A Report of a Rare Case of Choledocholithiasis Complicated by Proximal Basket Rod Rupture Requiring Surgical Intervention
Alexandre Gomes

TL;DR
A rare case of a broken ERCP basket during stone removal led to the need for surgery to clear the bile duct.
Contribution
This case highlights a rare complication of ERCP and the need for surgical intervention in such scenarios.
Findings
Mechanical lithotripsy caused a Dormia basket rod rupture during choledocholithiasis treatment.
Surgical intervention was required after failed endoscopic removal of the broken basket and stones.
A biliary stent was placed temporarily before surgical removal of the device and stones.
Abstract
We report a rare case of choledocholithiasis in which mechanical lithotripsy led to rupture of the proximal rod of the Dormia basket, complicating the removal of calculi via endoscopic retrograde cholangiopancreatography (ERCP) and necessitating surgical intervention. ERCP plays a key role in the management of biliopancreatic disorders. Although this approach has improved in recent decades, it remains one of the endoscopic procedures with the highest complication rates. These complications may arise due to the presence of large or impacted stones, resulting in excessive stress on the basket wires or rod. Basket impaction may lead to several complications, such as cholangitis, common bile duct (CBD) perforation, and pancreatitis. Therefore, early removal of the impacted device is recommended. However, no ideal technique for its removal has been established. A 34-year-old female patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
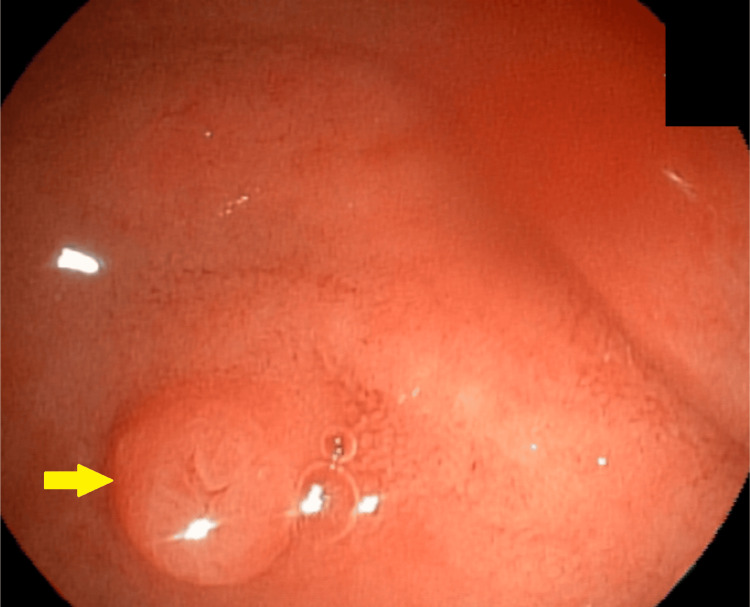 Figure 1
Figure 1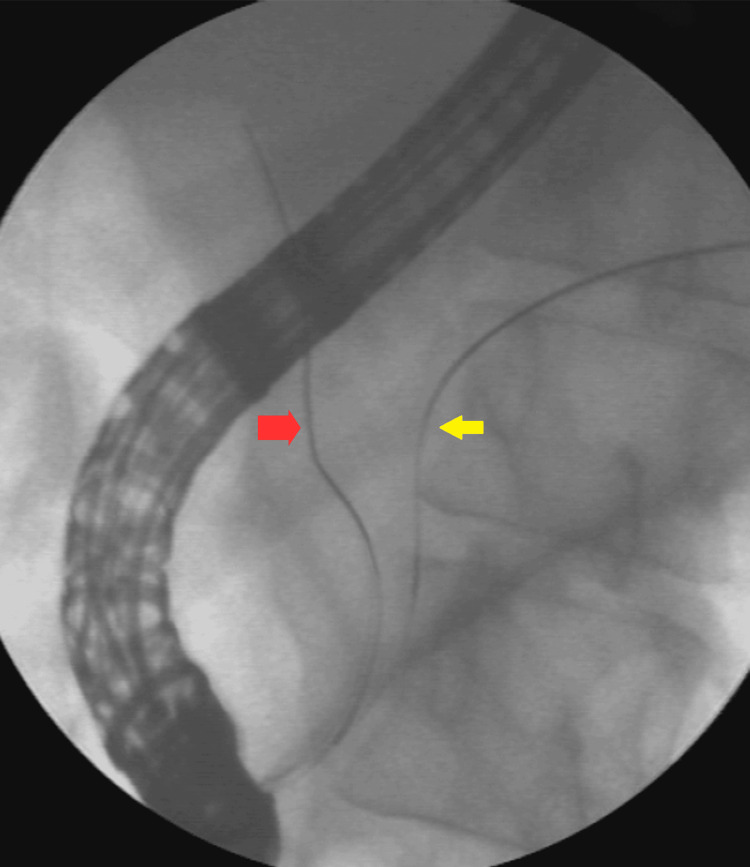 Figure 2
Figure 2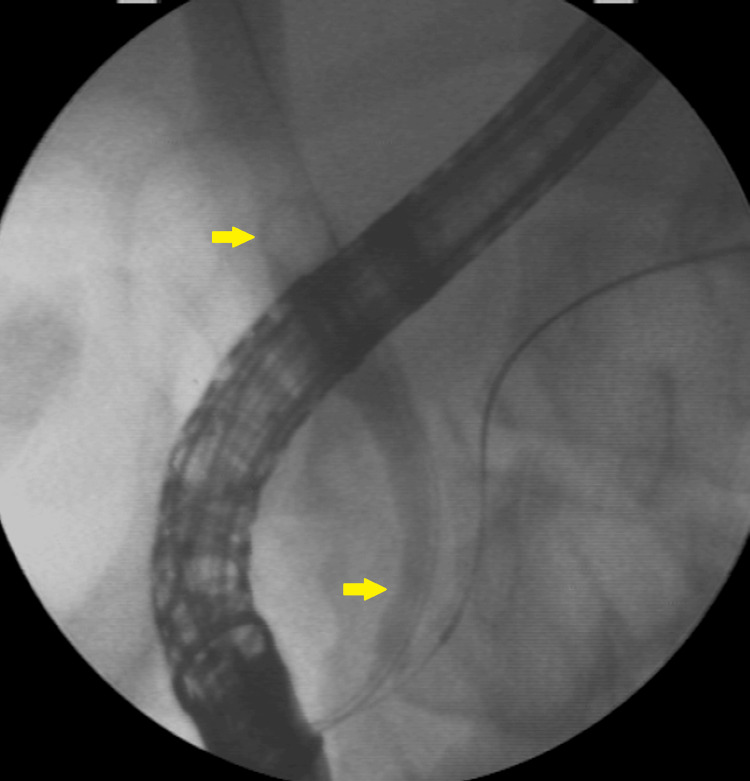 Figure 3
Figure 3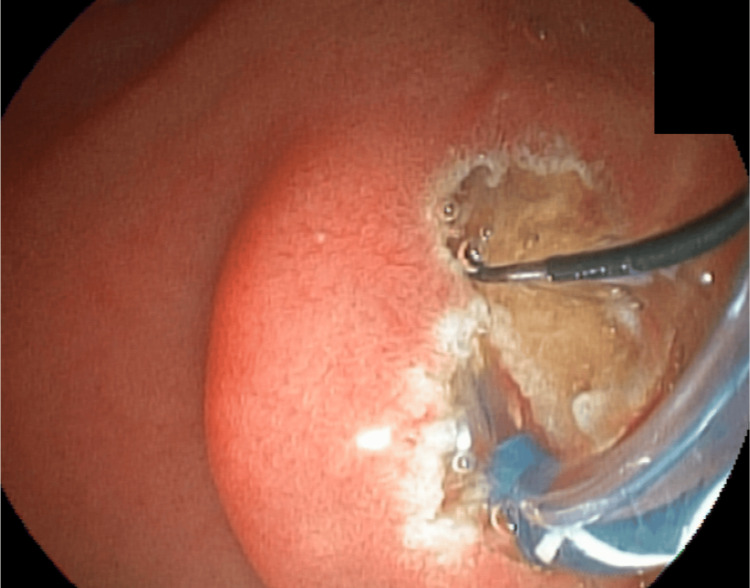 Figure 4
Figure 4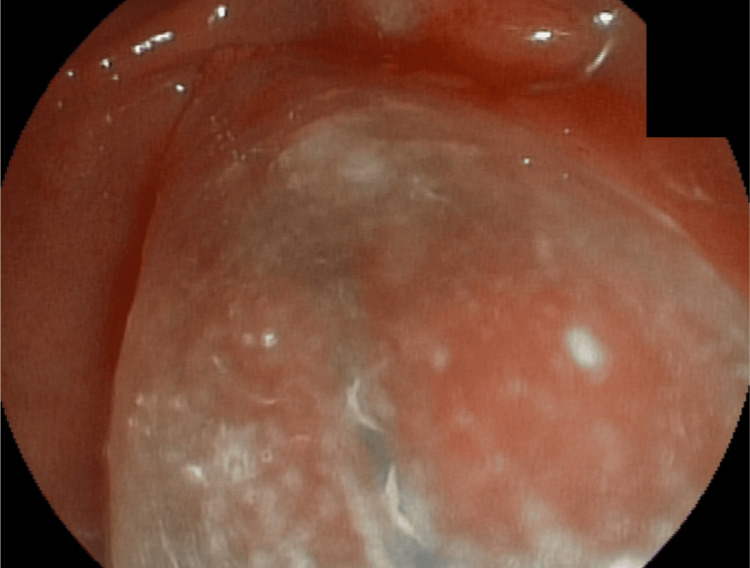 Figure 5
Figure 5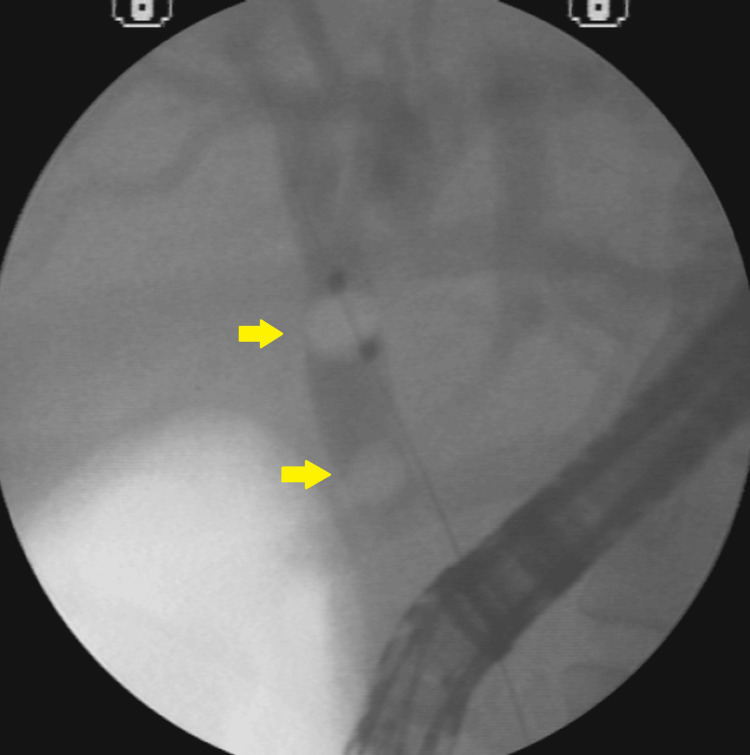 Figure 6
