Survival outcomes and clinical characteristics of brain metastases from prostate cancer: A single-center analysis
Kurl Jamora, Adeodatus Vito Nicanor, Ayah Erjan, Marc Vincent Barcelona, Dana Keilty, Michael Yan, Aristotelis Kalyvas, Marc Bernstein, Paul Kongkham, Gelareh Zadeh, Eshetu Atenafu, Srinivas Raman, Alejandro Berlin, Charles Catton, Peter Chung, Barbara-Ann Millar

TL;DR
Brain metastases from prostate cancer are rare and occur in advanced cases, often with other metastases and poor survival outcomes.
Contribution
This study provides a detailed analysis of clinical features and survival outcomes for a rare condition: brain metastases from prostate cancer.
Findings
Median overall survival after brain metastasis diagnosis was 9.4 months.
Most patients had castrate-resistant prostate cancer and concurrent metastases.
Treatment modality did not significantly affect survival outcomes.
Abstract
Brain metastases (BrM) from prostate cancer (PC) are rare. This study sought to evaluate their prevalence, clinical features, treatment modalities, and survival outcomes. From a database of BrM patients, we analyzed 28 cases of prostate cancer treated at our center between 2008 and 2023. BrM from PC comprised 0.7% of cases. The majority of patients had high-risk features at PC diagnosis: median prostate-specific antigen (PSA) at diagnosis was 65.5 ng/ml (range: 3.9–784.7 ng/ml), 82% were Gleason grade group ≥ 4, and 68% had perineural invasion (PNI). At BrM diagnosis, 79% were castrate-resistant. Most patients had concurrent metastases, including bone (94%), lymph nodes (63%), or lung (6%). Fifty percent presented with a single brain lesion, and the median Graded Prognostic Assessment (GPA) score was 1.5 (range: 0.5–2.5). Patients commonly had radiographic brain edema (57%) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
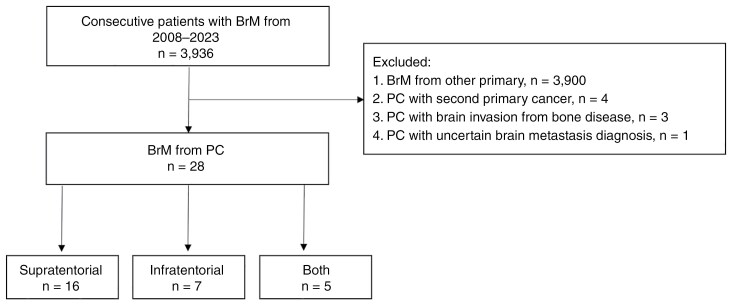 Figure 1
Figure 1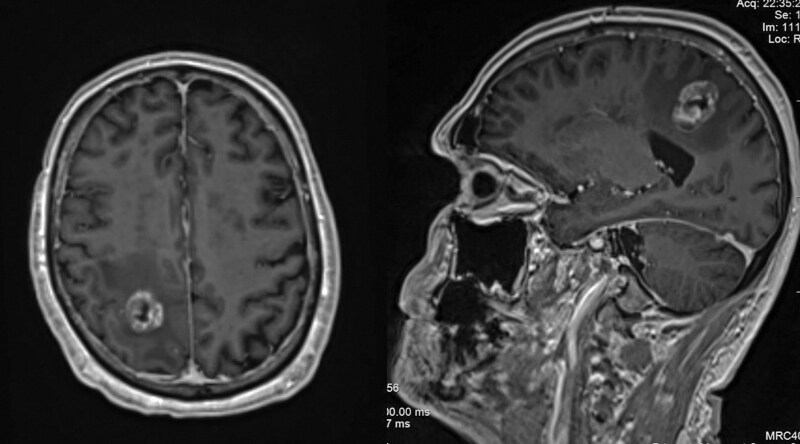 Figure 2
Figure 2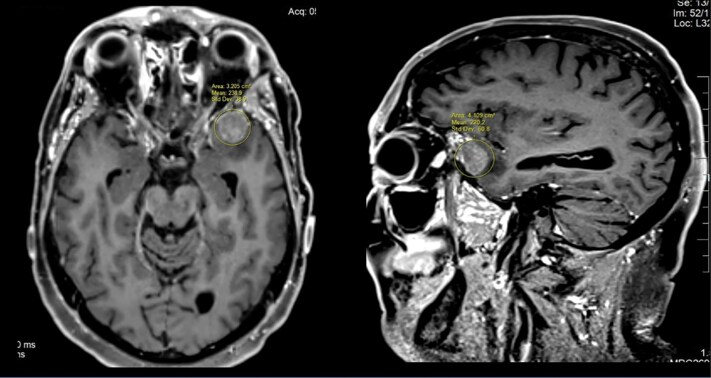 Figure 3
