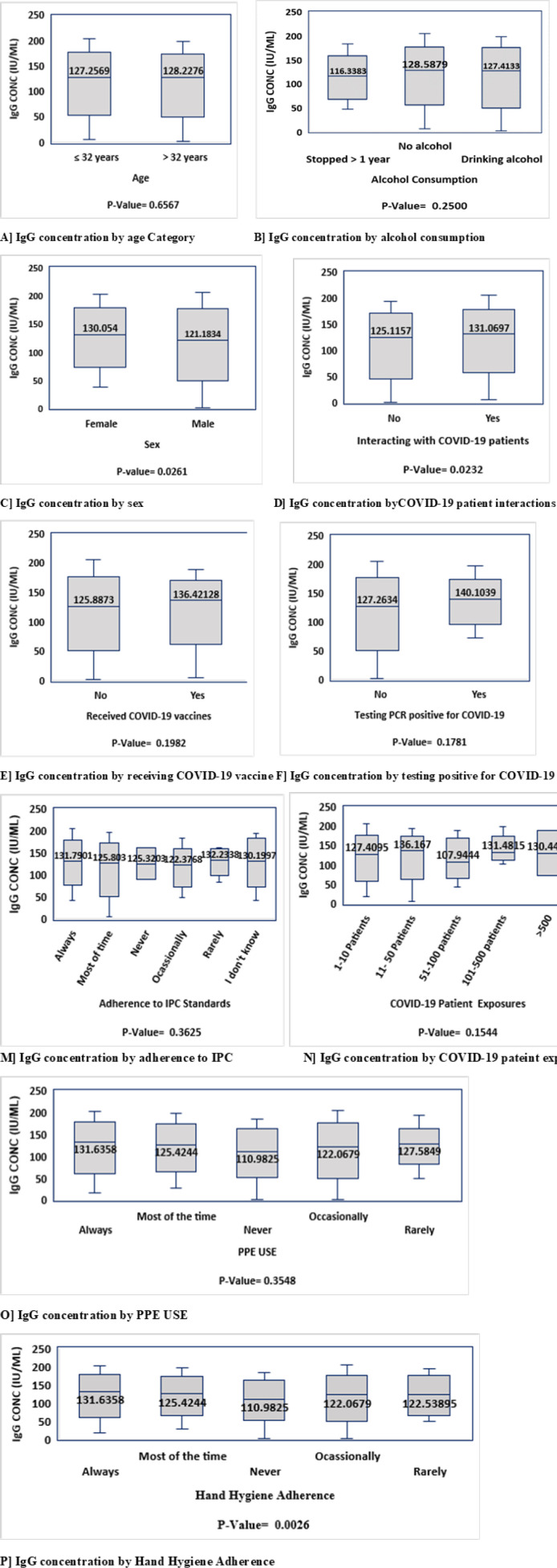 Figure 4
Figure 4| Variable | Frequency | Percentage |
|---|---|---|
| Sex | ||
| Male | 165 | 60.4 |
| Female | 108 | 39.6 |
| Age (in Years) | ||
| ≤ 32 years | 142 | 52.2 |
| > 32 | 130 | 47.8 |
| Median (IQR) | 32 (26-44) | |
| Cadre | ||
| Medical doctor | 78 | 29.0 |
| Nurse | 109 | 40.5 |
| Allied health professionals | 58 | 21.6 |
| Support staff | 23 | 8.9 |
| BMI | ||
| Underweight | 6 | 2.3 |
| Normal | 109 | 40.8 |
| Overweight | 83 | 31.1 |
| Obesity | 69 | 25.8 |
| Median (IQR) | 26.4 (22.8–30.1 | |
| Smoking status | ||
| Stopped >1 year ago | 8 | 2.9 |
| Never smoked | 257 | 94.1 |
| Currently smoke | 8 | 3.0 |
| Alcohol consumption | ||
| Stopped >1 year aeo | 17 | 6.2 |
| Never took alcohol | 158 | 57.8 |
| Currently take alcohol | 98 | 36.0 |
| Taking regular medication | ||
| No | 233 | 85.3 |
| Yes | 40 | 14.7 |
| Tested PCR Positive for COVID-19 | ||
| No | 248 | 91.2 |
| Yes | 24 | 8.8 |
| Received COVID-19 vaccine*(n=272) | ||
| No | 169 | 62.1 |
| Yes | 103 | 37.9 |
| Variable | Frequency | Percentage |
|---|---|---|
| Household size | ||
| 1–2 people | 90 | 33.1 |
| 3–5 people | 136 | 50.0 |
| 6–8 people | 37 | 13.6 |
| 9+ | 9 | 3.3 |
| Public transport | ||
| None | 75 | 27.5 |
| 1–2 people | 68 | 24.9 |
| 3–5 people | 19 | 7.0 |
| 6–8 people | 3 | 1.1 |
| 9+ | 108 | 39.5 |
| Stayed at least 2 meters from other people in indoor space | ||
| Always | 42 | 15.4 |
| Did not go indoor location | 31 | 11.4 |
| Never | 31 | 11.4 |
| Often | 28 | 10.2 |
| Rarely | 56 | 20.5 |
| Sometimes | 85 | 31.1 |
| Hand hygiene practice | ||
| Always as recommended | 150 | 56.6 |
| Most of the time | 104 | 39.3 |
| Never | 3 | 1.1 |
| Occasionally | 8 | 3.0 |
| IPC standards | ||
| Always | 100 | 38.9 |
| I don't know what IPC standard-precaution means | 22 | 8.6 |
| Most of the time | 97 | 37.7 |
| Never | 2 | 0.8 |
| Occasionally | 28 | 10.9 |
| Rarely | 8 | 3.1 |
| Wearing PPE as recommended | ||
| Always | 112 | 42.4 |
| Most of the time | 102 | 38.6 |
| Never | 8 | 3.1 |
| Occasionally | 33 | 12.5 |
| Rarely | 9 | 3.4 |
| Interactions with COVID–19 Patients | ||
| No | 110 | 41.7 |
| Yes | 154 | 58.3 |
| Exposure to COVID–19 Patients | ||
| 1–10 Patients | 169 | 68.4 |
| 11–50 | 41 | 16.6 |
| 51–100 | 18 | 7.3 |
| 101–500 | 17 | 6.9 |
| > 500 | 2 | 0.8 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research
BACKGROUND
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is the virus responsible for causing COVID-19.^1,2^ Since its emergence in December 2019 in Wuhan China, COVID-19 has posed significant global threat, resulting in numerous deaths, economic disabilities, and social disruptions.^3–5^ COVID-19 primarily affects the respiratory system, with potential to impact other organ systems beyond the lungs.^1,6^ It was initially discovered in Wuhan, China, on December 2019.^2^ In Tanzania, the first case of COVID-19 was reported in March 2020, indicating the virus’s rapid global spread and its impact.^7^