Figure 6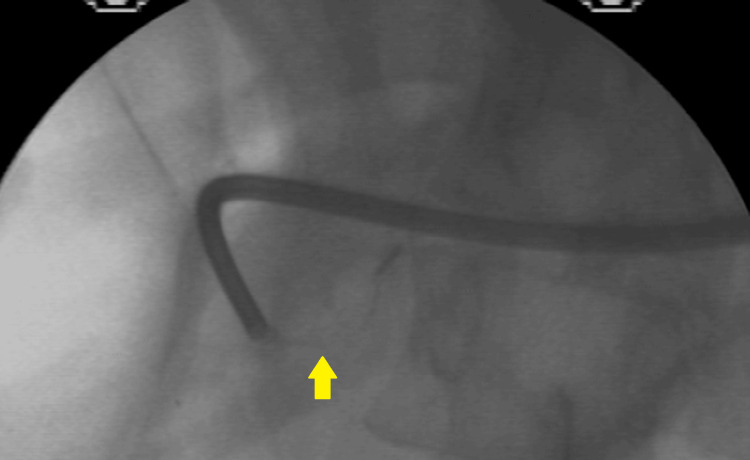 Figure 7
Figure 7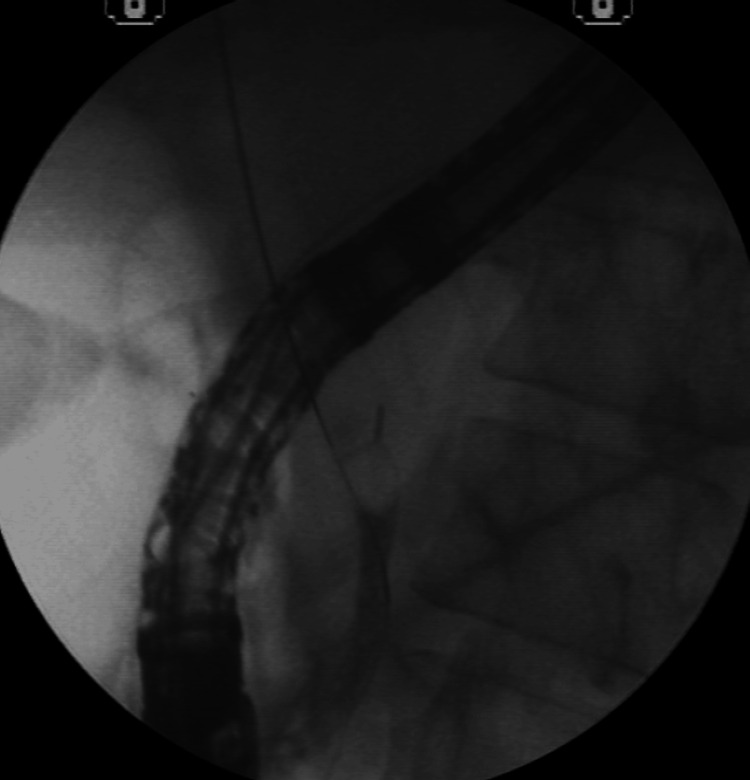 Figure 8
Figure 8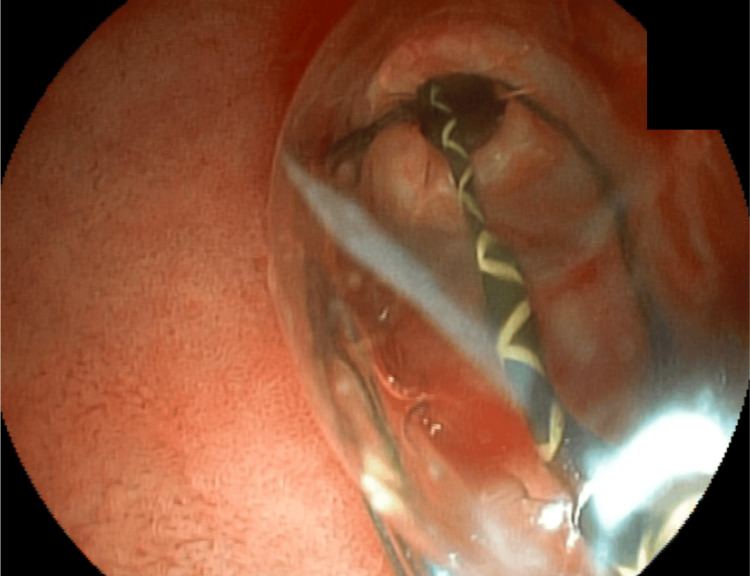 Figure 9
Figure 9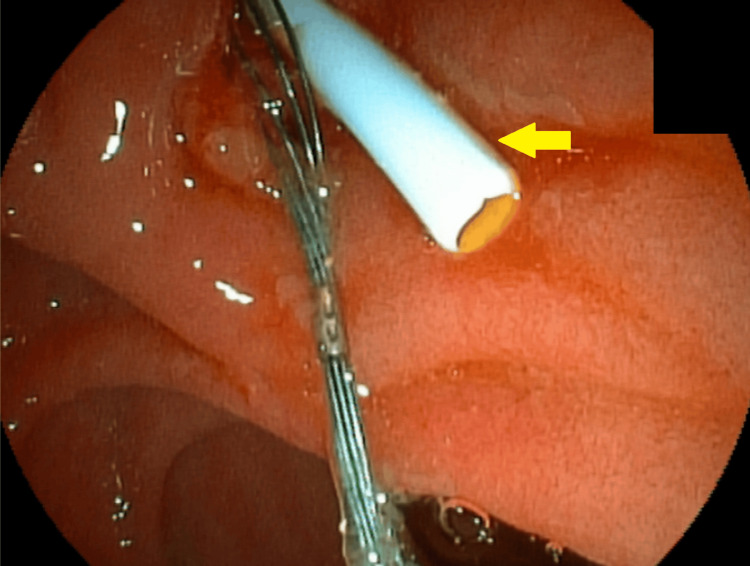 Figure 10
Figure 10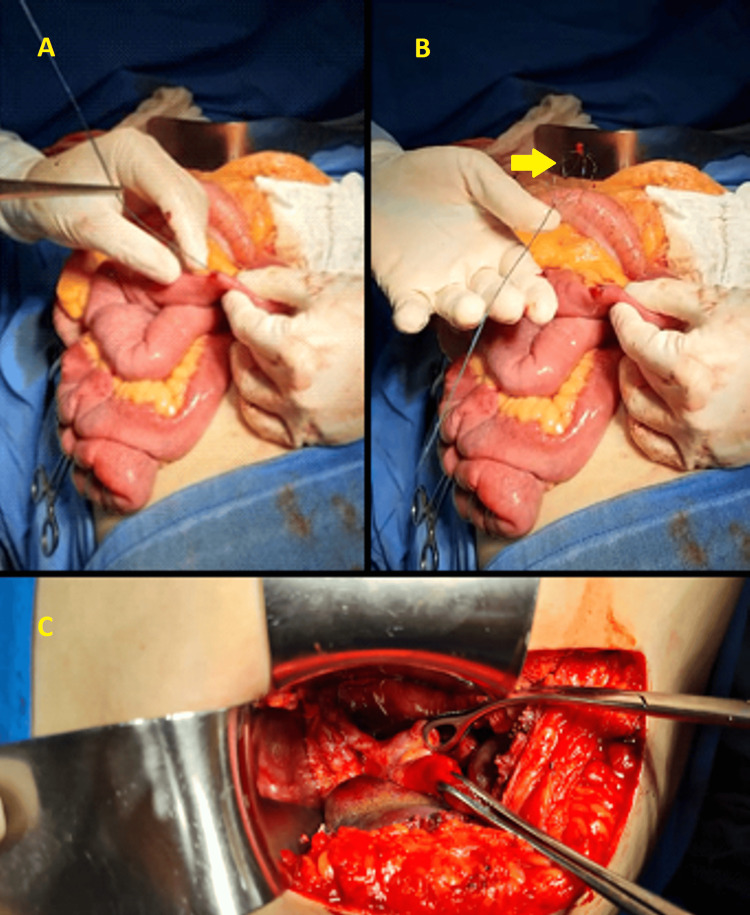 Figure 11
Figure 11Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Biliary and Gastrointestinal Fistulas
Introduction
Impaction of a lithotripter basket with an entrapped stone or rupture of the traction wire during mechanical lithotripsy occurs in 0.8-6% of procedures [1]. Few cases with similar presentations have been described in the medical literature, with resolution achieved through laparoscopy or laparotomy, but we found no case like the one described here [2-5]. Currently, 85-90% of choledocholithiasis cases are successfully treated by endoscopic retrograde cholangiopancreatography (ERCP) techniques: papilla sphincterotomy and basket or balloon extraction. Mechanical lithotripsy captures the stone with a retrieval basket and applies force against a metal sheath to fracture it. The technique has reported success rates of up to 90%, with a low complication rate. The most common complications include basket or system fracture with stone retention, pancreatitis, and bleeding [6].
