Systemic anticancer therapy at the end of life: real-world insights from a tertiary oncology center in Israel
Renana Barak, Esraa Safadi, Alla Nikolaevski-Berlin, Noa Soback, Ido Wolf, Barliz Waissengrin

TL;DR
This study examines aggressive cancer treatments given to patients near the end of life in Israel and finds high rates of such care.
Contribution
The study provides real-world data on systemic anticancer therapy use in advanced cancer patients in Israel, highlighting potential quality-of-care issues.
Findings
36% of patients received systemic anticancer therapy in the last 30 days before death.
Younger age and better performance status correlate with higher end-of-life treatment rates.
Breast cancer patients had notably higher rates of aggressive end-of-life care.
Abstract
Aggressive end-of-life (EOL) care, such as systemic anticancer therapy (SACT) for advanced cancer patients, represents a potential indicator of low-quality care that may deviate from the primary palliative objective of treatment. A retrospective study analyzed consecutive patients with advanced cancers treated at a tertiary oncology center in Israel from January 2019 to December 2022. Demographic and clinical data were examined, with a focus on intravenous (IV) oncologic treatment administration rates at 30 and 90 days before death. The study included 1851 patients who received IV oncologic medications and died during 2019-2022. The median age at death was 69 years, with 51.3% (951) being men. Systemic anticancer therapy administration rates were 36% (666 patients) in the last 30 days and 67.6% (1252 patients) in the last 90 days prior to death. Chemotherapy was the most common EOL…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
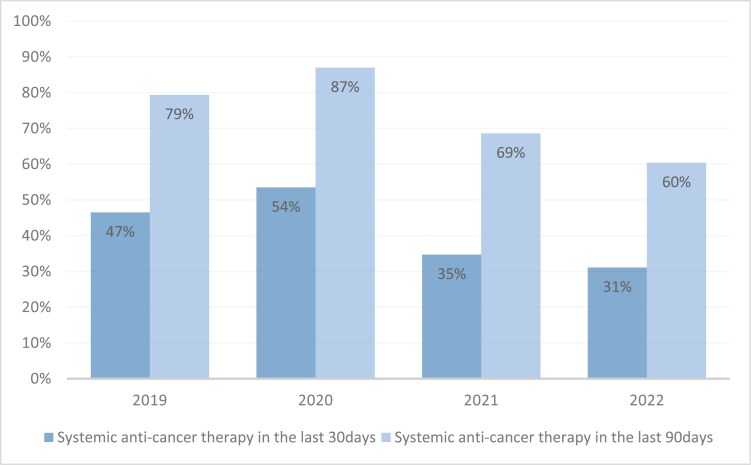 Figure 1
Figure 1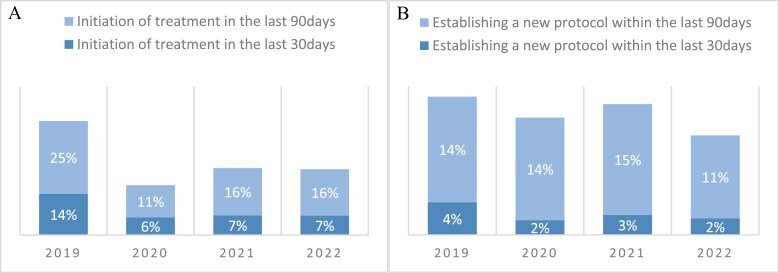 Figure 2
Figure 2| Variable | Value | Count (%) |
|---|---|---|
| Age at diagnosis (median [range], years) | 67 (18-101) | |
| Age at death (median [range], years) | 69 (21-102) | |
| Gender | Male | 951 (51.3) |
| Marital status | Single | 152 (8.2) |
| Married | 1168 (63.1) | |
| Divorced | 308 (16.64) | |
| Widower | 223 (12) | |
| Nationality | Jewish | 1805 (97.5) |
| Arab | 46 (2.5) | |
| ECOG performance status | 0-2 | 1496 (80.8) |
| 3-4 | 308 (16.6) | |
| Oncologic diagnosis | GI malignancies | 708 (38.25) |
| Lung malignancies | 327 (17.67) | |
| CNS malignancies | 141 (7.62) | |
| Breast malignancies | 137 (7.4) | |
| GU malignancies | 132 (7.13) | |
| Gynecologic malignancies | 124 (6.7) | |
| Head and neck malignancies | 58 (3.13) | |
| Other | 224 (12.1) | |
| Type of last treatment | Chemotherapy | 1057 (57.1) |
| Immune-Checkpoint Inhibitors | 278 (15) | |
| Monoclonal Antibodies | 188 (10.2) | |
| Chemotherapy + Monoclonal Antibodies | 158 (8.5) | |
| Clinical Trial | 87 (4.7) | |
| Chemotherapy + Immune-Checkpoint Inhibitors | 58(3.1) | |
| Immune-Checkpoint Inhibitors + Monoclonal Antibodies | 25 (1.4) | |
| Duration of disease (median [Q1, Q3], years) | 1.6 (0.8, 3.4) | |