Personnel on the front lines of treating COVID-19 patients, faced a higher occupational risk of contracting the disease than the general population. According to WHO estimates, COVID-19 resulted in approximately 115,500 deaths of healthcare workers (HCWs) worldwide.^8^ To protect this vulnerable group, WHO implemented several initiatives, including making COVID-19 vaccination a priority for HCWs.^9,10^ Nevertheless, Africa has a considerable scarcity of healthcare personnel to fulfil population demand.^11^ In Tanzania, between 0.4 and 1 HCW is available for every 1000 people.^12,13^ Despite WHO efforts, the majority of HCWs in Africa have low COVID-19 vaccine acceptance because of concerns regarding the side effects of the vaccines, safety, efficacy, short duration of the clinical trials, limited information, and social trust.^14^
Immune responses to SARS-CoV-2 are directed to the 4 main structural proteins of the virus which are; Spike (S), Envelope (E), Membrane (M), and Nucleocapsid (N) proteins.^15^ A specific humoral immune response against N and S protein has been reported and tend to persist in individuals.^16,17^ Immune responses to these proteins could result from natural immunity from infection or vaccination.^18^ However, It has also been noted that seroconversion can occur in asymptomatic people as well.^19^ The presence of neutralising antibodies against these proteins correlates with the protection against future SARS-CoV-2 infection.^20–22^
A COVID-19 seroprevalence range of 0% to 45% has been reported among HCWs in African countries by using a serological assessment of SARS-CoV-2 antibodies.^23^ A study from East Africa reported SARS-CoV-2 seroprevalence of 19.7% among HCWs in Kenya.^24^ There is a wide heterogeneity of SARS-CoV-2 seroprevalence among HCWs. This could be attributed to studies done at different timeframes during the pandemic. Additionally, the steps taken by each country’s health system to protect healthcare professionals from COVID-19 disease varied.^25^
Since the antibody response is a reliable proxy indicator of exposure to an infectious agent,^26^ monitoring SARSCoV-2 antibody response is crucial for understanding the burden of exposure to SARS-CoV-2 among the higher-risk groups such as HCWs. Assessing the concentration of SARS-COV-2 IgG antibodies among HCWs would aid in knowing not only their immunity but also exposure history to SARS-CoV-2. It will also aid in developing new strategies to protect this susceptible community from COVID-19 and future pandemic. At the time of the study’s design and conduct, no published reports on the SARS-CoV-2 IgG antibody response among HCWs in Tanzania were available. This study aimed to assess the seroprevalence of SARS-CoV-2 IgG antibodies among HCWs with different demographic profiles in North-Eastern Tanzania.
