‘No One Has Taught Us to Have It All’: Reflections from Women on the Gender-Based Challenges in Surgical Careers in Africa
Marcella F.D. Ryan-Coker, Mwanaidi Ayumba, Lotta Velin, Ala Magzoub, Joselyne Nzisabira, Grace Paidamoyo Gwini, Samuel Mesfin Girma, Aemon Berhane Fissha, Amy Paterson

TL;DR
This paper explores the gender-based challenges African women face in pursuing surgical careers and highlights the need for systemic change to promote equity.
Contribution
The study provides a detailed analysis of gender barriers in African surgical fields through survey data from women across various career stages.
Findings
63% of participants reported experiencing gender-based discrimination in their surgical careers.
74% cited societal and familial discouragement as major barriers to pursuing surgery.
Participants reported facing sexist comments, underestimation of skills, and sexual harassment.
Abstract
The surgical field in Africa has long grappled with a gender imbalance, with women being significantly underrepresented. Despite global efforts to foster gender diversity in healthcare practices, African women pursuing surgical careers still face substantial hurdles. This paper investigates these women’s experiences and challenges, aiming to raise awareness of these issues and propose strategies for improving gender equity. To describe contextual aspects of barriers affecting women in surgery in Africa. A cross-sectional survey was conducted, targeting female medical students interested in surgical careers, interns, trainees, and surgical consultants across Africa. The survey was distributed in November-December 2021. Data were analysed using descriptive statistics for quantitative data and a simplified thematic analysis for qualitative data. A total of 105 participants from 17…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
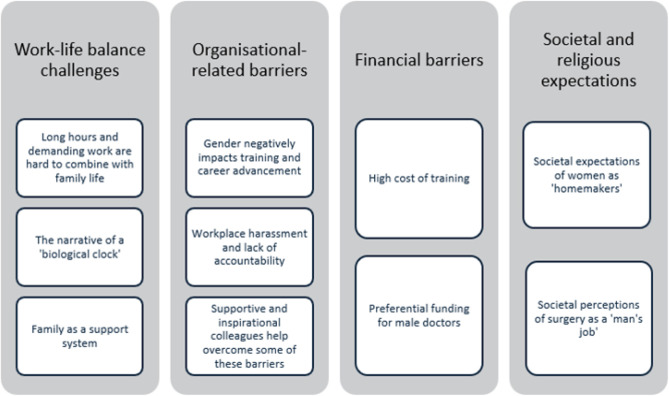 Figure 1
Figure 1| Demographic Data | Frequency | Percentage (%) |
|---|---|---|
| Age range (years) | ||
| <30 | 74 | 70.5 |
| 30-40 | 27 | 25.7 |
| 40-50 | 4 | 3.8 |
| Country of origin | ||
| Kenya | 23 | 22.1 |
| Zimbabwe | 18 | 17.3 |
| Sudan | 13 | 12.5 |
| South Africa | 11 | 10.6 |
| Sierra Leone | 10 | 9.6 |
| Others | 8 | 7.7 |
| Current country of residency | ||
| Kenya | 25 | 24.0 |
| Zimbabwe | 17 | 16.3 |
| Sudan | 14 | 13.5 |
| Sierra Leone | 9 | 8.7 |
| Others | 8 | 7.7 |
| Marital status | ||
| Single | 78 | 74.3 |
| Married | 22 | 20.9 |
| Engaged | 3 | 2.9 |
| Separated | 2 | 1.9 |
| Religion | ||
| Christian | 73 | 69.5 |
| Muslim | 24 | 22.9 |
| Not religious | 4 | 3.8 |
| Prefer not to say | 4 | 3.8 |
| Children | ||
| No | 83 | 79.1 |
| Yes | 22 | 20.9 |
| Number of children | ||
| 1 | 12 | 54.5 |
| 2 | 6 | 27.3 |
| 3 or more | 4 | 18.2 |
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Training level | ||
| Medical student | 56 | 53.3 |
| Registrar | 10 | 9.5 |
| House Officer/Intern | 10 | 9.5 |
| Medical officer | 10 | 9.5 |
| Specialist/Consultant | 13 | 12.4 |
| General practitioner | 1 | 0.9 |
| Independent practitioner | 1 | 0.9 |
| Not stated | 3 | 2.8 |
| Type of work institution | ||
| Public | 38 | 79.2 |
| Private | 10 | 20.8 |
| Mission/NGO | 3 | 6.2 |
| Surgical specialty | ||
| General Surgery | 20 | 41.7 |
| Obstetrics & Gynaecology | 8 | 16.7 |
| Orthopaedics | 5 | 10.4 |
| Paediatrics | 5 | 10.4 |
| Neurosurgery | 4 | 8.3 |
| Plastic & Reconstructive Surgery | 2 | 4.2 |
| Urology | 2 | 4.2 |
| Cardiothoracic & Vascular Surgery | 1 | 2.1 |
| Surgical Oncology | 1 | 2.1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiversity and Career in Medicine · Global Health Workforce Issues · Dental Education, Practice, Research
BACKGROUND
In medicine, the surgical profession symbolises precision, courage, and life-saving innovations. However, for women in surgery, the path to becoming a surgeon remains strewn with numerous and often profoundly ingrained obstacles. Throughout history, the surgical arena globally has been predominantly the domain of men.^1^ Surgical training demands an unwavering commitment to rigorous training and access to opportunities, hence why it is often argued to be a better career fit for men.^2,3^