| Systemic anticancer treatment administration at EOL | 30 days before death | 666 (36%) |
| 90 days before death | 1252 (67.6%) |
| Variable | Value | SACT use in the last 30 days, |
| SACT use in the last 90 days, |
|
|---|---|---|---|---|---|
| Full sample | 666 (36) | 1252 (67.6) | |||
| Age at diagnosis | <55 | 141 (36.1) | .16 | 268 (68.7) | .74 |
| 55-74 | 365 (38) | 653 (68) | |||
| ≥75 | 145 (32.7) | 294 (66.4) | |||
| Gender | Male | 338 (35.5) | .69 | 649 (68.2) | .58 |
| Female | 328 (36.4) | 603 (67) | |||
| Marital status | Single | 59 (38.8) | .37 | 102 (67.1) | .07 |
| Married | 420 (36) | 801 (68.6) | |||
| Divorced | 117 (38) | 215 (69.8) | |||
| Widower | 70 (31.4) | 134 (60) | |||
| Nationality | Jewish | 649 (36) | .87 | 1222 (67.7) | .75 |
| Arab | 17 (37) | 30 (65.2) | |||
| ECOG performance status | 0-2 | 586 (39.1) |
| 1034 (69.1) |
|
| 3-4 | 80 (26) | 195 (63) | |||
| Oncologic diagnosis | GI malignancies | 260 (36.7) |
| 491 (69.3) |
|
| Lung malignancies | 126 (38.5) | 222 (67.9) | |||
| Breast malignancies | 56 (40.9) | 93 (67.9) | |||
| Gynecologic malignancies | 45 (36.3) | 88 (71) | |||
| CNS malignancies | 29 (20.6) | 95 (67.4) | |||
| GU malignancies | 39 (29.5) | 72 (54.5) | |||
| Head and neck malignancies | 24 (41.4) | 45 (77.6) | |||
| Other | 87 (38.8) | 146 (65.2) | |||
| Type of last treatment | mAB | 50 (26.6) |
| 128 (68.1) | .62 |
| CT | 386 (36.5) | 716 (67.7) | |||
| ICIs | 118 (42.4) | 193 (69.4) | |||
| Clinical Trial | 28 (32.2) | 55 (63.2) | |||
| CT + mAB | 56 (35.4) | 99 (62.7) | |||
| ICIs + mAB | 5 (20) | 19 (76) | |||
| CT + ICIs | 23 (39.7) | 42 (72.4) | |||
| Duration of disease | <1 | 306 (52.7) |
| 510 (87.8) |
|
| 1-3.4 | 251 (30.5) | 520 (63.3) | |||
| ≥3.5 | 109 (5.9) | 222 (50) |
| Independent variable | Comparison categories | Odds ratio | 95% CI |
|
|---|---|---|---|---|
|
| 0-2 vs 3-4 | 1.81 | (1.33, 2.44) |
|
|
| <1 year vs 1-3.4 years | 2.92 | (2.29, 3.72) |
|
| <1 year vs ≥3.5 years | 4.95 | (3.61, 6.8) |
| |
| 1-3.4 years vs ≥3.5 years | 1.698 | (1.28, 2.26) |
| |
|
| < 55 vs 55-74 | 1.06 | (0.81, 1.38) |
|
| 55-74 vs ≥75 | 1.66 | (1.28, 2.15) |
| |
| < 55 vs 75+ | 1.75 | (1.28, 2.41) |
| |
|
| mAB vs mAB + ICI | 4.59 | (1.44, 14.49) |
|
| ICI vs mAB | 1.09 | (0.62, 1.94) |
| |
| mAB + CT vs mAB + ICI | 3.48 | (1.17, 10.39) |
| |
| ICI vs CT | 1.45 | (1.06, 2.00) |
| |
|
| Breast vs GI cancer | 2.02 | (1.32, 3.11) |
|
| GI vs CNS Cancer | 1.98 | (1.05, 3.73) |
| |
| Head & Neck vs GI cancer | 1.99 | (1.07, 3.7) |
| |
| Breast vs GU cancer | 2.55 | (1.44, 4.5) |
| |
| Head & Neck vs GU cancer | 2.5 | (1.23, 5.1) |
| |
| Breast vs CNS cancer | 4.01 | (2.05, 7.84) |
| |
| Breast vs Lung cancer | 2.14 | (1.32, 3.45) |
| |
| GYN vs CNS Cancer | 2.5 | (1.2, 5.2) |
| |
| Head & Neck vs CNS cancer | 3.94 | (1.7, 9.1) |
| |
| Head & Neck vs. Lung cancer | 2.1 | (1.1, 4.02) |
| |
|
| Male vs Female | - | - | .646 |
|
| Single vs Married | - | - | .95 |
|
| Jewish vs Arab | - | - | .89 |
