Interaction between Infection of Porphyromonas gingivalis, A Keystone Microbe of Oral Microbiome, and Serum Levels of Lutein/Zeaxanthin Is Associated with Risk for Age-related Macular Degeneration
Chung-Jung Chiu, Emily Chiu, Min-Lee Chang

TL;DR
High levels of a mouth bacterium called Porphyromonas gingivalis and low levels of certain nutrients like lutein and zeaxanthin may increase the risk of age-related macular degeneration.
Contribution
This study identifies a novel association between P. gingivalis infection, serum lutein/zeaxanthin levels, and the risk of age-related macular degeneration.
Findings
Higher serum IgG levels against P. gingivalis are linked to increased odds of early AMD.
Elevated lutein/zeaxanthin levels may reduce P. gingivalis-related AMD risk by up to 35%.
The study suggests a potential interaction between oral microbiome and nutrition in AMD development.
Abstract
Porphyromonas gingivalis (P. gingivalis) functions as a catalyst bacterium in the development of periodontitis, and the serum antibody level against P. gingivalis is considered a surrogate marker for the activity level of periodontopathic microbiome. The chronic systemic inflammation induced by P. gingivalis elevates the risk of various systemic and neurodegenerative disorders, including atherosclerosis, diabetes, and Alzheimer’s disease. Although the connection between human microbiome and age-related macular degeneration (AMD) remains relatively unexplored, it is noteworthy that AMD shares risk factors and etiological mechanisms with diseases related to P. gingivalis. To investigate the potential association between periodontopathic microbiome and AMD occurrence, we conducted a candidate microbe approach case-control study. Our hypothesis was tested by examining the correlation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
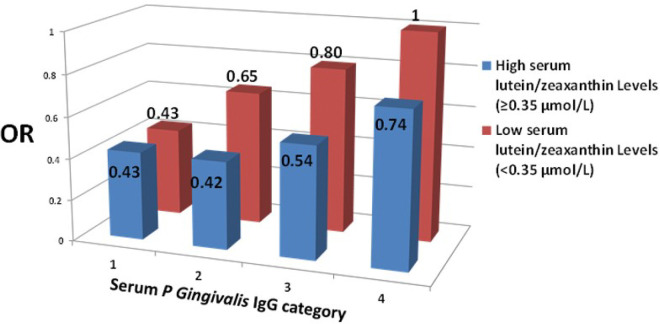 Figure 1
Figure 1- —National Institutes of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · Retinal Diseases and Treatments · Advanced Glycation End Products research
INTRODUCTION
Mucosal surfaces, including the oral mucosa, harbor a dynamic and intricate microbial community known as the “microbiome,” holding significant implications for human health and disease ^1^. Periodontal disease, a prevalent disease in human population ^2,3^, is significantly attributed to Porphyromonas gingivalis (P. gingivalis) ^4,5^, a gram-negative anaerobe primarily residing in the oral cavity. Colonizing the subgingiva, P. gingivalis contributes to the formation of a destructive biofilm (dental plaque) within a multispecies microbe community, leading to alveolar bone loss ^6^. Despite its low abundance, P. gingivalis acts as a catalyst in periodontitis, reshaping the composition of the oral commensal microbiome into a dysbiotic state, accelerating microbiome-mediated bone-destructive periodontitis ^7^. Moreover, the chronic trickling of this bacterium into the systemic bloodstream triggers a systemic inflammatory response, elevating levels of various inflammatory mediators ^8^. This P. gingivalis-induced systemic inflammation is linked to increased risks of systemic diseases such as atherosclerosis, rheumatoid arthritis, metabolic disorders ^4,9–12^, and neurodegenerative diseases, including cognition impairment and Alzheimer’s disease ^13,14^. This microbe serves as a vivid example of how the microbiome can impact diverse aspects of human health and disease in locations distant from its original habitat in the body. Significantly, our previous studies indicate that specific patterns of oral microbiome are strongly associated with human health and diseases, with P. gingivalis playing a pivotal role in patterns affecting retinal eye health ^15,16^. Age-related macular degeneration (AMD), a neurodegenerative disease of the retina causing blindness in individuals aged 65 + ^17^, shares risk factors and etiological mechanisms with P. gingivalis-related diseases ^18^. Hence, there is a hypothesis that periodontopathic microbiome is linked to the occurrence of AMD. To explore this, a “candidate microbe approach, association study” was conducted, correlating serum P. gingivalis immunoglobulin G (IgG) with AMD in a matched case-control study using data from the Third National Health and Nutrition Examination Survey (NHANES-III), a representative sample of the US population. Additionally, investigations were carried out to determine if modifiable risk factors for AMD could influence the P. gingivalis-related risk.