Africa’s unique cultural tapestry, socioeconomic disparities, and evolving healthcare landscapes have given rise to a distinct set of hurdles for women with surgical aspirations. The continent faces a severe shortage of specialist surgical workforce, owning only ~12% of the global surgical workforce despite hosting over a third of the population.^4,5^ Although women in surgery in Africa have come a long way from being about 9% to about 23% of all practicing surgeons on the continent, there is still a significant gap.^4,6^ Societal norms, traditional gender roles, limited access to quality education, workplace bias, and a dearth of female surgical mentors collectively contribute to this gender gap.^7,8^ Most existing studies on this issue in the region are focused on individual countries. This multinational survey aims to describe contextual aspects of barriers and obstacles affecting women in surgery in Africa.
METHODS
This cross-sectional multinational online survey was conducted as part of the work of the Gender Equity Initiative in Global Surgery (GEIGS). We surveyed female medical students interested in surgical specialities, interns, medical officers, registrars, and consultants in various surgical fields across Africa.
Ethical approval was obtained from the Sierra Leone Ethics and Scientific Review Committee. Informed consent was obtained from all participants before they engaged with the online questionnaire.
A 26-item questionnaire, set up on Google Form surveys and administered in three languages (English, French, and Arabic), was used to collect data from November to December 2021 via various online platforms. The questionnaire encompassed single- and multiple-choice questions, Likert scale items, and open-ended free-text responses. The survey collected quantitative and qualitative data, including demographic data, surgical training experience, mentorship, and experiences of bias and barriers to surgical training.
Data were de-identified for confidentiality. Quantitative data were analysed using the Statistical Package for the Social Sciences (SPSS). Braun and Clarke’s simplified version of thematic analysis was used for qualitative data.^9^ Responses were organised into condensed “meaning units.” These meaning units were then grouped into sub-themes, which were further categorised into overarching themes. Direct quotations from the participants were incorporated to exemplify sub-themes and illustrate the voice of the participants.
RESULTS
Participant Demographics: A summary of participant demographics is presented in Table 1. The study featured 105 respondents, representing a diverse cross-section of individuals, predominantly young (n=74, 70% under 30 years) and unmarried (n=78, 74%). A notable 21% (n = 22) with Christianity being the predominant religious affiliation (n = 73, 70%).
Work characteristics of participants: More than half of the respondents (n=56, 53%) were medical students interested in surgical careers, most of whom were in their 4th-6th year of study. The majority of respondents (79%) worked in public healthcare institutions, though some had roles in private practice. The common specialities were general surgery (n=20) and obstetrics and gynaecology (n=8). Regarding work hours, a substantial group (48.1%) worked 41–60 hours weekly (Table 2).
Gender Bias: Sixty percent (n=63) of respondents acknowledge some form of gender bias in their training or work. Of these, 79% (n=50) reported the forms of biases experienced, which included competency underestimation (n=12, 24%), reduced opportunities for skill development and career progression (n=9, 18%), unsolicited advice (n=6, 12%), sexual harassment (n=3, 6%), and sexist jokes (n=2, 4%).