| ECOG performance status | Total number of patients | Treatment rates in the last 30 days % ( | Treatment rates in the last 90 days % ( |
|---|---|---|---|
| 0 | 310 | 41% (127) | 68% (212) |
| 1 | 836 | 42% (348) | 71% (593) |
| 2 | 351 | 32% (111) | 65% (229) |
| 3 | 242 | 26% (62) | 64% (156) |
| 4 | 66 | 27% (18) | 59% (39) |
| NA | 47 | 0 (0) | 49% (23) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Childhood Cancer Survivors' Quality of Life · Cancer survivorship and care
Introduction
In recent decades, substantial advancements have reshaped cancer treatment, particularly in the metastatic setting. Novel systemic anticancer therapy (SACT), including chemotherapy, antibody-drug conjugates, biologic targeted therapies, and immune checkpoint inhibitors (ICIs), has shown improved patient survival and quality of life.^1,2^ However, the primary therapeutic focus remains palliative, emphasizing symptom control and overall well-being.^3,4^
Near the end of life (EOL), the use of molecular targeted therapies and immunotherapy is increasing, largely due to their favorable side effect profiles, ease of administration, and potential for long-term benefits compared with traditional chemotherapy.^5-8^ However, these therapies exhibit a distinct but significant toxicity profile, with increased rates of delirium and opioid use observed among patients treated with molecular therapies and ICIs, respectively, at the EOL.^9^ Other studies suggested that the optimism surrounding these treatments can lead patients and physicians to overestimate their efficacy.^7,10,11^
End-of-life oncologic treatments have been associated with adverse outcomes, including increased use of urgent medical services, delayed EOL discussions, reduced hospice enrollment, financial toxicity, and negative impacts on quality of life.^5,7,12^ While these concerns have been well-documented for chemotherapy, recent evidence highlights similar risks for ICI and targeted therapies.
In response, the American Society of Clinical Oncology (ASCO) introduced the “Choosing Wisely” campaign in 2013, providing guidelines to discourage chemotherapy use in late-stage illness. Subsequent updates in 2014 and 2021 expanded these recommendations to include immunological and targeted therapies.^13-15^ Despite these efforts, a significant proportion of advanced cancer patients continue to receive oncologic treatment near the EOL, with up to 38% receiving it within 1 month of death.^4,6,12,16-22^
Robust evidence supports the benefits of early palliative care, particularly in managing symptoms and improving quality of life for cancer patients. Prioritizing palliative care alongside treatment decision-making can help steer EOL care toward a less aggressive trajectory. Some studies even suggest a modest survival benefit with best supportive care alone at EOL.^23,24^ Yet, the appropriateness of early treatment withdrawal is not universally established, as some patients might still derive therapeutic advantages from less intensive medical approaches.
