LONG-TERM EFFICACY OF SPASTICITY-CORRECTIVE SURGERY AND BOTULINUM TOXIN INJECTIONS FOR UPPER LIMB SPASTICITY TREATMENT
Therese RAMSTRÖM, Johanna WANGDELL, Carina REINHOLDT, Trandur ULFARSSON, Lina Bunketorp KÄLL

TL;DR
This study found that surgery provides longer-lasting relief from upper limb spasticity compared to botulinum toxin injections.
Contribution
The study compares the long-term efficacy of surgery and botulinum toxin for upper limb spasticity treatment.
Findings
Surgery led to significantly greater reductions in spasticity compared to botulinum toxin.
Surgical benefits were sustained, while botulinum toxin effects were temporary.
Surgery improved range of motion, grip strength, and patient satisfaction more effectively.
Abstract
To evaluate the long-term efficacy of spasticity-corrective surgery and botulinum toxin treatment in patients with upper limb spasticity. Pretest-posttest quasi-experimental study. Thirty-four patients with disabling spasticity. Patients were divided into 2 groups based on their treatment preference: the surgery group, which underwent tendon lengthening/release (n = 17), and the botulinum toxin injection group (n = 17). The primary outcome measure was the Modified Ashworth Scale. Secondary outcomes included range of motion, grip strength, and activity performance. Assessments were conducted at baseline for both groups, at 3 months following botulinum toxin injection, and at 6 months following surgery, with an additional peak-effect evaluation for botulinum toxin at week 5. The surgery group demonstrated significantly greater reductions in composite Modified Ashworth Scale scores,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
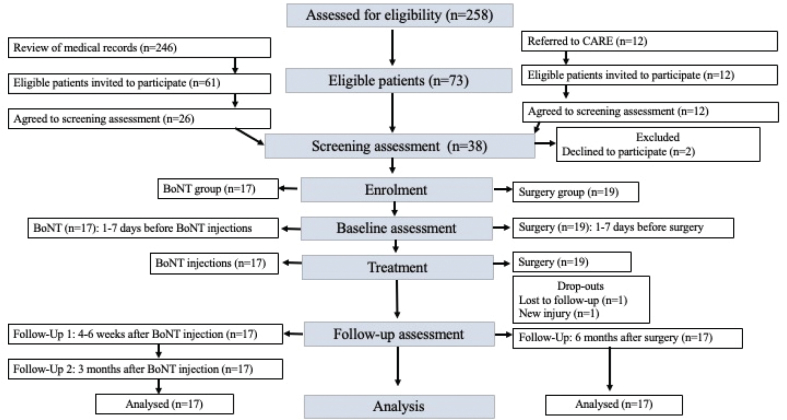 Fig. 1
Fig. 1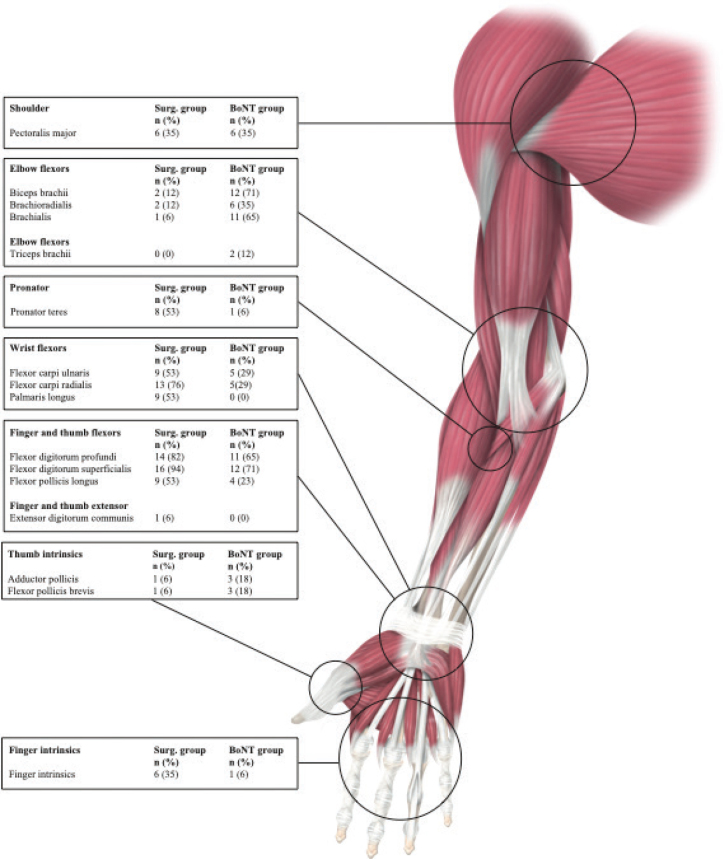 Fig. 2
Fig. 2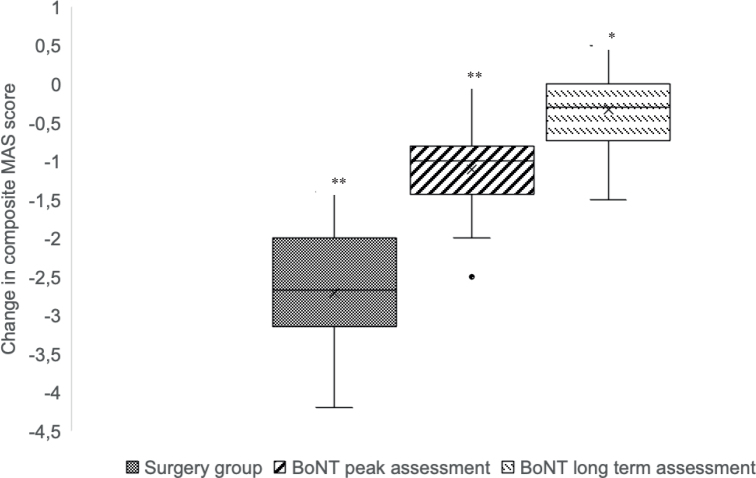 Fig. 3
Fig. 3| Characteristics | Surgery group | BoNT group |
|---|---|---|
|
| 17 | 17 |
| 60 (26–76) | 55 (24–81) | |
|
| ||
| Male | 12 (71) | 9 (53) |
| Female | 5 (29) | 8 (47) |
|
| ||
| SCI | 8 (47) | 1 (6) |
| Stroke | 8 (47) | 14 (82) |
| TBI | 1 (6) | 2 (12) |
| 7.5 (2–17) | 11.8 (1–33) | |
|
| ||
| Wheelchair | 6 (35) | 3 (18) |
| Wheelchair partial | 4 (23) | 5 (29) |
| Walking | 7 (41) | 9 (53) |
|
| ||
| HFR | 5 (29) | 6 (35) |