Mentorship: Mentorship was a critical factor in the experiences of the participants (n=96, 91%). However, only 36 (34%) respondents reported having a mentor, with a smaller fraction (n=17, 47%) having female mentors. Some of the perceived benefits of mentoring such as access to teaching resources and opportunities, assistance in career and personal life decision-making, increased confidence, and having a role model to aspire to.
Thematic Analysis
The inductive thematic analysis of the responses revealed four main themes (Figure 1).
Analytical Model for Thematic Analysis
Work-life balance challenges
This theme reinforces the delicate balance women in surgery must strike between demanding professional responsibilities and familial obligations. Respondents shared their experiences managing the extensive time and energy requirements of surgical training alongside the roles of mother and wife. A participant poignantly articulated, “Having to attend to emergencies at night, at the same time coming back home to the role of wife and mother, makes it difficult for spouses to accept that your job is demanding.”
Participants also reflected upon the tension of racing against the ‘biological clock,’ with societal pressures dictating timelines for marriage and family, often at odds with career aspirations. One respondent reported, “I have had to focus on work and training, so I am single. I have opted out of having children also, which is obviously frowned upon as an African.” Another said, “Society expects a ‘whole woman’ to be married and have kids at a certain age, like there are timelines to what a woman should be doing and when, hence the battle to become a societal woman and a professional woman at the same time.”
While societal expectations presented challenges, family and friends were perceived as potential sources of support. Participants acknowledged the critical role of their support systems in their surgical training, countering biases and challenges.
Organisational-related barriers
The theme of organisational-related barriers delved into experiences within medical schools, hospitals, or organisational settings. Respondents reported how gender influenced their training experience and professional progression, with women often viewed as inferior to their male counterparts. Comments such as: “Many women are looked down on or not given chances simply because of their gender” and “Being female, you are not always taken seriously. Surgery being considered a speciality for men and women not fully given a chance” illustrates some of the respondents’ lived experiences. Biases in training opportunities and clinical competency assessments emerged as key concerns, with reports such as: “Male counterparts are asked for advice first or given surgical opportunities before their female counterparts” or “at the hospital, women’s opinion is usually regarded second to that of men” or “Another assumption is that surgery requires physical strength, which females are incapable of,” highlighting the need for more inclusive practices. Descriptions of the work environment generally described the hostility faced by the respondents with comments such as: “The paramedic scrub nurse and male co-worker act with aggression towards the female surgeon or trainee.”
Workplace harassment, including sexual harassment, was a distressing reality faced by respondents at all levels of training, where the aggressors were typically at more senior levels. A medical student said, “…it is also disheartening to see incoming younger students being preyed on by men who are meant to be mentors and teachers.” The importance of reporting systems and accountability for perpetrators was emphasised. “Setting up a system in which people are held accountable for their actions. A system in which we can report or raise awareness of any form of harassment, with actual action being taken against perpetrators.”
Another sub-theme in the organisational barriers was the limited support for maternity leave and breastfeeding facilities.
Amidst the challenges, the theme of supportive colleagues in institutional settings shone through. The role of colleagues, particularly male colleagues, in providing vital support and mentorship was recognised as a powerful enabler. More senior women in leadership positions were seen as inspirational figures, driving change and motivation. One respondent remarked, “Seeing women of colour in positions of power, making big changes, is, and will always be, a massive driving push for me—if they could do it, I can too. I also often remind myself that it was probably much more difficult for them to achieve what they have given the times, and that they have lightened the load so that I may thrive too. This genuinely drives me.”
Financial barriers
The barrier of financial constraints was highlighted, including the high cost of surgical training and the limited financial resources. One respondent said, “The cost of training is ridiculous, and if no scholarships were available, I probably would not have come this far.”