In Israel, the public health system subsidizes medical and oncologic treatments, including biologic therapies and ICI, which are part of the national healthcare basket for advanced cancers.^25-27^ However, the difficulty of predicting patient survival^28-30^ and the challenge of discontinuing active treatment may encourage continued use of these therapies at the EOL. Additionally, while home hospice services have been introduced as part of a national program to improve EOL care, their utilization remains limited. According to 2016 Ministry of Health data, only 6.7 per 1000 individuals aged 65 and over received care in home hospice units, with cancer accounting for 65% of diagnoses.^25^ This highlights a significant gap between service availability and patient needs.
This study aims to explore trends in SACT use at the EOL in Israel, considering recent advancements in treatment options and the evolving healthcare landscape. By analyzing these patterns, we seek to better understand the factors influencing treatment decisions and identify opportunities to optimize EOL care within the healthcare system.
Methods
Study population
We conducted an observational, single center, retrospective cohort study. The study included patients aged 18 years and older with advanced solid malignancies who were treated at the Tel Aviv Sourasky Medical Center (TASMC) oncology department or day care unit and died between 2019 and 2022. Patients were eligible for inclusion if they received intravenous oncologic treatments such as IV chemotherapy, ICIs, or monoclonal antibodies. Patients enrolled in phase 1-3 clinical trials were also included. The exclusion criteria involved administration of oral or intramuscular oncologic treatments at the EOL, as with these routs of administration we were unable to accurately monitor the dates of treatment administration or cessation at home or other ambulatory care settings. Consequently, excluded treatments primarily comprised hormonal therapies and small molecule inhibitors.
Data
Demographic and clinical data were drawn from electronic medical records. Information on age, gender, ethnicity, marital status, oncological diagnosis, ECOG performance status recorded during the most recent oncology clinic visit, duration of disease (from date of diagnosis, based on biopsy date until death), date of death (based on the Population and Immigration Authority), and date and type of last treatment before death (ICI, chemotherapy protocol, biological treatments, clinical trial) were collected. The study was approved by the Helsinki Committee for Clinical Research at TASMC (Helsinki number 1031-20).
Statistical analysis
All explanatory variables (demographic and clinical characteristics of the patients) were characterized by appropriate descriptive measures. We examined the relationship between each of the explanatory variables and receiving oncology treatment in the last 30 days of life and in the last 90 days of life by chi-square test for independence. Logistic regression models were performed to investigate the influence of patients’ demographic (age, gender, marital status, nationality) and clinical characteristics (diagnosis, disease duration, treatment type, ECOG performance status) on the probability of receiving IV SACT in the last 30 and 90 days of life. Continuous variables, such as age at diagnosis and disease duration, were converted into categorical inputs for the regression model, with cutoffs determined according to quartiles of the study population (ie, <25%, 25%-74%, and ≥75%). Among patients receiving chemotherapy at EOL, logistic regression model was performed to investigate the impact of same patients’ clinical and demographic characteristics on the probability of receiving monotherapy regimen during the last 30 days of life. Statistical analysis was performed by SAS 9.4 software.