Case presentation
A 34-year-old white female patient with a body mass index (BMI) of 35 presented with right upper quadrant abdominal pain and jaundice, without fever. Imaging studies revealed cholelithiasis and choledocholithiasis. During ERCP, a small papilla of Vater was identified, making cannulation of the common bile duct (CBD) difficult; the guidewire repeatedly entered only the main pancreatic duct. The double-wire cannulation technique was therefore employed, allowing successful access to the bile duct (Figures 1-2).
Small, flat-type papilla without protrusion, with difficult cannulation
Double-wire cannulation techniqueThe first guide wire (yellow arrow) went to the main pancreatic duct, and the second wire (red arrow) went to the CBD.CBD: common bile duct
Imaging revealed 10-mm calculi in the dilated proximal CBD and a long narrowing of the distal CBD (Figure 3).
Radioscopy showing CBD with calculi and distal narrowingA 10-mm stone in the proximal CBD and long narrowing of the distal CBD.CBD: common bile duct
A sphincterotomy was performed (Figure 4), followed by dilation of the distal CBD using a 15-mm balloon catheter (Figure 5).
Sphincterotomy
Dilation of the distal CBD with a 15-mm balloon catheterCBD: common bile duct
However, stone removal with a stone-extraction balloon was unsuccessful (Figure 6).
Calculi and stone extraction balloonThe stone was not removed due to the distal CBD disproportion.CBD: common bile duct
Basket passage and stone capture for attempted removal; however, distal CBD narrowing did not allow the set to be removed. Mechanical lithotripsy was performed in an attempt to fragment the stone (Figure 7).
Mechanical lithotripsy
Mechanical lithotripsy was unsuccessful in fragmenting the stone, and a complication arose when the proximal rod of the basket broke, making it challenging to remove the basket along with the trapped stone (Figure 8).
Dormia along the entrapped stone and the broken rod
A second 15-mm dilation was performed to remove the imprisoned basket along with the calculi (Figure 9).
Second dilation of the distal CBD with a 15-mm balloon catheterCBD: common bile duct
After this new dilation, the removal of the incarcerated set was attempted using mouse tooth forceps. However, no success was noted. An 8.5-French biliary plastic stent was placed (Figure 10).
Placement of the 8.5-French biliary plastic stent
The endoscopist then recommended a later endoscopic approach, removing the basket, stone, and prosthesis. However, the surgeon of the case opted for open surgery two days later and cholecystectomy, removal of the prosthesis, stone, and basket by duodenotomy, and CBD opening (Figure 11).
Laparotomy, cholecystectomy, and removal of stent, stone, and basket via duodenotomy and CBD opening(A) Palpation and removal of the basket wire through the duodenum. (B) Dormia basket removed without calculi. (C) Removal of the stone through the opening in the CBD.CBD: common bile duct
The patient’s evolution was satisfactory, and she was discharged without other complications.
Discussion
ERCP is a diagnostic and therapeutic procedure commonly used for biliary tract clearance, mainly for removing CBD stones and biliary prosthesis placement in cases of malignant or benign obstruction [7]. Despite a high overall success rate (approximately 95-98%), ERCP-related complications occur in 6-8% of cases. In a study involving 16,855 patients, 1,154 experienced complications (6.85%), and 55 died (0.33%). Mild-to-moderate complications occurred in 872 (5.17%) patients, whereas severe events occurred in 282 (1.67%), pancreatitis in 585 (3.47%), 242 (1.44%), bleeding in 226 (1.34%), and perforations in 101 (0.60%). Cardiovascular and anesthetic complications occurred in 173 (1.33%), with nine fatalities (0.07%) [6,8,9]. The literature offers abundant data on ERCP complications [9]; however, the risks remain significantly lower compared to surgical management of CBD stones. Over recent decades, the treatment of choledocholithiasis has evolved significantly with advances in endoscopic techniques.