Figure 3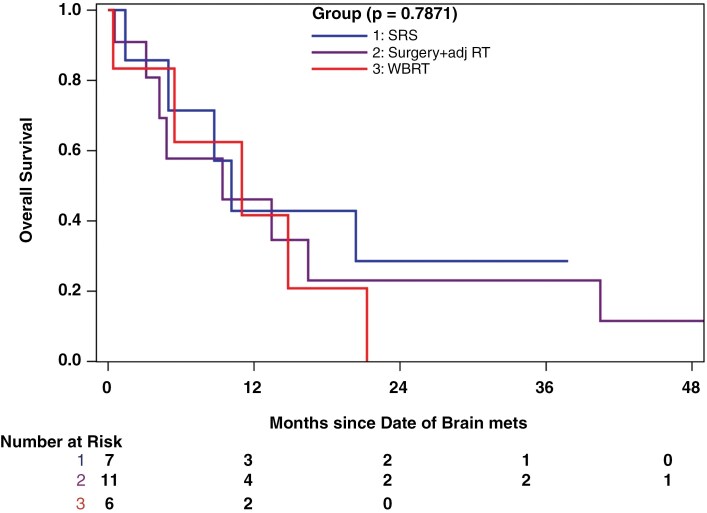 Figure 4
Figure 4|
| |
| Age at diagnosis | |
| Mean (SD) | 63.6 (8.5) |
| Median (Range) | 62.6 (51.0, 81.4) |
| PSA at diagnosis | |
| Mean (SD) | 130.1 (195.5) |
| Median (Range) | 65.5 (3.9, 784.7) |
| Gleason score, | |
| 7 | 5 (17.9%) |
| 8 | 12 (42.9%) |
| 9 | 10 (35.7%) |
| 10 | 1 (3.6%) |
| Perineural invasion, | |
| Yes | 17 (68.0%) |
| No | 8 (32.0%) |
| Missing | 3 |
| Distant metastasis at diagnosis, | |
| Yes | 15 (53.6%) |
| No | 13 (46.4%) |
| Extracranial disease, | |
| Absent | 2 (7.1%) |
| Present | 26 (92.9%) |
| Bone metastasis, | |
| Yes | 15 (93.8%) |
| No | 1 (6.3%) |
| Missing | 12 |
| Lung metastasis, | |
| Yes | 1 (6.3%) |
| No | 15 (93.8%) |
| Missing | 12 |
| Lymph node metastasis, | |
| Yes | 10 (62.5%) |
| No | 6 (37.5%) |
| Missing | 12 |
| CSPC or CRPC, | |
| CSPC | 6 (21.4%) |
| CRPC | 22 (78.6%) |
| Number of BrM at diagnosis, | |
| 1 | 14 (50.0%) |
| 2 | 4 (14.3%) |
| 3 | 2 (7.1%) |
| 4 | 4 (14.3%) |
| 5 | 1 (3.6%) |
| 6 | 1 (3.6%) |
| 10+ | 2 (7.1%) |
| Months from PC diagnosis to BrM | |
| Mean (SD) | 77.8 (73.4) |
| Median (Range) | 47.8 (0.1, 240.9) |
| ECOG at BrM diagnosis | |
| 0 | 3 (10.7%) |
| 1 | 15 (53.6%) |
| 2 | 6 (21.4%) |
| 3 | 4 (14.3%) |
| Total GPA score | |
| Mean (SD) | 1.4 (0.6) |
| Median (range) | 1.5 (0.5, 2.5) |
| Neurological symptoms, | |
| No | 13 (46.4%) |
| Yes | 15 (53.6%) |
| Brain edema, | |
| No | 12 (42.9%) |
| Yes | 16 (57.1%) |
| Seizures, | |
| No | 26 (92.9%) |
| Yes | 2 (7.1%) |
| Systemic therapy at BrM diagnosis, | |
| Yes | 23 (82.1%) |
| No | 5 (17.9%) |
| Type of BrM, | |
| Pure intraparenchymal BrM | 12 (42.9%) |
| Pure dural BrM | 15 (53.6%) |
| Both intraparenchymal and dural BrM | 1 (3.6%) |
| Location of BrM, | |
| Supratentorial only | 16 (57.1%) |
| Infratentorial only | 7 (25.0%) |
| Both supratentorial and infratentorial | 5 (17.9%) |
| Type of BrM treatment, | |
| SRS | 7 (25.0%) |
| WBRT | 6 (21.4%) |