Gender bias in funding allocation, favouring males, added another layer of complexity to the financial challenges faced by aspiring female surgeons. When financial support is limited, funding may preferentially be allocated to males in different levels of training. This was described both in early educational stages, which may reduce the likelihood of pursuing medical studies, and at more senior training levels. Respondents said, “Finances are directed more to the male child[ren]…” and “Financial barriers are one of the greatest challenges. Everybody, including my family, has distanced themselves. Because one medicine is expensive, and two, only men are expected to pursue sciences”. Another reported, “More often than not, young female doctors miss out on opportunities due to funds and societal pressure to settle down and take care of family. An easier path remains to give up or postpone the dreams.”
Societal and religious expectations
Societal and religious expectations were pervasive in participants’ lives, influencing personal and professional choices. Participants described the weight of societal expectations, where women were predominantly viewed as “homemakers,” impacting their ability to pursue surgical careers: “Women are viewed as homemakers more than career women, and social and family attachments make us lean more towards being homemakers; no one has taught us to have it all.” Another described these expectations: “Women are seen as helpers to their husbands, so they are expected by society to be home most of the time, taking care of their husbands and families… Men are the head, and women have to follow suit; therefore, they take on roles that are not demanding or require a high level of training.”
Furthermore, the perception of surgery as a “man’s job,” which was not compatible with the role of a wife and/or mother, added to the challenges: “Women in the medical profession feel like a surgical career is a demanding profession, and thus they will not have time to take care of/raise their families”. “People think women are not mentally or emotionally capable of practicing surgery, and they believe a woman should have to give up surgery to look after her family because a woman will not be able to handle both, so she has to sacrifice one, and that is simply not true, and if you end up going further in surgery, you are immediately described as a bad mother or wife or daughter or sister.”
The societal impact rippled through patients’ interactions, with respondents often mistaken for nurses while male nurses will be referred to as doctors due to entrenched biases. One respondent said, “Society never expects a female to be a doctor, let alone a surgeon.” Another respondent similarly highlighted the perceived belief that “patients will always prefer male surgeons.”
DISCUSSION
This study explores the multifaceted challenges African women in surgery encounter. A central theme emerging from this study is the delicate balance women in surgery must strike between their professional and personal lives. Heavy workloads and long working hours were reported as significant barriers underscoring the demanding nature of surgical careers. These demands can create conflicts with cultural and societal expectations prevalent in African societies, where women traditionally hold roles as primary caretakers and homemakers.^11^ Additionally, the confusion between female surgeons and nurses, despite their professional appearance, complicates their roles and recognition in the hospital setting. Such gender-related stereotypes and consequences, such as lowered morale or hampered self-confidence, have similarly been described in contexts beyond the African region.^19^
Pursuing a career in surgery can be perceived as neglecting these roles, leading to societal disapproval. The presence of a “marriage wage penalty” and a “motherhood wage penalty” indicates the systemic challenges faced by women in surgery, especially when they enter marriage or have children.^12^ The narrative that women must prioritise family life over their surgical careers is deeply integrated into cultural and societal expectations. Such attitudes place an additional burden on women, potentially leading to their exit from surgical training. These findings confirm reports from previous studies in Rwanda^13^, South Africa ^14^, and Australia.^15^
The financial aspect of these barriers and obstacles is a critical element that deserves attention. Although this study did not assess the cost of training, respondents identified this as a barrier. O’Callaghan et al. surveyed medical students and surgeons in the UK and found a substantial cost associated with training.^16^ Little is known about the cost of surgical training in Africa. However, in a society where more educational and training opportunities are given to boys, it is plausible that the cost associated with surgical training can be a severe limiting factor for women with surgical career aspirations.
This study uncovers the pervasive gender bias and discrimination that women in surgical training endure. The mistreatment they face is broad and includes underestimation of their skills, unequal opportunities in the workplace, mansplaining, unsolicited advice, microaggressions, sexual harassment, and sexist jokes. These findings echo previous research in Nigeria and South Africa, where the women in surgery reported having experienced some form of gender bias and discrimination.^14,17^ Laessig et al.^18^ also emphasised the presence of gender bias during training. One example described was that letters of recommendation for female surgeons often focused on their physical appearance rather than their clinical competence. This underscores the importance of addressing gender bias at various stages of surgical careers, from training to career advancement.