Results
Out of 21 040 patients that were treated at the TASMC oncology department or day care unit between 2019 and 2022, 1851 patients met the inclusion criteria. The baseline characteristics of these eligible patients are detailed in Table 1. Among them, 951 (51.3%) were men, the median age at death was 69 years (range 21-102), and the majority of patients were Jewish 1805 (97.5%). At the most recent oncology clinic visit, 1497 patients (80.8%) had an ECOG score of 0-2. The most prevalent oncological diagnoses were gastrointestinal (GI) malignancies with 708 cases (38.2%), followed by lung cancer with 327 cases (17.7%), central nervous system (CNS) tumors 141 (7.6%), and breast cancer 137 (7.4%). The median duration of disease, measured from the date of diagnosis (biopsy date) to death, was 1.6 years. The upper quartile included patients with a disease duration exceeding 3.4 years, while the lower quartile comprised patients with a disease duration shorter than 9.6 months. This distribution was subsequently used for subgroup comparisons in the multivariate regression models. Chemotherapy was the most common last treatment administered, occurring in 1057 cases (57.1%), followed by ICI in 278 cases (15%) and monoclonal antibodies (mAB) 188 (10.2%). Notably, only 87 (4.7%) were enrolled in a clinical trial, of whom nearly two-thirds (59 patients) participated in a phase 1 trial, and 1252 patients (67.6%) and 666 patients (36%) received systemic anticancer treatment in the last 90 and 30 days before death, respectively.
Characteristics of patients receiving treatment at EOL
Among 666 patients (36%) treated with systemic anticancer treatment in the last 30 days before death and 1252 patient (67.6%) treated with SACT during their last 90 days, similar distribution of baseline characteristics was seen, as detailed in Table 2. In 30-day time point, 50.7% (338) of treated patients were men, 586 (88%) had an ECOG score of 0-2, and 306 (46%) had disease duration of less than one year. In 90-day time point, 649 (51.8%) were men, 1034 (82.5%) had an ECOG score of 0-2, and disease duration was less than a year for 510 (41%) patients. Looking at disease duration, almost 90% (510) of patients with disease duration of less than a year received SACT in the last 90 days and 52.7% (306) were treated during the last month before death, while patients with disease duration longer the 3.5 years had substantially lower rates of SACT administration at EOL (50% and 6% at 90- and 30-day time points, respectively). Univariate analysis demonstrated significant associations between ECOG performance status score, disease duration, and tumor origin and treatment administration at both 30 and 90-day time points (P <.05 for all). In contrast, demographic variables such as gender, marital status, and ethnicity were not associated with the administration of anticancer treatment at the EOL.
Treatment modalities and protocols at EOL
Chemotherapy (CT) was the most commonly administered treatment, utilized by 386 patients (58%) and 716 patients (57.2%) in 30- and 90-day time points, respectively. At 30-day time point, chemotherapy was followed by ICI (17.7%, n = 118), CT combined with mAB (8.4%, n = 56), mAB alone (7.5%, n = 50), and participation in clinical trials (4.2%, n = 28). Similar distribution was observed at 90 the day time point, except for monoclonal antibodies regimens which were more frequently administered without chemotherapy (10.2%, n = 128) compared with chemotherapy (7.9%, n = 99). However, the type of treatment was significantly associated with treatment administration only at 30-day time point (P =.0135).
Seventy percent (n = 269) of chemotherapy-based regimens administered during the last month before death consisted of multiagent, while only 30% (n = 117) were single agent protocols. A multivariate logistic regression was conducted to assess the influence of clinical variables on the likelihood of receiving single-agent versus multiagent chemotherapy protocols at the EOL. The analysis revealed that longer disease duration was significantly associated with an increased probability of receiving less aggressive treatment, such as single-agent chemotherapy regimen. Patients with a disease duration of 3.5 years or longer had an odds ratio (OR) of 4.7 for single agent protocol compared with those with the duration of less than 1 year (95% CI, 2.33-9.28, P =.0005) and OR of 1.92 compared with disease duration of 1-3.4 years (95% CI, 1.0-3.7, P =.05). Additionally, tumor origin significantly influenced the likelihood of single-agent chemotherapy. Patients with lung cancer and GI malignancies were more likely to receive single-agent compared with those with gynecologic cancers (OR = 2.95, 95% CI, 1.08-8.06, P =.035; OR = 1.20, 95% CI, 0.47-3.07, P =.036, respectively). In contrast, age, gender, marital status, nationality, and ECOG score did not demonstrate a significant association with single-agent treatment receipt.