| Posterior fossa radiotherapy | 2 (7.1%) |
| Surgery + SRS/VMAT | 7 (25.0%) |
| Surgery + WBRT | 4 (14.3%) |
| Palliative care | 2 (7.1%) |
| Unadjusted HR (95%CI) |
| Adjusted HR (95%CI) |
| |
|
| 0.8394 | 0.3610 | ||
| SRS/WBRT/PFRT | Reference | Reference | ||
| Surgery + RT | 0.91 (0.36, 2.31) | 1.73 (0.53, 5.60) | ||
|
| 1.02 (0.97, 1.07) | 0.5376 | ||
|
| 1.05 (0.90, 1.22) | 0.5433 | ||
|
|
| 0.5673 | ||
| 0 | Reference | Reference | ||
| 1 | 0.55 (0.15, 2.06) | 0.3782 | 0.29 (0.05, 1.63) | 0.1595 |
| 2 | 0.70 (0.15, 3.33) | 0.6577 | 0.26 (0.03, 2.11) | 0.2089 |
| 3 | 1.70 (0.33, 8.69) | 0.5254 | 0.34 (0.04, 3.26) | 0.3476 |
|
| 0.49 (0.23, 1.05) |
| 0.37 (0.13, 1.09) |
|
|
| 0.8586 | |||
| Present | Reference | |||
| Negative | 0.83 (0.11, 6.30) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBrain Metastases and Treatment · Prostate Cancer Treatment and Research · Radiopharmaceutical Chemistry and Applications
Brain metastases (BrM) are commonly observed and extensively studied in lung, melanoma, and breast cancers.^1–3^ Conversely, prostate cancer (PC) rarely metastasizes to the brain. Limited retrospective reviews and institutional reports have documented its incidence between 0.16% and 8.06%.^4^ Advancements in brain imaging and more effective treatment options for PC and BrM may alter their incidence rates and clinical outcomes, underscoring the necessity for further research on this uncommon phenomenon. This study aims to assess the prevalence, clinical characteristics, treatment options, and survival outcomes of BrM from PC.
Methods
Patients
From a prospectively maintained database of BrM patients at Princess Margaret Cancer Centre, covering treatments from January 2008 to December 2023, we identified patients with histologically proven PC and excluded those with second primary cancers or parenchymal invasion from adjacent skull-based disease. We determined patient demographics, clinical details on PC and BrM diagnosis, and clinical outcomes.