METHODOLOGY
Study Setting and Design
This cross sectional study was conducted from September to November, 2022 at Kilimanjaro Christian Medical Centre (KCMC), one of the four tertiary, zonal referral hospitals in Tanzania. KCMC, a 640 bed facility with 1300 healthcare workers^27^ was purposively selected due to its designation as a national centre for managing COVID-19 cases during the pandemic, and its location in the North-Eastern region of Tanzania. Kilimanjaro and Arusha regions are renowned as Tanzania’s safari capitals. The regions are popular stopovers for adventurers who are preparing to trek Mount Kilimanjaro. This makes Kilimanjaro region vulnerable to cross border transmission of infectious diseases, including SARS-CoV-2.
Study Population
This study involved HCWs working at KCMC during the study period. Any person employed or volunteering in this setting was selected based on the definition of a HCW by WHO.^11^ If the selected HCWs did not consent to participate or donate a blood sample, they were considered as ineligible for the study and thus excluded.
Sample Size and Sampling Technique
Since no prior data on the prevalence of SARS-COV-2 antibodies among HCWs in Tanzania were available during the study’s design, an estimate of 50% as seroprevalence of SARS COV-2 antibodies among HCWs was assumed to calculate a sufficient sample size. Using the formula by Pourhoseingholi et al^28^, and assuming an infinite population, a desired precision of 0.05, and a confidence level of 95%, a minimum sample size of 384 HCWs was computed. With a known population of 1300 HCWs at KCMC, an estimated sample size of 297 HCWs was computed using the finite population correction formula.^29^ Out of these, 273 HCWs participated in the study based on their availability. To ensure fair representation, the HCWs were stratified into 13 strata based on the different departments at KCMC. Both inpatient and outpatient HCWs were selected from each stratum. Given the demanding schedules of the HCWs, systematic recruitment within the strata was not feasible. Therefore, a convenience sample of up to 38 HCWs was selected from each stratum.
Data Collection Procedures
HCWs who consented to participate in the study were interviewed using a study questionnaire embedded in Redcap Software installed on an Android tablet. This tool, validated by the WHO Regional Office for Africa (AFRO), was designed specifically for use in healthcare workers cohort studies on SARS-CoV-2 antibody screening.^30^ For this study, only the sections relevant to participant enrolment were utilised. This adapted questionnaire included socio demographic and clinical characteristics, information about COVID-19 vaccination history, and COVID-19 illness, occupation and community-related behaviour during the pandemic.
Sample Collection
From each study participant, a total of 2 millilitres of blood sample through venepuncture was collected under aseptic conditions. Samples were stored in a cool box (maintained at 4–8°C using ice packs) in the field for a maximum of 3 hours before these samples were transferred to the Biotechnology Laboratory at Kilimanjaro Clinical Research Institute for serum extraction. The samples had their serum extracted instantly upon arrival at the Laboratory. For serum extraction, samples were allowed to clot then centrifuged at 1000 g for 15 minutes. After that, the serum was collected and kept frozen at negative 20°C.
Detection of SARS-COV-2 Antibodies
IgG antibodies against SARS-CoV-2 were detected by using Generic Assays (GA) Enzyme-Linked Immuno-Sorbent assay (ELISA) for SARS-CoV-2 IgG Screening kits (MedipanGmbHGA Generic Assays GmbH, Ludwig-Erhard-Ring 3, 15827 Blankenfelde-Mahlow OT Dahlewitz, Germany). This indirect ELISA kit was a two-stage that focuses on the Spike and Nucleocapsid antigen of the SARS-CoV-2 virus detection. The reported sensitivity and specificity of these GA ELISA tests are > 98%. ^31^ Concentration results obtained from the standard curve were then interpreted as either strong positive, positive, weakly positive, borderline or negative according to the manufacturer’s cut-off value for concentrations.