Predictors of anticancer treatment administration at EOL
Using multivariate model, the probability of receiving oncologic treatment within the 30 days preceding death was significantly influenced by 4 independent clinical variables: ECOG PS score, disease duration, age, and tumor origin (Table 3). Patients with ECOG performance status score of 0-2 had an OR of 1.81 relative to those with scores of 3-4 (95% CI, 1.33-2.44, P <.0001). Additionally, patients with a disease duration of less than 1 year exhibited markedly higher probabilities of receiving treatment, with ORs of 2.92 (95% CI, 2.29-3.72, P =.0127) and 4.95 (95% CI, 3.61-6.80, P <.0001) when compared with individuals with durations of 1-3.4 years and 3.5 years or more, respectively. Younger patients had higher probability for treatment at EOL, patients under 55 years old and 55-74 had ORs of 1.75 (95% CI, 1.28-2.41, P <.0001) and 1.66 (95% CI, 1.28-2.15, P <.0001) in comparison to 75 years and older, respectively. Furthermore, patients receiving ICIs had 45% higher probability for treatment at 30 days before death compared with patients treated with chemotherapy (OR 1.45, 95% CI, 1.06-2.00, P =.02). Breast cancer patients had over twice the probability of receiving systemic anticancer treatment in the last 30 days compared with individuals with GI, GU, and lung origin (OR 2.02, 2.55, and 2.14, respectively) and a 4-fold greater risk compared with those with CNS malignancies (OR 4.01, 95% CI, 2.05-7.84, P <.0001). Treatment administration in the last 90 days before death was similarly influenced by shorter disease duration, younger age at diagnosis and tumor origin, with breast cancer consistently exhibiting higher treatment rates compared with GI, GU, and lung cancers (Supplementary Table 1).
Rate of treatment administration
In a year-by-year analysis (Figure 1), the lowest rates of EOL SACT in both groups (last 30 days and 90 days) was in 2022 (31.1% and 60.4%, respectively), and the highest rate were in 2020 (53.5%, 87%).
Rate of systemic anticancer therapy administration in last 30 and 90 days of life, by year.
Adjustments and initiations treatment
During the last 30 days of their lives, 50 patients (2.7%) had their treatment protocol modified, while 141 (7.6%) patients began receiving systemic anticancer treatment for the first time. In the last 90 days of life, 244 (13.2%) patients underwent a change in their treatment protocol, and 312 (16.8%) initiated systemic anticancer therapy for the first time during this period. Figure 2 illustrates trends regarding the establishment of new protocols and the initiation of treatment among patients in the final 30 and 90 days of life, categorized by year.
Rate of first-line therapy initiation at last 30 days and last 90 days of life, by year (A), rate of initiation of subsequent line of treatment at the last 30 and 90 days of life, by year (B).
Performance status and aggressiveness of care
Analysis of systemic anticancer therapy administration by categories of ECOG performance status revealed that patients with performance status 0 or 1 had, as expected, the highest rates of receiving treatment (Table 4). Specifically, of all patients with performance status 0, 41% received systemic therapy in the last 30 days before their death an 68% in the last 90 days before their death. For patients with performance status 1, the percentages were 42% and 71%, respectively, for the same time periods.
Discussion
The findings of this study provide critical insights into the patterns of systemic anticancer treatment administration at the EOL, particularly in light of the evolving landscape of oncologic therapies. Among the 1851 eligible patients, a significant number received treatment in the final phases of their lives, highlighting a trend toward continued oncologic interventions even when the primary goal shifts to palliative care.
Notably, 36% of patients received systemic anticancer treatment within the last 30 days before death, nearly two-thirds (67.6%) of patients received treatment in the last 90 days before death, with chemotherapy being the most common modality in both time points. The study revealed that ECOG performance status, disease duration, age, and tumor origin were significant predictors of treatment likelihood. Higher rates of treatment were observed in younger aged patients, with an ECOG score of 0-2, and those with shorter disease durations, emphasizing the complex relationship between health status and therapeutic decisions at the EOL.