| LFR | 7 (41) | 5 (29) |
| NFR | 5 (29) | 6 (35) |
|
| ||
| 1 | 4 (23) | 7 (41) |
| 2 | 2 (12) | 2 ((12) |
| 3 | 11 (65) | 8 (47) |
| 4 | 0 (0) | 0 (0) |
|
| ||
| Right | 7 (41) | 10 (59) |
| Left | 10 (59) | 7 (41) |
|
| 3 (18) | 1 (0.05) |
|
| 17 (100) | 16 (94) |
| Patient | Diagnosis | Sex | Regimen | Age | Target muscle | Product | Aim with treatment |
|---|---|---|---|---|---|---|---|
|
| |||||||
| 1 | TBI | Female | LFR | 40 | BR(50U), Brachialis(50U) FDS(50U), FDP(60U) | Botox | Enable use as a supportive arm for daily activities, balance while walking |
| 2 | Stroke | Female | HFR | 24 | BR(25U), Brachialis(25U), FDS(25U), FDP(25U) | Botox | Grasping and releasing objects. Use of hand in daily activities and work. |
| 3 | Stroke | Male | LFR | 55 | Bic(150U), Brachialis(150U), FDS(150U), FDP (150U) | Dysport | Reduce pain due to increased tone, facilitate balance and walking with a straighter arm |
| 4 | Stroke | Male | NFR | 68 | Pec(100U), Bic(100U), BR(100U), Brachialis(50U), FCU(100U), FDP(100U) | Dysport | Facilitate hygiene; facilitate range of motion exercise to reduce risk of contractures |
| 5 | Stroke | Male | NFR | 64 | Pec(50U), Bic(50U), Brachialis(50U), FCU(75U), FCR(75U) | Xeomin | Facilitate hygiene, dressing |
| 6 | Stroke | Male | HFR | 62 | Bic(100U), BR(100U), Brachialis(100U), FDS(100U), ADP(40U) | Dysport | Grasping and releasing objects. Use of hand in daily activities, facilitate balance and walking with a straighter arm |
| 7 | Stroke | Female | HFR | 39 | FDS(140U), FDP(100U), FPL(60U) | Dysport | Use of hand in daily activities |
| 8 | Stroke | Female | LFR | 62 | Bic(180U), FDS(220U), FDP(220U), FPL(70U), FPB(50U), ADP(50U) | Dysport | Reduce pain, facilitate hygiene, enable use as a supportive arm for daily activities |
| 9 | Stroke | Male | HFR | 54 | Bic(25U), BR(25U), Brachialis(35U), Pron(20U), FDS(70U), FDP(25U) | Xeomin | Grip function, use of hand in daily activities |
| 10 | TBI | Female | NFR | 67 | Bic(100U), Brachialis(100U), FCU(100U), FDS(100U) | Dysport | Facilitate hygiene, dressing, improve range of motion to reduce contracture risk |
| 11 | Stroke | Male | NFR | 81 | Biceps(75U), BR(35U), Brachialis(40U), FCU(50U), FCR(50U), Intrinsic(25U), ADP(25U) | Botox | Facilitate hygiene, dressing, improve range of motion to reduce contracture risk |