Statistical Analysis
Categorical variables, such as perineural invasion, distant metastasis at diagnosis, bone metastasis, lung metastasis, lymph node metastasis, ECOG at BrM diagnosis, neurological symptoms (eg, headache, nausea, vomiting, sensorimotor deficits, or seizures caused by edema or intracranial pressure changes), brain edema, seizures, systemic therapy at BrM diagnosis, type of BrM, location of BrM, and type of BrM treatment, were presented as counts and percentages. BrM types were categorized as pure parenchymal metastases (confined to the brain parenchyma without involvement of the pachymeningeal dura), pure dural metastases (originating from the pachymeningeal dura without bony skull involvement), and both (involving both intraparenchymal and dural sites). Continuous variables such as age at diagnosis, total GPA score, as well as follow-up were presented as medians with ranges.
The main outcome variable of interest includes time to death (OS). Time to death was calculated in months from the BrM diagnosis (Date of Brain Mets) to the date of death or to the date of the last follow-up, whichever comes first. Overall survival rates were calculated using the Kaplan–Meier product-limit method and the log-rank test was used to assess the impact of covariates of interest on OS. The Cox proportional hazards model was used to obtain HR rates with 95% CI. All P-values will be 2-sided and for the statistical analyses, P < .05 will be considered to indicate a significantly different result. Statistical analyses will be performed using SAS version 9.4 of the SAS system for Windows (Copyright © 2002-2012 SAS Institute, Inc., Cary, NC. USA).
Results
Proportion of Brain Metastases from Prostate Cancer
Of the 3,936 patients with BrM seen at our institution between January 2008 and December 2023, 36 had PC. Of these patients, 4 had a second primary cancer, 3 had skull-based metastasis with adjacent parenchymal invasion, and 1 had an uncertain diagnosis of BrM, which could potentially be a meningioma (Figure 1). Following multidisciplinary discussion, consensus based on imaging suggested meningioma for the latter patient, leading to a decision for observation. The proportion of BrM originating from PC is therefore 0.7% (28 out of 3936) with 11 (39.3%) of these being pathologically confirmed. More than half (15, 54%) presented with neurologic symptoms, while the remainder were incidentally discovered on imaging.
Flow diagram summarizing patient selection. BrM: brain metastasis; PC: prostate cancer.
Patient and Tumor Characteristics
Patient and disease characteristics of the 28 patients included in the study are listed in Table 1. The median age at BrM diagnosis was 63 years (range: 51–81 years). All patients had adenocarcinoma histology. At the time of PC diagnosis, median prostate-specific antigen (PSA) was 65.5 ng/ml (range: 3.9–784.7 ng/ml). All had a Gleason score of ≥ 7, and a majority of 23 (82%) had a Gleason score of ≥ 8. The majority of patients (17, 68%) had perineural invasion, and 15 (54%) presented with de novo metastatic disease. At the time of BrM diagnosis, 22 patients (79%) were castrate-resistant. BrM diagnosis occurred at a median of 47.8 months (range: 0.1–241 months) from PC diagnosis. Most had concurrent metastases, including bone 15 (94%), lymph nodes 10 (63%), or lung 1 (6%), and 23 (82%), were receiving systemic therapy. Most of the patients (16, 64%) had an ECOG performance status of 0–1. Fifty percent of patients (14) presented with a single brain lesion, and the median Graded Prognostic Assessment (GPA) score was 1.5 (range: 0.5–2.5). Patients had either pure intraparenchymal metastasis (n = 12, 42.9%, see Figure 2), pure dural metastasis (n = 15, 53.6%, see Figure 3), or both (n = 1, 3.6). Metastases were supratentorial only in 16 (57%) patients, infratentorial only in 7 (25%), and both supratentorial and infratentorial in 5 (18%). Patients commonly had neurological symptoms (15, 54%) and brain edema on imaging (16, 57%), whereas only 2 (7%) had seizures.
Intraparenchymal brain metastasis. Axial and sagittal T1-weighted MR images showing a heterogeneous enhancing metastasis in the right posterior semiovale, accompanied by surrounding vasogenic edema.
Purely dural-based metastasis. Axial and sagittal T1-weighted MR images showing an enhancing dural-based mass in the anterior left middle cranial fossa. The lesion does not involve the overlying skull.