Some respondents reported religion to have been one of the barriers that prevented women from pursuing surgical careers. Although we could not elaborate further in this study, this finding resonates with previous studies documenting religion as a potential obstacle to female advancement into surgical professions.^4,20,21^
Despite the numerous barriers women face in surgery in Africa, this study identifies potential solutions and strategies to mitigate these. These include encouragement and support from the community and family to fulfil their aspirations while maintaining a healthy work-life balance. These efforts should also encompass mentorship, leadership roles for women in surgery, and confidence building. Providing financial support for female surgeons in training can also help alleviate the financial constraints associated with surgical careers. A fundamental shift in attitude within the surgical community is also essential. Colleagues, peers, and employers should actively support and hold accountable those who engage in discriminatory practices, harassment, and bias. Efforts should be made to allow flexible work arrangements and structured residency programs to help women pursue surgical careers without sacrificing their personal lives. Finally, the academic, healthcare, and surgical communities should work together to develop data-driven solutions and policy changes that promote gender equity.
Strengths and limitations
This study’s strength lies in its diverse participant pool, from various surgical backgrounds and cadres across Africa. It provides a comprehensive mapping of a broad range of challenges and opportunities and lays the groundwork for future in-depth interview studies. However, the primary limitations include a small sample size and a majority of medical student participants, limiting insights into some critical barriers. Additionally, responder bias may influence results, as those with interest or experience in gender discrimination may be more or less likely to participate.
CONCLUSION
This study offers a comprehensive understanding of the barriers faced by women in surgery in Africa, encompassing issues of work-life balance, hospital culture, financial barriers, and societal and religious expectations. It highlights the need for concerted efforts to overcome these challenges and foster an empowering environment that allows women to pursue their surgical careers with due recognition, respect, and support.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bellini MI, Graham Y, Hayes C, Zakeri R, Parks R, Papalois V. A woman’s place is in theatre: women’s perceptions and experiences of working in surgery from the Association of Surgeons of Great Britain and Ireland women in surgery working group. BMJ Open. 2019 Jan;9(1):e 024349.10.1136/bmjopen-2018-024349 PMC 632629230617103 · doi ↗ · pubmed ↗
- 2Mahoney ST, Strassle PD, Schroen AT, Agans RP, Turner PL, Meyer AA, et al. Survey of the US Surgeon Workforce: Practice Characteristics, Job Satisfaction, and Reasons for Leaving Surgery. J Am Coll Surg. 2020 Mar;230(3):283–293.e 1.31931143 10.1016/j.jamcollsurg.2019.12.003 · doi ↗ · pubmed ↗
- 3Malik M, Inam H, Janjua MBN, Martins RS, Zahid N, Khan S, et al. Factors Affecting Women Surgeons’ Careers in Low–Middle-Income Countries: An International Survey. World j surg. 2021 Feb;45(2):362–8.33040193 10.1007/s 00268-020-05811-9 · doi ↗ · pubmed ↗
- 4O’Flynn E, Andrew J, Hutch A, Kelly C, Jani P, Kakande I, et al. The Specialist Surgeon Workforce in East, Central and Southern Africa: A Situation Analysis. World j surg. 2016 Nov;40(11):2620–7.27283189 10.1007/s 00268-016-3601-3 · doi ↗ · pubmed ↗
- 5Ozgediz D, Riviello R, Rogers SO. The surgical workforce crisis in Africa: a call to action. Bull Am Coll Surg. 2008 Aug;93(8):10–6.19492736 · pubmed ↗
- 6Odera A, Tierney S, Mangaoang D, Mugwe R, Sanfey H. Women in Surgery Africa and research. The Lancet. 2019 May;393(10186):2120.10.1016/S 0140-6736(19)31106-731226043 · doi ↗ · pubmed ↗
- 7Jesuyajolu DA, Okeke CA, Obuh O. The Challenges Experienced By Female Surgeons in Africa: A Systematic Review. World j surg. 2022 Oct;46(10):2310–6.35789283 10.1007/s 00268-022-06650-6 · doi ↗ · pubmed ↗
- 8A Lobaid AM, Gosling C, Khasawneh E, Mc Kenna L, Williams B. Challenges Faced by Female Healthcare Professionals in the Workforce: A Scoping Review. JMDH. 2020 Aug; Volume 13:681–91.32821112 10.2147/JMDH.S 254922 PMC 7417925 · doi ↗ · pubmed ↗