| 12 | Stroke | Female | NFR | 56 | Pec(50U), Tric(50U), Bic(50U), Brachialis(25U), FDS(40U), FDP(25U), FPL(25U) | Botox | Facilitate hygiene, dressing, walking ability |
| 13 | Stroke | Male | LFR | 66 | Pec(50U), Bic(50U), Brachialis(50U), FCU(50U), FDP(50U), FPL(30U) | Botox | Balance while walking, enable use as a supportive arm for daily activities |
| 14 | Stroke | Male | HFR | 52 | Pec(40U), Tric(15U), Bic(15U), FDP(30U) | Botox | Reduce pain, use of hand in daily activities and leisure activities |
| 15 | Stroke | Female | LFR | 42 | FCR(75U), FDS(100U), FDP(125U), | Dysport | Enable use as a supportive arm for daily activities |
| 16 | Stroke | Female | NFR | 42 | FCR(60U), FDS(20U), FPB(10U) | Xeomin | Facilitate hygiene, dressing, improve range of motion to reduce contracture risk, cosmetic |
| 17 | SCI | Male | HFR | 68 | Pec(40U), Bic(50U), FCR(50U), FDS(20U), FPB(5U) | Xeomin | Grip function, use of hand in daily activities |
|
| |||||||
| Patient | Diagnosis | Sex | Regimen | Age | Target muscle | Aim with treatment | |
|
| |||||||
|
| |||||||
| 1 | Stroke | Male | LFR | 62 | Pron, FCU, FCR, Intrinsic | Pain due to increase tone, support arm in daily life | |
| 2 | Stroke | Male | LFR | 68 | Pec, Pron, FCU, FCR, PL, FDS, FDP, Intrinsic | Enable use as a supportive arm for daily activities | |
| 3 | Stroke | Male | NFR | 75 | FDS, FDP, Intrinsic, FPL | Facilitate hygiene | |
| 4 | Stroke | Male | LFR | 62 | Pec, FCU, FCR, PL, FDS, FDP, ADP | Facilitate hygiene, support arm in daily activities | |
| 5 | Stroke | Male | NFR | 74 | Pec, Pron, FCU, FCR, PL, FDS, FDP, EDC | Facilitate hygiene | |
| 6 | Stroke | Female | LFR | 35 | Pron, FCR, PL, FDS, FPL | Balance while walking, enable use as a supportive arm for daily activities | |
| 7 | SCI | Female | LFR | 56 | Pec, Pron, FDS, FDP | Facilitate hygiene, facilitate dressing and posture in sitting, support hand | |
| 8 | SCI | Male | HFR | 52 | FDS, FDP, FPL | Grip function, use of hand in daily activities and leisure activities | |
| 9 | Stroke | Male | NFR | 58 | Pec, Bic, BR, Brachialis, FCU, FCR, FDS, FDP, FPL | Facilitate hygiene | |
| 10 | SCI | Male | HFR | 59 | Pron, FCU, FCR, FDS, FDP, Intrinsic, | Grip function, use of hand in daily activities and leisure activities | |