Survival
All 28 patients were analyzed for treatment and survival outcomes. Patients received the following treatments: stereotactic radiosurgery (SRS) (n = 7), whole brain radiotherapy (WBRT) (n = 6), surgery followed by adjuvant radiotherapy (n = 11), posterior fossa radiotherapy (PFRT) (n = 2), and palliative care (n = 2) (Table 1). The median follow-up since the diagnosis of brain metastases (BrM) was 7 months (range: 0.4–55.4 months). The median overall survival (OS) after BrM diagnosis was 9.4 months (95% CI: 4.8–14.8 months).
Univariate analysis revealed that the type of BrM treatment, age, number of BrM at diagnosis, ECOG status, and presence of extracranial disease were not significantly associated with improved OS. When OS was further stratified at 6, 12, and 18 months, analyzing single vs. multiple BrMs and CSPC vs. CRPC, no significant associations were found (Supplementary Tables S1 and S2). However, the total GPA score showed a trend toward significance (P = .07). Multivariable analysis further supported this finding, showing an upward trend in OS with higher GPA scores (P = .07) (Table 2).
Treatment modalities—surgery plus adjuvant radiation (9.4 months), SRS (10.1 months), or WBRT (11.0 months)—showed no significant difference in median survival (P = .79) (Figure 4). Although the median survival for patients with a single BrM (10.1 months) was higher than for those with multiple BrM (2.8 months), this difference did not reach statistical significance (P = .79). Likewise, median survival did not significantly differ between patients with castrate-sensitive prostate cancer (CSPC) (5.0 months) and those with castrate-resistant prostate cancer (CRPC) (10.1 months) (P = .69).
Overall Survival Distribution by Brain Metastasis Treatment Modality. RT: radiotherapy; SRS: stereotactic radiosurgery; WBRT: whole brain radiotherapy
Discussion
This 16-year retrospective review reveals a 0.7% incidence of BrM from PC, aligning with findings from similar retrospective series and underscoring their rarity within this patient demographic.^5–10^ However, the incidence rate might be influenced by the study’s institutional scope rather than a broader population-based approach. In addition, the patient sample in this study was only derived from a prospective database of patients referred to the BrM clinic by various subspecialty clinics. This may exclude some patients not referred by the genitourinary clinic and were managed independently instead, potentially introducing a selection bias. Unlike the MD Anderson Cancer Center (MDACC) study,^7^ which incorporated autopsy reports—identifying 60% of PC BrM cases post-mortem—our review’s exclusion of such reports likely underestimates asymptomatic BrM instances only discoverable at autopsy. The use of magnetic resonance imaging (MRI) for screening could potentially identify smaller, asymptomatic BrM, suggesting a possibly higher incidence rate than currently reported. However, the frequency with which MRIs are utilized for screening asymptomatic PC patients is not known in our study.
While some studies on prostate cancer with brain metastases excluded cases with dural-based disease, our review included both dural-based and purely parenchymal metastases. We identified a predominance of purely dural-based brain metastases from prostate cancer, accounting for 54% of the cases. In our study, skull-based metastases and dural-based metastases were distinguished using brain MRI, with the former showing involvement of the skull cortex and the latter limited to the pachymeningeal dura without bony involvement. Leptomeningeal metastases, on the other hand, were identified by enhancement or sugar coating pattern, typically observed in the cortical sulci or cerebellar folia.^11^ This contrasts with findings from a study conducted in Turkey,^5^ which reported a 20% incidence of pure dural-based disease, and the MDACC study, which reported an incidence of 21%.^7^ The overall incidence of BrM in the Turkish study was 2.9%, whereas the MDACC study reported an incidence of 0.8%. In our study, the overall incidence of pure-dural-based BrM is 0.38% (15 per 3,936 patients), while the incidence of pure intraparenchymal BrM is 0.30% (12 per 3,936 patients).