MATERIALS and METHODS
Study cohort
The Third National Health and Nutrition Examination Survey (NHANES-III) was performed between 1988 and 1994 by the National Center for Health Statistics. It is a cross-sectional nationwide health survey of 33994 non-institutionalized US residents aged 2 months and older using a stratified multistage probability sampling design to sample a representative cohort of the US general population.
Case and control definitions
During the second phase of NHANES-III enrollment (1991–1994), 9371 persons had serum analysis for immunoglobulin levels of P. gingivalis ^19^, with 2925 persons ≥ 55 years of age. Of these, 1933 persons had gradable bilateral fundus photography at the time of the complete examination. We excluded persons with history of diabetes, heart attack, stroke, cancer, and missing covariate information. Races other than non-Hispanic white, non-Hispanic black, Mexican-American and participants on immunomodulatory medications or corticosteroids were also excluded from our study. Among non-smokers, other tobacco product users such as chewing tobacco, cigar, and pipe and cotinine level > 15 ng/ml were also excluded. Among the remaining eligible 1070 persons, 174 persons were identified as early AMD cases and 12 persons as late AMD cases. Early AMD was defined as the presence of either soft drusen (≥ 63 μm, equivalent to Grade 3 drusen in the Wisconsin Age-related Maculopathy Grading System) ^20^ or any drusen type with areas of depigmentation or hypopigmentation of the retinal pigment epithelium (RPE) without any visibility of choroidal vessels or with increased retinal pigment in the macular area. Late AMD was defined as the presence of signs of exudative macular degeneration or geographic atrophy (sharply delineated roughly round or oval area of apparent absence of the RPE in which choroidal vessels are more visible than in surrounding areas). The intergrader and intragrader Kappa scores ranged from 0.62 to 0.83 for the NHANES-III AMD grading, indicating a good reliability ^21^. Among the remaining 884 non-AMD persons, we selected a series of control subjects by a random selection of one-by-one frequency matching in age, sex, and race such that the overall characteristics distributions of the controls resembled the overall characteristics distributions of the cases.
Serum P. gingivalis immunoglobulin G
Serum P. gingivalis IgG indicates systemic response to this periodontal disease-causing pathogenic bacterium. The antibody measurement in the NHANES-III data set was reported in enzyme-linked immunosorbent assay (ELISA) units (EU) of IgG. The detailed measurement methods are previously described elsewhere (National Center for Health Statistics NHANES III Data Documentation. http://www.cdc.gov/nchs/data/nhanes/nhanes3/depp.pdf). To examine for possible dose-response relationships of P. gingivalis IgG and AMD risk, we retained the same categorization ranges of P. gingivalis IgG from previous report from the Atherosclerosis Risk in Communities Study (ARIC) ^22^, which had similar demographics to the NHANES-III subjects ^14^. The report showed a significant (P < 0.0001) relationship between periodontitis severity and P. gingivalis IgG with a mean P. gingivalis IgG for healthy individuals of 53.8 EU, mild periodontitis 60.9 EU, moderate periodontitis 69.4 EU and severe periodontitis 168.4 EU. The midpoint between each of these P. gingivalis IgG means was used to create cut-off points for the four P. gingivalis IgG groups: ≤57 EU (referent), 58–65 EU, 66–119 EU and > 119 EU (highest).
Statistical methods
The following were considered as covariates in our analyses: age, sex, race, education level, smoking status, body mass index (BMI, computed from weight and height; Kg/m^2^), drinking alcohol (at least 12 drinks in the past 12 months), serum levels of C reactive protein (CRP), vitamin C, vitamin E, and lutein/zeaxanthin, and two clinical periodontal measurements (mean number of tooth sites that bled on probing [mBOP] and mean clinical attachment loss [mCAL]). Descriptive statistics for these covariates between cases and controls were calculated. To determine significance of differences, analysis of variance (ANOVA) for comparison of means of continuous variables and chi-square tests for categorical variables were used. We also examined the correlations between serum P. gingivalis IgG and these covariates using Spearman correlation coefficients, Mann-Whitney tests, or Kruskal-Wallis tests, as appropriate.