| 11 | SCI | Male | HFR | 68 | Pec, FCU, FCR, PL, FDS, FDP, FPL | Grip function, use of hand in daily activities | |
| 12 | SCI | Female | LFR | 63 | FCU, FCR, PL, FDS, FDP | Facilitate hygiene, enable use as a supportive arm for daily activities | |
| 13 | TBI | Male | NFR | 45 | Bic, Pron, FCR, FDS, FDP, Intrinsic, FPL | Facilitate hygiene | |
| 14 | Stroke | Female | NFR | 69 | FCU, PL, FDS, FDP, FPL, FPB | Facilitate hygiene, dressing, | |
| 15 | SCI | Male | LFR | 76 | FCR, PL, FDS, FDP, Intrinsic, | Grip function, use of hand in daily activities | |
| 16 | SCI | Male | HFR | 26 | BR, Pron, FCR, PL, FDS, FPD, FPL | Grip function, use of hand in daily activities and leisure activities | |
| 17 | SCI | Female | HFR | 72 | FCR, FDS, FPL | Grip function, use of hand in daily activities | |
| Pectoral Muscles | Spastic pectoral muscles promote shoulder internal rotation and adduction, leading to poor posture, restricted breathing, and challenges with dressing and washing the upper body. |
| Elbow Flexors | Spasticity in the elbow flexors (biceps brachii, brachioradialis, and brachialis) keep the elbow flexed and the forearm supinated (due to the biceps brachii), restricting reach and grasp. This can impair balance and walking and interfere with hygiene and dressing of the upper body. |
| Forearm Muscles | The pronator teres, when spastic, forces the arm into a pronated position, making object grasping difficult and leading to compensatory shoulder movements during hand use. |
| Wrist and Finger Flexors | Spastic wrist flexors (flexor carpi radialis, flexor carpi ulnaris, and palmaris longus) hold the wrist in a flexed position, making grasping difficult and sometimes interfering with dressing. Finger flexors (flexor digitorum superficialis and flexor digitorum profundus) cause the fingers to remain clenched, making it difficult to open the hand, release objects, maintain hand hygiene, or cut fingernails. |
| Thumb muscles | Thumb flexor spasticity pulls the thumb into the palm, preventing key pinch and making it difficult to hold or place objects in the hand. An overactive thumb abductor positions the thumb too close to the index finger, restricting cylindrical grasp and pinch. Additionally, spastic intrinsic muscles keep the metacarpophalangeal (MCP) joints flexed, further restricting hand opening. |