This case involved choledocholithiasis with an impacted stone that was large and disproportionate to the caliber of the distal CBD. Despite a wide papillary sphincterotomy and dilation of the distal CBD using a 15-mm balloon catheter, stone extraction was unsuccessful. Urgent mechanical lithotripsy was attempted; however, rupture of the proximal wire of the Dormia basket occurred, making removal of the device impossible. A second attempt was made after repeat dilation of the distal CBD with a 15-mm balloon catheter, but it was also unsuccessful. A plastic biliary stent was then placed. The point of rupture was located at the junction between the nitinol and steel components of the basket rod. This interface may represent a potential point of structural weakness in nitinol baskets and should be taken into consideration when such materials are used.
In cases of disproportion between the size of the large calculi and the narrowing distal portion of the CBD, the endoscopist may opt for some strategies to avoid the imprisonment of the basket and mechanical lithotripsy [10-12]. One is to leave the plastic biliary stent for three to four months and make a new attempt to withdraw. Another option is to perform early cholangioscopy-guided electrohydraulic lithotripsy or laser fragmentation of the stones [13].
There were three possible approaches to resolve this case. The ideal strategy would have been delayed cholangioscopy with laser lithotripsy, followed by removal of the basket, stone, and stent. Alternatively, the case could have been managed laparoscopically through cholecystectomy, choledocholithotomy, and extraction of the basket, stone, and stent. However, definitive treatment was achieved via laparotomy, with cholecystectomy, choledocholithotomy, and removal of the basket, stone, and stent.
Conclusions
We report a case of choledocholithiasis in which mechanical lithotripsy resulted in rupture of the proximal nitinol rod of a Dormia basket, making stone removal via ERCP difficult and requiring surgical intervention. The most appropriate approach would have been delayed cholangioscopy with laser lithotripsy, followed by the basket, calculi, and stent removal. Alternatively, laparoscopic management with cholecystectomy, choledocholithotomy, and removal of the basket, calculi, and stent could have been considered. However, the case was ultimately resolved through open laparotomy, including cholecystectomy, choledocholithotomy, and removal of all retained elements.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Biliary-basket impaction complicated by in vivo traction-wire fracture: report of a novel management approach Gastrointest Endosc Maple JT Baron TH 103110336420061714092710.1016/j.gie.2006.04.023 · doi ↗ · pubmed ↗
- 2Dormia basket impacted during ERCP, resolved by laparoscopic bile duct approach: case report Int J Surg Case Rep Vargas Ávila AL Martin Perez JA Vargas Flores J 62667920213343477010.1016/j.ijscr.2020.12.078PMC 7809167 · doi ↗ · pubmed ↗
- 3Laparoscopic retrieval of impacted and broken dormia basket using a novel approach J Minim Access Surg Varshney VK Sreesanth KS Gupta M Garg PK 4154171620203297835510.4103/jmas.JMAS_245_19PMC 7597889 · doi ↗ · pubmed ↗
- 4Emergency open surgery with a duodenotomy and successful removal of an impacted basket following a complicated endoscopic retrograde cholangiopancreatography procedure: a case report J Med Case Rep Abu Shakra I Bez M Bickel A 931520213361875610.1186/s 13256-020-02608-1PMC 7901177 · doi ↗ · pubmed ↗
- 5Impaction of a lithotripsy basket during endoscopic lithotomy of a common bile duct stone World J Gastroenterol Fukino N Oida T Kawasaki A Mimatsu K Kuboi Y Kano H Amano S 283228341620102053360710.3748/wjg.v 16.i 22.2832 PMC 2883143 · doi ↗ · pubmed ↗
- 6Endoscopic retrograde cholangiopancreatography-related complications: risk stratification, prevention, and management Clin Endosc Wu CC Lim SJ Khor CJ 4334455620233746010310.5946/ce.2023.013PMC 10393565 · doi ↗ · pubmed ↗
- 7Endoscopic management of difficult common bile duct stones World J Gastroenterol Trikudanathan G Navaneethan U Parsi MA 1651731920132334593910.3748/wjg.v 19.i 2.165PMC 3547556 · doi ↗ · pubmed ↗
- 8Retained stone retrieval basket causing chronic pancreatitis: a case report Front Surg Lee JW Tan MY Koh C Iyer SG Gao Y 12358331020233762194710.3389/fsurg.2023.1235833 PMC 10445159 · doi ↗ · pubmed ↗