Understanding the pathways through which PC metastasizes—either hematogenously via the vena cava or retrogradely through the valveless Batson’s plexus—sheds light on its potential to reach distant sites, including the brain.^12,13^ Retrospective studies have shown certain PC histologies, such as small cell carcinoma (SCC) and neuroendocrine subtypes, are more prone to BrM, mirroring the metastatic behavior of SCC from lung cancer.^6,7,14,15^ In contrast, our study found only adenocarcinoma histology in all patients, with no instances of SCC or other rare subtypes. In an analysis of BrM from PC of purely adenocarcinoma origin by Bhambhvani et al., the proportion of BrM from PC is 0.86%, a rate that closely parallels the incidence found in our study.^10^
Consistent with prior reports, our study found that BrM from PC predominantly occurred in patients presenting with high-risk features such as elevated PSA levels at diagnosis, advanced Gleason scores, PNI, castrate resistance, and synchronous metastases in other organs.^5–7,10,16^ Furthermore, the median interval between PC diagnosis and BrM detection—47.8 months—parallels findings from other studies.^5,6,14,17,18^ This pattern underscores the potential need for targeted BrM screening strategies at a certain time point in patients with these high-risk features. The majority of patients do exhibit symptoms, however, typically presenting with at least one non-focal symptom, whereas seizures are uncommon. This highlights the complexity of BrM symptomatology in PC and further supports the rationale for regular monitoring in this patient population. The true incidence of brain metastases from prostate cancer is likely underestimated, as evidenced by the MDACC study, where 78 cases were diagnosed via autopsy compared to 53 identified through imaging. Improved survival rates in prostate cancer may contribute to a rising incidence of brain metastases. For instance, a study by Caffo et al. reported an increase in brain metastases from 0.8% to 2.8% following the introduction of docetaxel, with most cases occurring after patients developed castration-resistant disease.^17^ Currently, no published guidelines exist on how to screen for brain metastases in high-risk prostate cancer patients. However, the increasing use of prostate-specific membrane antigen positron emission tomography (PSMA-PET) has shown promise in detecting incidental brain lesions.^19–22^ Equivocal findings on PSMA-PET could then be further evaluated with MRI for detailed characterization. This approach seems reasonable for monitoring high-risk patients.
The median survival in our study was 9.4 months, which is higher than most institutional retrospective analyses reporting 2.8–5.5 months.^5–10^ Population-based database studies have reported longer median survivals of 10–12 months.^23,24^ Specifically, our study identified a median survival of 10.1 months in BrM patients treated with SRS, comparable to the MDACC study’s 9 months.^7^ Another study involving patients exclusively treated with Gamma Knife SRS reported a median survival of 13 months.^14^ Notably, in our study, the SRS group exhibited a relatively higher 6-month survival rate compared to other groups (SRS: 71.4%; surgery and adjuvant RT: 57.7%; WBRT: 62.5%), although this advantage did not extend beyond 12 months (Supplementary Table S3). Patients in our study treated with WBRT had a median survival of 11 months, higher than the 2–7 months reported in other retrospective studies.^5,8,25,26^ Nonetheless, these comparisons are limited by our study’s small sample size and the variations in the time periods during which patients were treated, potentially affecting the availability of diagnostic and treatment modalities. At our center, the decision to administer WBRT was guided by the number of brain metastases and the patient’s performance status. Regarding stereotactic treatment, fractionated SRS was introduced in 2017, particularly for large brain metastases, whereas single-fraction SRS was the standard practice prior to 2017. Detailed information on dose, volume, and fractionation has been previously described.^27^
Our study did not identify any patient or treatment-related factors that significantly correlated with OS. However, a higher GPA score showed a trend toward improved OS. The GPA is a well-established prognostic index for patients with brain metastases. Over time, the GPA has been refined with diagnosis-specific prognostic indices for breast cancer, small cell and non-small cell lung cancer, gastrointestinal cancer, melanoma, and renal cell carcinoma.^28^ The rarity of BrM from PC may make it challenging to identify prognostic factors specific to this disease. Nonetheless, the trend toward improved OS with a higher generic GPA score is noteworthy. Future studies in larger patient groups should investigate disease-specific factors that could potentially predict outcomes for this group of patients.