| Outcome measure |
| Diff surgery. Baseline-long term. Mean(SD)/Median (min–max) |
| Diff BoNT Baseline -peak. Mean(SD)/Median (min–max) |
| Diff BoNT Baseline -long term. Mean (SD)/Median (min–max) | ||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Wrist neutral A | 14 | 1.1 (0.8) | 12 | 0.5 (0.7) | 0.169 | 12 | 0.9 (0.3) |
|
| 1.0 (0.0–2.0) | 0.0 (0.0–2.0) | 0.6346 | 0.0 (0.0–1.0) | 0.3123 | ||||
| Wrist neutral P | 17 | 0.8 (1.2) | 17 | 0.4 (0.6) | 0.375 | 17 | 0.0 (0.0) |
|
| 0.0 (0.0–4.0) | 0.0 (0.0–2.0) | 0.5409 | 0.0 (0.0–0.0) | 0.1740 | ||||
| Wrist flexed A | 14 | 0.6 (0.7) | 12 | 0.7 (1.1) | 0.539 | 12 | 0.4 (0.9) | 0.722 |
| 0.5 (0.0–2.0) | 0.5 (–1.0–3.0) | 0.1517 | 0.0 (0.0–3.0) | 0.0908 | ||||
| Wrist flexed P | 17 | 0.5 (0.9) | 17 | 0.2 (0.4) | 0.786 | 17 | 0.0 (0.3) | 0.245 |
| 0.0 (0.0–2.0) | 0.0 (0.0–1.0) | 0.0637 | 0.0 (–1.0–1.0) | 0.3026 | ||||
| Resting position | 17 | 1.7 (1.0) | 17 | 0.5 (0.6) |
| 17 | 0.2 (0.6) |
|
| 2.0 (0.0–4.0) | 1.0 (–1.0–1.0) | 0.6336 | 0.0 (–1.0–1.0) | 0.7225 | ||||
| Grip strenght | 14 | –0.6 (4.3) | 12 | –2.3 (4.0) | 0.347 | 12 | 0.9 (3.6) | 0.297 |
| –0.5 (–7.4–8.0) | –1.4 (–11.4–3.7) | 0.1867 | 0.1 (–4.2–6.0) | 0.2070 | ||||
| Pinch strenght | 14 | 0.8 (0.8) | 13 | –0.4 (1.1) |
| 13 | –0.2 (1.1) |
|
| 0.8 (–1.0–2.0) | –0.2 (–2.9–1.3) | 0.5794 | 0.0 (–2.7–2.0) | 0.5234 | ||||
| Pain(VAS) | 17 | –1.3 (2.7) | 16 | –1.1 (1.8) | 0.790 | 16 | 0.2 (1.3) | 0.179 |
| 0.0 (–10.0–0.0) | 0.0 (–5.0–2.0) | 0.0534 | 0.0 (–2.0–3.0) | 0.2703 | ||||
| Hand function (VAS) | 17 | 2.3 (2.3) | 16 | 0.7 (1.9) |
| 16 | 0.6 (1.9) |
|
| 2.0 (0.0–9.0) | 0.0 (–2.0–6.0) | 0.4266 | 0.0 (–1.0–6.0) | 0.4579 | ||||
| Cosmetic (VAS) | 17 | –0.3 (1.9) | 16 | –0.2 (2.1) | 0.657 | 16 | –0.1 (1.8) | 0.471 |
| 0.0 (–5.0–5.0) | 0.0 (–3.0–4.0) | 0.0893 | 0.0 (–4.0–5.0) | 0.2418 | ||||
| Spasticity (VAS) | 17 | –4.7 (3.1) | 16 | –1.8 (1.6) |
| 16 | –0.0 (1.3) |
|
| –4.0 (–10.0–0.0) | –2.1 (–4.0–2.0) | 0.4416 | 0.0 (–3.5–2.0) | 0.7582 | ||||
| GRT | 10 | 27.4 (50.7) | 8 | 18.1 (20.5) | 8 | 14.4 (20.9) | ||
| 19 (–7.0–174) | 24.0 (–15.0–38.0) | 10.0 (–9.0–51.0) | ||||||
|
| ||||||||
| Subtest 1 | 12 | 29.2 (39.9) | 8 | 10.0 (15.2) | 8 | 1.2 (8.3) | ||
| 10 (0–120) | 0.0 (0.0–40.0) | 0.0 (–10.0–20.0) | ||||||