To evaluate the association between P. gingivalis IgG and AMD risk, logistic regression models were fitted by controlling for selected covariates. All analyses were performed using SAS^®^ SURVEYLOGISTIC procedure (version 9.3; SAS Institute Inc, Cary, NC), which takes into account of the complex sampling design used in NHANES-III and yields unbiased standard error (SEM) and confidence interval (CI) estimates. Odds ratios (ORs) were calculated by dividing the odds of AMD among persons in higher categories of serum levels of P. gingivalis IgG by the odds among persons in the lowest category of P. gingivalis IgG. We used P < 0.05 to denote statistical significance and all tests were two-sided.
This study involved only the secondary data analysis of existing US national databases that are publicly available and have been de-identified. This research qualified for exemption of institutional review board human subjects approval under 45 CFR 46.101(b) (4) as specified by the Federal Regulations for Protection of Human Research Subjects. Thus, this is an exempt study and there was no need for institutional review board approval from our institutions. This human observational study report was prepared to conform to the STROBE guidelines.
RESULTS
Since our controls were matched with cases in age, sex, and race, it is not surprising that the distributions of these three covariates were not significantly different between cases and controls (Table 1). Probably due to this matching strategy, the distributions for the other covariates were not significantly different, either. However, serum P. gingivalis IgG categorical distributions showed significantly different (P<0.0001) between cases and controls, and cases tended to be in the higher IgG categorical levels than controls, and the vice versa.
In our bivariate analysis, age (P=0.007) and serum vitamin C level (P=0.004) were inversely correlated with serum P. gingivalis IgG level while serum vitamin E level (P=0.004) was positively correlated (Table 2). Male sex (P=0.01), non-Hispanic black (P<0.0001), lower levels of education (P=0.01), and former smokers (P=0.001) tended to have higher levels of serum P. gingivalis IgG. However, BMI, alcoholic intake, and serum levels of lutein/zeaxanthin and CRP were not significantly correlated with serum P. gingivalis IgG level.
Next, in the logistic analysis evaluating our primary interest of the association between serum P. gingivalis IgG level and risk for AMD, we used a hierarchical strategy in our model construction to examine the confounding effects from the covariates (Table 3). Starting from an age-adjusted model (Model 1), we stepwise included the other covariates; Model 2 additionally adjusted for demographic covariates, including sex, race, BMI and education; Model 3 additionally adjusted for habitual exposures, including smoking history and alcohol intake; Model 4 additionally adjusted for serum levels of nutrient covariates, including vitamin C, vitamin E, lutein/zeaxanthin, and CRP, and Model 5 additionally adjusted for two clinical periodontal measurements (mBOP and mCAL). As shown in Table 3, the OR and 95% CI for each serum P. gingivalis IgG categorical level in every higher hierarchical models were similar with the age-adjusted OR and 95% CI, which showed a significant trend (P=0.036) of increased risk by increasing serum P. gingivalis IgG level. Overall, compared with the lowest IgG category, the second higher category conferred a 20% increased risk for early AMD, the third higher category conferred a 40%–60%, and the highest (fourth) category conferred an over two-fold of risk. Because including more covariates in the models decreases the statistical power, the trend tests became less significant in higher hierarchical models, however, they were all within marginal significance (P<0.1). Similar results were noted when including the 12 late AMD cases (see Case and control definitions) in the analysis.
We further tried to evaluate if the effect of serum P. gingivalis IgG level on AMD risk varies by the status of modifiable risk factors for AMD, including smoking status (ever smokers vs. non-smokers), BMI (≥25 vs. <25 or ≥28 vs. <28 or ≥30 vs. <30 Kg/m^2^), and serum levels (higher vs. lower than the median) of vitamin C (median=39 mmol/L), vitamin E (median=23.5 μmol/L), and lutein/zeaxanthin (mediam=0.35 μmol/L). The results indicated that the P. gingivalis-related AMD risk significantly (P for interaction<0.0001) varies by serum levels of lutein/zeaxanthin (≥0.35 μmol/L vs. <0.35 μmol/L). Compared subjects in the low serum level of lutein/zeaxanthin with those in the high serum level, there is an up to 35.4% (=(0.65–0.42)/0.65) higher risk of AMD for serum P. gingivalis IgG category 2 (58–65 EU), 32.5% (=(0.80–0.54)/0.80) for category 3, and 26% (=(1–0.74)/1) for category 4 (Figure 1). In other words, higher serum lutein/zeaxanthin levels were protective against P. gingivalis-related AMD risk.