The observed rate of 36% of patients receiving SACT within 30 days of death in this study was notably higher than most previously reported rates, which ranged from 2.2% to 22.5% in various international studies.^4,6,16-20,22^ However, this rate aligns closely with Canavan et al.’s findings of 39% and Auclair et al.’s report of 38%, suggesting that higher rates of EOL SACT administration may be more common in recent years, particularly with the advent of immunotherapy and targeted treatments.^12,21^ The rate of systemic treatment in the last 90 days before death was 67.6%, consistent with literature ranging from 56% to 67%.^7,31^ Possible explanation to the more aggressive treatment given at our institution could be the central location with high population density allowing easy access to healthcare, availability of advanced treatments subsidized by the state, religious and cultural norms emphasizing fighting the disease, and simultaneous provision of palliative treatments alongside anticancer therapies.
In this study, 40.9% of breast cancer patients received IV anticancer treatment within 30 days of death. These patients exhibited significantly higher treatment rates, with OR ranging from 2.02 to 4.01 compared with other cancer types such as lung, CNS, GU, and GI malignancies. This finding is consistent with existing literature that indicates high rates of aggressive EOL treatment for metastatic breast cancer.^32^ However, our study excluded patients receiving oral therapies, which may have unintentionally led to the inclusion of individuals with more aggressive disease subtypes such as hormone-resistant, HER2-positive, and triple-negative breast cancer. This population often experiences shorter disease durations and is generally younger in age.
Albeit the observed inverse correlation between ECOG PS score and utilization of EOL anticancer treatment, which aligns with the ASCO guidelines against administration of anticancer treatment in patients with poor performance status.^14,15^ Over one-quarter of patients with ECOG PS score of 3 and 4 (26% and 27%, respectively) received treatment in the last 30 days of life. Yet, only 16.6% (308 patients) of our study population had ECOG PS score of 3-4. These high rates of oncologic treatment administration could be influenced by the relatively small sample size, but together with the generally high rates of treatment among the entire study population, most likely suggest an aggressive approach with a significant financial burden on the health care system^13^ and probably futile regarding quality of life.^33,34^
Following the outbreak of the COVID-19 epidemic, studies have demonstrated a correlation between cancer morbidity and an increased risk of mortality from the coronavirus.^35^ This finding helps to explain the relationship observed in our study between the administration of anticancer treatment at EOL and the year in which the treatment was administered. With 2020, the year of epidemic break, exhibiting the highest rates of therapy during both timepoints examined (last 30 and 90 days of ones’ life). This trend is likely attributed to the fact that patients who died during the epidemic year were in a more critical condition and sought treatment in hospitals despite the imposed restrictions.
Despite the global trend toward increased use of ICIs and TTs near the EOL, often as part of precision medicine guided by tumor molecular profiling and following standard-of-care treatments, along with a decline in chemotherapy use,^5,12^ in our study, chemotherapy remained the most commonly administered treatment at EOL. A possible explanation could be the subsidy of treatment. In cases when novel “expansive” oncologic medications are not provided by the national health care basket, chemotherapy is typically subsidized and offered free of charge. With regards to cultural norms such as fighting the disease, personal views and values, and general difficulty of therapy cessation, choices of patients and caregivers around the EOL are not a consequence of medical decisions based on evidence-based medicine alone. Therefore, most patients continue chemotherapy provided earlier and 10% even started a new line of treatment at 30 days from death.
It is vital to recognize that the evidence does not conclusively support universal early treatment withdrawal, as some patients may still benefit from less aggressive oncologic therapies. The key challenge lies in identifying the potentially small subset of patients who could derive such benefit. In our study, multiagent chemotherapy protocols dominated (69.6%) in patients’ final 30 days of life. Notably, patients with longer disease trajectories and specific tumor types, particularly lung and GI malignancies, showed a higher likelihood of receiving less aggressive single-agent therapy. These findings emphasize the critical importance of nuanced patient selection and personalized treatment strategies during EOL care.