This study has several limitations. Firstly, it is a retrospective analysis conducted at a single tertiary center, which may introduce selection bias. PC patients with BrM who were not referred to the BrM Clinic for management were not included, potentially skewing the data. In addition, autopsy reports were not incorporated. The low incidence of BrM from PC resulted in a small sample size, limiting the ability to draw definitive conclusions regarding predictive factors for OS. To address these limitations, future research should include longitudinal studies with long-term follow-up to help identify late-emerging prognostic factors and trends. Investigating genetic and molecular markers may uncover novel prognostic factors specific to PC patients. Ultimately, future studies should aim to develop a disease-specific GPA for PC patients with BrM to improve prognostic accuracy and guide treatment decisions.
Conclusion
BrM from PC are rare, predominantly occurring in patients with advanced, castrate-resistant stages, and are often accompanied by other metastases. This analysis aids in understanding the disease trajectory and informing treatment discussions. Despite the rarity and the challenges in identifying specific prognostic factors, the study highlights the potential role of the GPA as a prognosis tool to estimate OS. Future research should focus on longitudinal studies with long-term follow-up to identify late-emerging prognostic factors.
Supplementary Material
vdaf063_suppl_Supplementary_Table_S1
vdaf063_suppl_Supplementary_Table_S2
vdaf063_suppl_Supplementary_Table_S3
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gavrilovic IT , Posner JB. Brain metastases: epidemiology and pathophysiology. J Neurooncol.2005;75(1):5–14.16215811 10.1007/s 11060-004-8093-6 · doi ↗ · pubmed ↗
- 2Eichler AF , Loeffler JS. Multidisciplinary management of brain metastases. Oncologist.2007;12(7):884–898.17673619 10.1634/theoncologist.12-7-884 · doi ↗ · pubmed ↗
- 3Gutiérrez-Valencia E , Sánchez-Rodríguez I, Balderrama-Ibarra R, et al Diagnosis and management of brain metastases: an updated review from a radiation oncology perspective. J Cancer Metastasis Treat. 2019;5:54.
- 4Rajeswaran K , Muzio K, Briones J, et al Prostate cancer brain metastasis: review of a rare complication with limited treatment options and poor prognosis. J Clin Med. 2022;11(14):4165.35887929 10.3390/jcm 11144165 PMC 9323816 · doi ↗ · pubmed ↗
- 5Kanyilmaz G , Aktan M, Yavuz BB, KoçM; Department of Radiation Oncology, Necmettin Erbakan University Meram School of Medicine, Konya, Turkey. Brain metastases from prostate cancer: a single-center experience. Turk J Urol. 2019;45(4):279–283.29975631 10.5152/tud.2018.74555 PMC 6619844 · doi ↗ · pubmed ↗
- 6Hatzoglou V , Patel GV, Morris MJ, et al Brain metastases from prostate cancer: An 11-year analysis in the MRI era with emphasis on imaging characteristics, incidence, and prognosis. J Neuroimaging. 2014;24(2):161–166.23279641 10.1111/j.1552-6569.2012.00767.x PMC 4724409 · doi ↗ · pubmed ↗
- 7Tremont-Lukats IW , Bobustuc G, Lagos GK, et al Brain metastasis from prostate carcinoma: the M. D. Anderson Cancer Center experience. Cancer.2003;98(2):363–368.12872358 10.1002/cncr.11522 · doi ↗ · pubmed ↗
- 8Schröder C , Windisch P, Lütscher J, Zwahlen DR, Förster R. Cranial radiotherapy for prostate cancer patients with brain metastases inaccessible to stereotactic radiotherapy. In Vivo. 2022;36(4):1841–1846.35738629 10.21873/invivo.12901 PMC 9301406 · doi ↗ · pubmed ↗