DISCUSSION
Traditionally, microbiology in the context of human health primarily concentrated on local effects. However, our study has revealed a notable shift in perspective, demonstrating a positive association between the serum signature of P. gingivalis and the risk of AMD. This contributes to the growing body of evidence suggesting that the microbiome within the human body can exert influences on distant tissues and organs. Additionally, aligning with the notion that the microbiome composition is significantly shaped by host’s diet, our findings indicate that elevated serum levels of lutein/zeaxanthin offer a protective effect against the P. gingivalis-related AMD risk.
To date, only few studies have been published that explores the correlation between periodontitis and AMD ^23–25^. Although pooled analysis suggested that periodontitis patients may have a higher risk of AMD ^23,24^, bias assessment and power analysis indicated that the association remains debatable ^25^.
As part of the cross-sectional Finnish national population-based Health 2000 Survey ^26^, 1751 individuals aged 30 years or older were included in the study, consisting of 54 individuals with degenerative fundus changes (AMD group) and 1,697 individuals free of AMD (non-AMD group). In their univariate analysis comparing the AMD group with the non-AMD group, Karesvuo et al. identified a significant difference in the proportion of individuals with alveolar bone loss among males and a significant difference in the number of teeth among females. However, likely due to insufficient case numbers and control selection, no significant difference was found between the AMD group and the non-AMD group in terms of the proportion of carriage of salivary periodontopathic bacteria, including P. gingivalis. Following multivariate adjustment for various factors such as age, diabetic status, systolic blood pressure, education, smoking, and the carriage of salivary bacteria, only alveolar bone loss remained significantly associated with the risk of AMD among males.
While previous research has proposed infection as a potential risk factor for AMD ^27^, and P. gingivalis has been linked to various human neurodegenerative disorders ^13,14^, our study is the first to establish a significant relationship between P. gingivalis and AMD. Notably, P. gingivalis is not limited to the oral cavity, as it also inhabits other sites within the human body. The ubiquitously expressed transglutaminase 2 (TG2) plays a crucial role in P. gingivalis adherence to host cells ^6^, with periodontitis being its sole known clinical manifestation in situ. Furthermore, P. gingivalis acts as a catalyst in periodontopathic microbiome, and the serum P. gingivalis IgG level has been demonstrated to closely correlate with the severity of periodontitis ^7,22^. As a result, the serum P. gingivalis IgG level can function as a surrogate marker for the activity level of periodontopathic microbiome in the oral cavity ^4^.
In contrast to most pathogenic bacteria that typically induce severe inflammation and outcompete native bacteria, P. gingivalis establishes colonization at low levels and functions as a “catalyst” to foster a pathogenic microbiome (pathobionts). Studies in a murine periodontal model have demonstrated that even at low numbers, the introduction of P. gingivalis into the oral microbiome community significantly accelerates pathological alveolar bone loss ^28^. However, since P. gingivalis alone fails to induce periodontitis, the hypothesis arises that P. gingivalis exerts its bone-destructive role in collaboration with other dysbiotic bacteria. Mechanistic investigations indicate that P. gingivalis colonization in the oral cavity disrupts the host immune system and induces changes in the quantity and composition of the oral commensal microbiome. This occurs through the secretion of gingipain, a complement component 5 (C5) convertase-like enzyme. Gingipain generates elevated levels of locally active C5a, leading to C5aR activation, triggering inflammation while simultaneously inhibiting the killing capacity of leukocytes and suppressing the expression of chemokines. Studies further highlight the significance of the complement pathway in P. gingivalis-related pathogenesis, proposing the targeting of C3 as a potential treatment strategy for periodontitis ^29^. Interestingly, it is well-documented that the activation of C3 and the generation of excessive quantities of C5a and C5b-C9 play a significant role in the pathogenesis of AMD ^30^. While it has been established that the inflammatory and immune response triggered by P. gingivalis has both local and systemic effects ^4,9–12^, the impact of gingipain, C5 activation, and the dysbiotic microbiome induced by P. gingivalis on the retina is yet to be determined.