Statistical Analysis
STATA statistical software version 15 was used to do all statistical tests. Hence, all data from the created spreadsheet was imported to STATA. Some figures (Figure 1, 2 and 3) were generated by using GraphPad Prism v 9.5.1 Descriptive statistics was used to summarise the study participant’s baseline socio-demographic, clinical, COVID-19 exposure history and the seroprevalence of antibodies against SARS-CoV-2. After verifying that SARS-CoV-2 IgG concentration among HCWs is not normally distributed (p =0.00132 by Shapiro Wilk test), non-parametric tests were performed to compare the relationship between the exposure variables and median SARS-CoV-2 IgG concentration. The Mann–Whitney test was used to compare antibody concentrations of two independent groups. The Kruskal–Wallis test was used to compare more than two groups. A p-value of 0.05 was regarded as the cut-off for statistical significance.
Seroprevalence of SARS-CoV-2 IgG Antibody Concentrations Among the Study participants (N=273)
Seroprevalence of SARS-CoV-2 IgG Antibody Concentrations Among Non-Vaccinated Participants (N=169)
Seroprevalence of SARS-CoV-2 IgG Antibody Concentrations Among Vaccinated Participants (N=103)
Ethical Considerations
Ethical clearance for this study was obtained from the College Research and Ethical Review Committee (CRERC) of Kilimanjaro Christian Medical University College (KCMUCo), with ethical clearance number PG61/2022. After the proposal was submitted and accepted by the ethical committee, permission from the district administration (Medical Officer, Administrative Secretary, and Executive Director), and hospital administration was sought. The questionnaire and blood samples were labelled using numbers and letters to conceal participants’ identities.
RESULTS
Response Rate
A total of 273 participants had their serum SARS-CoV-2 IgG concentrations determined.
Demographic and Clinical-Exposure Characteristics of the Study Participants
Of the 273 participants tested, half were below 32 years old, with a median age of 32 (IQR: 26–44) and a male predominance of 60.4% among the total number of participants. The majority of study participants were nurses (40.5 %) and had a normal BMI (40.8%). Less than half of the study participants received the COVID-19 vaccine, and only 8.8% reported being ever tested PCR positive for COVID-19 in the past. The vast majority of participants (94.1%) stated that they had never smoked, Table 1
Occupational and Community-Related Behaviour Factors during the Pandemic
The majority of participants (58.3%) reported interacting with COVID-19 patients. A significant proportion (56.6%) always practiced good hand hygiene as recommended, 38.9% adhered to IPC standard precautions when in contact with patients. Less than half (42.4%) consistently wore PPE based on risk assessment. Half of the participants lived in households of 3 to 5 people, and 39.5% used public transportation more than nine times a day, Table 2.
Seroprevalence of SARS-CoV-2 IgG Antibody Concentration among the Study Participants
Nearly all participants (99.6%) tested positive for SARS-CoV-2 IgG antibody, with 64.5% exhibiting strong seropositivity (Figure 1). A comparison between vaccinated and unvaccinated individuals revealed that the majority of vaccinated participants demonstrated strong seropositivity (Figures 2 and 3).
Socio-Demographic, Clinical, and Behavioural Characteristics Associated with Variation in Median SARS-CoV-2 IgG Concentration among Study Participants.
Sex, BMI, smoking status, adherence to recommended hand hygiene, professional cadre, and interaction with COVID-19 patients were variables significantly influencing median SARS-CoV-2 IgG concentrations. IgG median concentration was significantly higher in females compared to males. It was found that those with obesity had significantly greater median concentrations than individuals with other BMI categories. Non-smokers showed higher SARS-CoV-2 IgG median concentrations than current smokers. Individuals who frequently adhered to recommended hand hygiene practice were found to have a significantly higher median concentration. Moreover, median concentrations were significantly greater in either individual who interacted with COVID-19 patients. Interestingly, allied health professionals had significantly higher median concentration compared to other health care workers. Other factors were assessed but did not show statistically significant differences in median SARSCOV 2 IgG concentration among participants (Figure 4).