| Subtest 2 | 12 | 25 (26.4) | 8 | 22.5 (19.1) | 8 | 10.0 (15.2) | ||
| 20 (0–80) | 20.0 (0.0–50.0) | 5.0 (–10.0–30.0) | ||||||
| Subtest 3 | 12 | 27.5 (33.9) | 9 | 30.0 (28.7) | 9 | 15.5 (17.4) | ||
| 15 (–10–100) | 40.0 (0.0–80.0) | 20.0 (0.0–50.0) | ||||||
| Subtest 4 | 16 | 36.2 (36.8) | 16 | 11.2 (15.9) |
| 16 | –6.9 (26.8) |
|
| 35 (0–120) | 10.0 (–10.0–40.0) | 0.3659 | 0.0 (–70.0–20.0) | 0.5297 | ||||
| Subtest 5 | 11 | 41.8 (31.6) | 5 | 22.0 (19.2) | 5 | 14.0 (20.7) | ||
| 30 (0–90) | 20.0 (0.0–50.0) | 10.0 (–10–40.0) | ||||||
| COPM-P | 12 | 2.8 (1.1) | 14 | 1.7 (1.4) | 0.067 | 14 | 1.0 (1.6) |
|
| 3.0 (0.8–4.8) | 1.6 (–0.6–5.0) | 0.3588 | 0.1 (–0.6–4.0) | 0.4910 | ||||
| COPM-S | 12 | 2.9 (1.4) | 12 | 2.7 (2.1) | 0.887 | 12 | 1.6 (1.5) |
|
| 2.8 (–0.6–5.0) | 2.7 (–0.2–5.4) | 0.0292 | 1.5 (0.0–4.0) | 0.4133 | ||||
| ArmA a | 17 | –11.1 (6.0) | 17 | –4.1 (4.6) |
| 17 | –0.2 (4.8) |
|
| –12.0 (–21.0–0.0) | –4.0 (–14–3.0) | 0.5385 | 0.0 (–6.0–13.00) | 0.7316 | ||||
| ArmA b | 17 | –8.0 (7.3) | 17 | –2.5 (7.1) |
| 17 | –1.5 (4.3) |
|
| –6.0 (–20.0–0.0) | –1.0 (–18.0–16.0) | 0.3712 | 0.0 (–12.0–9.0) | 0.4925 | ||||
| Eq5dl VAS | 17 | 7.8 (13.4) | 16 | 2.0 (16.5) | 0.363 | 16 | 9.0 (13.9) | 0.929 |
| 10.0 (–15.0–40.0) | 0.0 (–40.0–30.0) | 0.1636 | 3.0 (–10.0–35.0) | 0.0189 | ||||
| Outcome measure |
| Baseline mean (SD)/median (range) | 6 months mean (SD)/median (range) | Diff mean (SD)/median (range) |
|
|---|---|---|---|---|---|
|
| |||||
| Shoulder abduktion A | 6 | 38.3 (34.3) | 53.3 (36.1) | 15 (18.7) | |
| 25 (0–90) | 55 (0–90) | 10 (0–50) | |||
| Shoulder abduktion P | 6 | 77.5 (12.5) | 113.3 (20.6) | 35.8 (22.4) | |
| 77.5 (60–90) | 115 (90–140) | 37.5 (0–70) | |||
| Supination A | 7 | 5.7 (28.3) | 70.7 (28.6) | 65.0 (25.8) | |
| 0 (–45–45) | 80 (10–90) | 80 (15–90) | |||
| Supination P | 9 | 58.3 (35) | 86.1 (9.9) | 27.8 (30.2) | |
| 80 (0–90) | 90 (60–90) | 10 (0–70) | |||
| Wrist extension A | 11 | 25.9 (26.4) | 57.3 (21.4) | 31.4 (14.1) |
|
| 0 (0–9.5) | 0 (0–9.5) | 0 (–5–5) | |||
|
| |||||
| Wrist neutral A | 12 | 3.0 (0.8) | 4.0 (0.7) | 0.5 (0.7) |
|
| 3 (2–4) | 4 (3–5) | 0.0 (0.0–2.0) | |||
| Wrist flexed A | 12 | 4.0 (0.8) | 4.6 (0.5) | 1.0 (0.7) |
|
| 4 (2–5) | 5 (245) | 1.0 (0.0–2.0) | |||