If an established etiological relationship between P. gingivalis and AMD is confirmed, AMD could join the ranks of diseases—such as obesity, metabolic disorders, and inflammatory bowel diseases—that have been shown to be transmittable through the transfer of dysbiotic microbiome ^31^. In such a scenario, the management of P. gingivalis-related AMD risk could involve the elimination of P. gingivalis from the oral cavity. However, it is worth noting that the composition of the microbiome is highly susceptible to changes influenced by the host microenvironment and diet ^32^. Our analysis (Figure 1) also suggests that maintaining a higher serum level of lutein/zeaxanthin (≥0.35 μmol/L or ≥20 μg/dL), possibly through a healthy diet or the use of the Age-Related Eye Disease Study 2 (AREDS2) supplement ^33–36^, could help modulate the P. gingivalis-related AMD risk. Although studies have demonstrated that lower serum levels of various carotenoids, including zeaxanthin, increase the risk of periodontitis ^37^, and supplemental lutein/zeaxanthin has been shown to be protective against AMD ^36^, it remains to be determined if lutein/zeaxanthin has a direct impact on the P. gingivalis-driven microbiome.
This study boasts several strengths, including its design as a matched case-control study within a representative cohort of the US population. The standardized collection of risk factor information and the use of photographic grading for maculopathy are additional strengths, aiming to minimize the impact of confounding factors and misclassifications. However, it is important to acknowledge certain limitations. The restricted number of AMD cases in our study resulted in insufficient sample sizes for certain analyses. For instance, in our interaction analyses, we only had a sufficient sample size to assess the relationship with serum levels of lutein/zeaxanthin. The cross-sectional nature of the study also poses a limitation in terms of defining temporality. Nevertheless, it’s worth noting that serum P. gingivalis IgG is considered to reflect chronic, intermittent exposure ^14^, and the average age of onset for periodontitis is notably younger than that for AMD ^2^. Additionally, serum levels of lutein/zeaxanthin are considered to reflect the long-term intake of these nutrients ^36^.
In conclusion, our study has unveiled a novel association between exposure to P. gingivalis, serum lutein/zeaxanthin levels, and the risk for AMD. Although the intricate mechanisms underlying this relationship require further investigation, our findings have the potential to significantly influence therapeutic and preventive strategies for AMD. This is particularly noteworthy given the high prevalence of P. gingivalis in the human population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Darveau R. P. Periodontitis: a polymicrobial disruption of host homeostasis. Nat Rev Microbiol. 8, 481–490. (2010).20514045 10.1038/nrmicro 2337 · doi ↗ · pubmed ↗
- 2Burt B. & Research Science and Therapy Committee of the American Academy of Periodontology. Position paper: epidemiology of periodontal diseases. J Periodontol. 76, 1406–1419. (2005).16101377 10.1902/jop.2005.76.8.1406 · doi ↗ · pubmed ↗
- 3Chapple I. L. Time to take periodontitis seriously. BMJ. 348, :g 2645. (2014).24721751 10.1136/bmj.g 2645 · doi ↗ · pubmed ↗
- 4Pussinen P. J. Periodontal pathogen carriage, rather than periodontitis, determines the serum antibody levels. J Clin Periodontol. 38, 405–411. (2011).21362013 10.1111/j.1600-051X.2011.01703.x · doi ↗ · pubmed ↗
- 5Hajishengallis G., Darveau R. P. & Curtis M. A. The keystone-pathogen hypothesis. Nature reviews. Microbiology 10, 717–725, doi:10.1038/nrmicro 2873 (2012).22941505 PMC 3498498 · doi ↗ · pubmed ↗
- 6Boisvert H., Lorand L. & Duncan M. J. Transglutaminase 2 is essential for adherence of Porphyromonas gingivalis to host cells. Proc Natl Acad Sci U S A. 111, 5355–5360. (2014 ).24706840 10.1073/pnas.1402740111 PMC 3986193 · doi ↗ · pubmed ↗
- 7Honda K. Porphyromonas gingivalis sinks teeth into the oral microbiota and periodontal disease. Cell Host Microbe. 10, 423–425. (2011).22100158 10.1016/j.chom.2011.10.008 · doi ↗ · pubmed ↗
- 8Kamer A. R. Inflammation and Alzheimer’s disease: possible role of periodontal diseases. Alzheimers Dement. 4, 242–250. (2008 ).18631974 10.1016/j.jalz.2007.08.004 · doi ↗ · pubmed ↗