Palliative care in Israel has progressed significantly since its first modern hospice in 1983, with legislative support in 2005 and recognition as a subspecialty in 2012. Despite these advancements, a considerable gap remains between available services and patient needs. In 2015, a palliative care unit was established at Tel-Aviv Sourasky Medical Center, gaining recognition as a specialization center in 2022. The unit is closely integrated with the Oncology division. However, our study’s lack of hospice care implementation data limits our understanding of its impact on palliative and oncologic outcomes.
The study’s limitations, include those arising from its design being retrospective, the study was limited to a single medical center and the high level of ethnic homogeneity of the study population. Additionally, it is important to consider the timing of data collection, which coincided with the outbreak of the COVID-19 epidemic. During this period, patients may have reduced their in-person interactions, resulting in decreased meetings with the healthcare team and potential alterations in treatment receipt. This could introduce confounding factors that might influence the outcomes observed. Our study has several strengths—the large sample size, the collection of extensive demographic data, and the participation of patients who were treated by multiple doctors, who provided different insight and took treatment decisions, an advantage arising from the fact that TLVMC is a tertiary medical center.
In conclusion, our study demonstrates that, in the absence of regulatory measures or financial constraints, aggressive EOL treatments are likely to persist. Awareness of different treatment options along the way is imperative for healthcare providers, and acknowledgment of the concept of “a good death” is essential when making decisions for terminal cancer patients. Additionally, we suggest that health care professionals around the world continue to learn, research, and ask questions about the necessity of anticancer therapy at EOL, to the individual patient and to the system as a whole. Our results may imply that EOL SACT do not meet doctors’ expectations as well as patients’ care-wishes.
Supplementary Material
oyaf066_suppl_Supplementary_Tables_1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lundberg FE , Andersson TML, Lambe M, et al Trends in cancer survival in the Nordic countries 1990–2016: the NORDCAN survival studies. Acta Oncol.2020;59:1266-1274. https://doi.org/10.1080/0284186 x.2020.182254433073632 · doi ↗ · pubmed ↗
- 2Bright CJ , Lawton S, Benson S, et al Data resource profile: the Systemic Anti-Cancer Therapy (SACT) dataset. Int J Epidemiol.2020;49:15-15l. https://doi.org/10.1093/ije/dyz 13731340008 PMC 7426029 · doi ↗ · pubmed ↗
- 3Vanbutsele G , Pardon K, Van Belle S, et al Effect of early and systematic integration of palliative care in patients with advanced cancer: a randomised controlled trial. Lancet Oncol.2018;19:394-404. https://doi.org/10.1016/S 1470-2045(18)30060-329402701 · doi ↗ · pubmed ↗
- 4Wadhwa D , Hausner D, Popovic G, et al Systemic anti-cancer therapy use in palliative care outpatients with advanced cancer. J Palliat Care.2021;36:78-86. https://doi.org/10.1177/082585972097594933241732 · doi ↗ · pubmed ↗
- 5Kerekes DM , Frey AE, Prsic EH, et al Immunotherapy initiation at the end of life in patients with metastatic cancer in the US. JAMA Oncology. 2024;10:342-351. https://doi.org/10.1001/jamaoncol.2023.602538175659 PMC 10767643 · doi ↗ · pubmed ↗
- 6Nguyen M , Ng Ying Kin S, Shum E, et al Anticancer therapy within the last 30 days of life: results of an audit and re-audit cycle from an Australian regional cancer centre. BMC Palliative Care. 2020;19:14. https://doi.org/10.1186/s 12904-020-0517-331987038 PMC 6986019 · doi ↗ · pubmed ↗
- 7Glisch C , Saeidzadeh S, Snyders T, et al Immune checkpoint inhibitor use near the end of life: a single-center retrospective study. J Palliat Med.2020;23:977-979. https://doi.org/10.1089/jpm.2019.038331702481 · doi ↗ · pubmed ↗
- 8Grivas P , Plimack ER, Balar AV, et al Pembrolizumab as first-line therapy in cisplatin-ineligible advanced urothelial cancer (KEYNOTE-052): outcomes in older patients by age and performance status. Eur Urol Oncol.2020;3:351-359. https://doi.org/10.1016/j.euo.2020.02.00932423837 PMC 8246631 · doi ↗ · pubmed ↗