| Wrist neutral P | 17 | 4.1 (1.2) | 4.9 (0.2) | 0.8 (1.2) |
|
| 4 (1–5) | 5 (4–5) | 0.0 (0.0–4.0) | |||
| Wrist flexed P | 17 | 4.5 (0.8) | 5 (0.0) | 0.5 (0.9) |
|
| 5 (3–5) | 5 (5–5) | 0.0 (0.0–2.0) | |||
| Resting position | 17 | 1.8 (0.7) | 3.5 (0.8) | 1.7 (1.0) |
|
| 2 (1–3) | 4 (2–5) | 2.0 (0.0–4.0) | |||
| Thumb-indexfinger | 12 | 6.3 (4.5) | 9.5 (4.2) | 2.7 (4.5) | 0.053 |
| 7 (0–14) | 10 (3–16) | 2 (–3.5–13.5) | |||
| First webspace | 12 | 6.2 (3.5) | 7.5 (3.0) | 1.3 (3.7) | 0.285 |
| 6 (0–12) | 7.2 (3–11) | 0.7 (–5–8) | |||
| GRT | 10 | 79.1 (63.1) | 109.2 (79.9) | 27.4 (50.7) |
|
| 55.5 (19–190) | 89 (16–231) | 19 (–7–174) | |||
|
| |||||
| Subtest 1 | 12 | 13.3 (31.4) | 42.5 (48.1) | 29.2 (39.9) |
|
| 31.4 (0–90) | 25 (0–120) | 10 (0–120) | |||
| Subtest 2 | 12 | 31.7 (37.4) | 56.7 (44.8) | 25 (26.4) |
|
| 10 (0–100) | 60 (0–130) | 20 (0–80) | |||
| Subtest 3 | 12 | 52.5 (47.3) | 80 (47.3) | 27.5 (33.9) |
|
| 65 (0–150) | 80 (0–150) | 15 (–10–100) | |||
| Subtest 4 | 16 | 71.2 (53.5) | 107.5 (54.7) | 36.2 (36.8) |
|
| 65 (0–150) | 135 (0–150) | 35 (0–120) | |||
| Subtest 5 | 11 | 93.6 (54.7) | 135.4 (54.7) | 41.8 (31.6) |
|
| 120 (0–150) | 120 (0–150) | 30 (0–90) | |||
| COPM-P | 12 | 2.3 (1.0) | 5.4 (1.1) | 2.8 (1.1) |
|
| 2.7 (1–4) | 5.3 (3–7) | 3 (0.8–4.8) | |||
| COPM-S | 12 | 2.2 (5.1) | 5.1 (1.4) | 2.9 (1.4) |
|
| 2.1 (1–3) | 5.6 (1–7) | 2.8 (–0.6–5) | |||
| ArmA subtest a | 17 | 16.2 (4.6) | 5.1 (3.5) | 11.2 (6.0) |
|
| 17 (10–23) | 5 (0–13) | –12 (–21–0) | |||
| ArmA subtest b | 17 | 41.2 (10.3) | 33.2 (15.4) | 8.0 (7.3) |
|
| 48 (21–51) | 38 (4–50) | –6 (–20–0) | |||
| Eq5dl | 17 | 63.5 (23.0) | 71.3 (20.9) | 7.8 (13.4) |
|
| 70 (10–90) | 75 (20–100) | 10 (–15–40) | |||
| Outcome measure |
| Baseline mean (SD) median (min–max) | FU1 (peak) mean (SD) median (min–max) | Mean diff mean (SD) median (min–max) |
| FU2 (LT) mean (SD) median (min–max) | Mean diff mean (SD) median (min-max) |
|
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Shoulder abduktion P | 6 | 93.3 (33.3) | 113.3 (18.6) | 20 (22.8) | 96.7 (18.6) | 3.3 (25.0) | ||
| 100 (30–120) | 120 (90–130) | 15 (0–60) | 95 (80–130) | 25 (–20–50) | ||||
| Elbow extension A | 8 | 16.2 (14.1) | 9.4 (10.8) | –6.9 (11.0) | 13.7 (10.3) | –2.5 (11.9) | ||
| 15 (0–40) | 5 (0–25) | –5 (–20–10) | 15 (0–30) | 0 (–20–10) | ||||