SARS COV-2 IgG Concentrations Across Different Participant Exposure Groups and Social-Behavioural Factors
DISCUSSION
This study aimed to determine the IgG antibody response to SARS-CoV-2 among HCWs in KCMC. The findings revealed a remarkably high seroprevalence of 99.6% among the sampled HCWs. Notably, significantly higher median SARS-CoV-2 antibody concentrations were observed in females, allied health professionals, obese participants, HCWs who adhered to recommended hand hygiene practices, and those with frequent interactions with COVID-19 patients. This higher seroprevalence of SARS-CoV-2 antibodies among HCWs reflects the substantial level of virus exposure in their occupation and the ongoing risk of infection within the hospital. These findings align with other studies that have reported high seroprevalence of SARS-CoV-2 antibodies among HCWs.^32,33^ However, the seroprevalence observed in this study is higher than that reported in other East African countries.^34–36^ This significant discrepancy may be attributed to the level of COVID-19 precautions initially implemented in Tanzania as compared to other East African countries.
Our study findings revealed that HCWs who interacted with COVID-19 patients had significantly higher median antibody concentrations. However, it’s important to note that the number of COVID-19 patients to which a HCW was exposed to did not predict seroconversion. This confirms that while exposure to COVID-19 patients may be a significant factor in the detection of SARS-CoV-2 antibodies among HCWs, the sheer number of patients alone is not a reliable predictor of seroconversion. These results are consistent with earlier studies that demonstrated regular interaction with COVID-19 patients increases the risk of contracting SARS-CoV-2.^25,37–41^
Contrary to expectations, this study did not find any statistical differences in antibody concentrations among HCWs based on their history of testing PCR positive for COVID-19. Unlike previous studies, this study was unable to demonstrate that a prior SARS-CoV-2 infection leads to seropositivity for SARS-CoV-2 antibodies.^25,42–44^ Several factors may have influenced these results. The low percentage of healthcare workers who tested positive in this study might have contributed to the findings. Additionally, the significant decline in SARS-CoV-2 antibody levels after infection could additionally explain these results.^45^ Therefore, identifying an appropriate time interval for antibody monitoring is crucial to determine how long SARS-CoV-2 antibodies persist.
This study found that allied health professional had a higher median SARS-CoV-2 IgG concentration compared to other HCWs cadres. This indicates an increased risk of SARS-CoV-2 exposure among this group. A plausible explanation could be that allied health professionals often engage in hands-on, close-contact care with patients, including those with COVID-19. Such direct and frequent interactions likely lead to higher exposure levels. Additionally, allied health professionals may perform tasks that require prolonged presence in contaminated areas or close proximity to infected patients, further heightening their risk. These findings align with a previous observational study, that reported higher odds of seropositivity among allied health professionals compared to medical doctors.^46^ The specific reasons behind this finding will be explored in a separate study, aiming to identify strategies to better protect allied healthcare workers from the risk of acquiring communicable diseases in their work environment.
Another significant finding was the higher median IgG antibody concentration observed among HCWs who strictly adhered to recommended hand hygiene practices during the pandemic. This finding contrasts with other studies that found no association between self-reported hand hygiene adherence and SARS-CoV-2 antibody positivity among HCWs.^47^ Hand hygiene is a critical component of infection prevention practices in hospitals and reflects underlying behaviours, attitudes, and beliefs.^48^ It is a possibility that healthcare workers who adhered to recommended hand hygiene were also more likely to have received the COVID-19 vaccine. However, this hypothesis was not explored in the current study and warrants further exploration to better understand the interplay between hand hygiene practices, vaccination uptake, and SARS-CoV-2 antibody responses.
Our findings indicate that females had higher median concentrations of SARS-CoV-2 antibodies than males, supporting the theory that females tend to produce higher antibody levels after infections, potentially due to male androgens being suppressive to the immune system,^49^ exposing males to serious adverse clinical outcomes and higher mortality rates.^53,54^ Contrary to our findings, several other studies have reported higher SARS-CoV-2 antibody levels in male HCWs compared to females, often attributing this observation to behavioural differences.^35,39,50–52^
The results of this study suggests that individuals who currently smoke exhibits lower antibody response to SARSCoV-2. This may be due to the fact that smoking increases the clearance of circulating antibodies by enhancing the production of monocytes and macrophages.^55,56^ However, it is important to note that other studies have not found any association between smoking and SARS-CoV-2 antibody concentrations. These discrepancies are likely due to differences in study population characteristics, methodologies, or other confounding factors.^57,58^ Further research is necessary to clarify the relationship between smoking and antibody responses to SARS-CoV-2.
CONCLUSION
This study reports findings of a comprehensive assessment of the IgG antibody response to SARS-CoV-2 among HCWs at KCMC in Tanzania, showing a remarkably high seroprevalence. The results pinpoint several key factors associated with higher median SARS-CoV-2 IgG antibody concentrations, including female gender, allied health professional status, obesity, adherence to hand hygiene practices, frequent interaction with COVID-19 patients, and COVID-19 vaccination. These findings underscore the substantial virus exposure among HCWs and the ongoing risk of infection within hospital settings. The notably higher seroprevalence observed in this study compared to other East African countries may reflect differences in the implementation of COVID-19 precautions adopted by other countries such as lock down contrary to those adopted in Tanzania. Additionally, while the correlation between adherences to hand hygiene and elevated antibody concentrations cannot be precisely explained by our findings, it may reflect better adherence to COVID-19 precautions, potentially including higher vaccine uptake among adhering HCWs. These findings contribute valuable insights into the factors influencing antibody responses among HCWs, offering potential directions for future research and targeted protective measures in healthcare settings.
Recommendations
Based on the findings of this study, we recommend reinforcement and improvement of infection control measures, including stringent hand hygiene practices and the persistent use of personal protective equipment (PPE) by HCWs, to address the high seroprevalence and exposure levels. Allied health professionals, who are at increased risk, should receive additional protective measures, such as enhanced PPE and targeted training. Enhance disease outbreak preparedness by instituting regular surveillance of emerging pathogens to guide control strategies.
Study limitations and strengths
While this study has achieved its objectives, several limitations should be noted. The scope of the study was limited in terms of coverage, as it was conducted in a single centre, a tertiary hospital, where SARS-CoV-2 virus exposure levels are likely higher than in other settings. Therefore, caution must be applied in result generalisation to broader populations. Additionally, the retrospective assessment of self-reported exposure may have introduced recall bias, potentially affecting the accuracy of exposure data. Notwithstanding these limitations, this is among the first studies reporting the seroprevalence of SARS-CoV-2 IgG antibodies among HCWs in Tanzania, providing valuable insights into exposure levels and antibody responses in this high-risk group. These findings contribute important baseline data for future research and the development of targeted interventions to protect HCWs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Harapan H, Itoh N, Yufika A, et al. Coronavirus disease 2019 (COVID-19): A literature review. Journal of Infection and Public Health. 2020;13(5):667–673. doi: 10.1016/j.jiph.2020.03.01932340833 PMC 7142680 · doi ↗ · pubmed ↗
- 2Zhu N, Zhang D, Wang W, et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi: 10.1056/NEJ Moa 200101731978945 PMC 7092803 · doi ↗ · pubmed ↗
- 3Poudel K, Subedi P. Impact of COVID-19 pandemic on socioeconomic and mental health aspects in Nepal. Int J Soc Psychiatry. 2020;66(8):748–755. doi: 10.1177/002076402094224732650687 PMC 7443960 · doi ↗ · pubmed ↗
- 4Wang C, Wang D, Abbas J, Duan K, Mubeen R. Global Financial Crisis, Smart Lockdown Strategies, and the COVID-19 Spillover Impacts: A Global Perspective Implications From Southeast Asia. Frontiers in Psychiatry. 2021;12. Accessed May 19, 2023. https://www.frontiersin.org/articles/10.3389/fpsyt.2021.64378310.3389/fpsyt.2021.643783 PMC 844639134539457 · doi ↗ · pubmed ↗
- 5Lekagul A, Chattong A, Rueangsom P, Waleewong O, Tangcharoensathien V. Multi-dimensional impacts of Coronavirus disease 2019 pandemic on Sustainable Development Goal achievement. Globalization and Health. 2022;18(1):65. doi: 10.1186/s 12992-022-00861-135761400 PMC 9235167 · doi ↗ · pubmed ↗
- 6Mehta OP, Bhandari P, Raut A, Kacimi SEO, Huy NT. Coronavirus Disease (COVID-19): Comprehensive Review of Clinical Presentation. Frontiers in Public Health. 2021;8. Accessed May 19, 2023. https://www.frontiersin.org/articles/10.3389/fpubh.2020.58293210.3389/fpubh.2020.582932 PMC 784432033520910 · doi ↗ · pubmed ↗
- 7Tarimo CS, Wu J. The first confirmed case of COVID-19 in Tanzania: recommendations based on lesson learned from China. Tropical Medicine and Health. 2020;48(1):25. doi: 10.1186/s 41182-020-00214-x 32355447 PMC 7183743 · doi ↗ · pubmed ↗
- 8World Health Organization. The Impact of COVID-19 on Health and Care Workers: A Closer Look at Deaths. World Health Organization; 2021. https://apps.who.int/iris/handle/10665/345300