| Elbow extensionP | 14 | 17.5 (25.8) | 10.0 (19.3) | –7.5 (9.7) |
| 14.6 (25.0) | –2.8 (6.1) | 0.102 |
| 10 (0–75) | 0 (0–65) | –5 (–30–0) | 0 (0–75) | 0 (–10–10) | ||||
| Wrist extension P | 8 | 26.2 (34.6) | 42.5 (35.7) | 16.2 (16.0) |
| 28.7 (41.5) | 2.5 (16.7) | |
| 15 (–10–90) | 30.0 (0–90) | 10 (0–40) | 10 (–10–90) | 0 (–20–40) | ||||
|
| ||||||||
| Wrist neutral A | 10 | 2.2 (1.6) | 2.8 (1.6) | 0.5 (0.7) |
| 2.3 (1.6) | 0.1 (0.3) | 0.317 |
| 1 (1–5) | 2.5 (1–5) | 0 (0–2) | 1.5 (1–5) | 0 (0–5) | ||||
| Flexed wrist A | 10 | 2.9 (1.7) | 3.7 (1.6) | 0.8 (1.1) | 0.054 | 3.4 (1.6) | 0.5 (1.0) | 0.102 |
| 2.5 (1–5) | 4.5 (1–5) | 1 (–1–3) | 3.5 (1–5) | 0 (0–3) | ||||
| Wrist neutral P | 17 | 3.9 (1.0) | 4.3 (0.9) | 0.4 (0.6) |
| 3.9 (1.0) | 0.0 (0.0) | 1.0 |
| 4 (2–5) | 5 (2–5) | 0.0 (0.0–2.0) | 4 (2–5) | 0.0 (0.0–0.0) | ||||
| Flexed wrist P | 17 | 4.5 (0.9) | 4.8 (0.6) | 0.2 (0.4) |
| 4.5 (0.9) | 0.0 (0.3) | 1.0 |
| 5 (2–5) | 5 (3–5) | 0.0 (0.0–1.0) | 5 (2–5) | 0.0 (–1.0–1.0) | ||||
| Resting position | 17 | 2.0 (1.0) | 2.5 (0.9) | 0.5 (0.6) |
| 2.2 (1.0) | 0.2 (0.6) | 0.102 |
| 1 (1–4) | 3 (1–4) | 1.0 (–1.0–1.0) | 3 (1–4) | 0.0 (–1.0–1.0) | ||||
| Thumb-indexfinger | 8 | 5.25 (5.7) | 5.2 (5.9) | 0.0 (0.5) | 6.3 (6.5) | 1.1 (1.8) | ||
| 4 (0–16) | 3.5 (0–16) | 0 (–1–1) | 5.5 (0–17) | 0.5 (–1–4) | ||||
| First webspace | 8 | 4.4 (4.6) | 4.6 (4.7) | 0.2 (1.1) | 4.9 (4.8) | 0.5 (1.6) | ||
| 4.4 (0–12) | 4 (0–11) | 0.5 (–1–4) | 4 (0–12) | 0 (–0.5–4.5) | ||||
| Grip strenght | 12 | 15 (–10–90) | 30.0 (0–90) | 10 (0–40) | 0.07 | 10 (–10–90) | 0 (–20–40) | 0.380 |
| 8.8 (2–30) | 6 (0.2–26) | –1.4 (–4.2–6) | 10 (0.9–36) | 0.1 (–4.3–6) | ||||
| Pinch strenght | 13 | 3.5 (2.9) | 3.1 (3.2) | 0.4 (1.1) | 0.195 | 3.3 (3.2) | 0.2 (1.1) | 0.476 |
| 2.2 (0–10) | 1.7 (0–10) | –0.2 (–2.9–1.3) | 2 (0–6) | 0 (–2.7–1.7) | ||||
| Pain | 16 | 2.7 (2.9) | 1.6 (1.7) | 1.1 (1.8) |
| 3.0 (2.6) | 0.2 (1.3) | 0.455 |
| 2.7 (0–6) | 1.5 (0–4) | 0 (–5–2) | 2.5 (0–7) | 0 (–2–3) | ||||
| Hand function | 16 | 1.7 (1.9) | 2.4 (2.9) | 0.7 (1.9) | 0.180 | 2.3 (2.6) | 0.6 (0.5) | 0.206 |
| 1.5 (0–6) | 1.5 (0–9) | 0 (–2–6) | 1.5 (0–9) | 0 (–1–6) | ||||
| Cosmetic | 16 | 3.5 (3.2) | 3.2 (3.3) | 0.2 (2.1) | 0.638 | 3.4 (3.5) | 0.1 (0.5) | 0.791 |
| 3.5 (3.2) | 3.2 (3.3) | 0.2 (2.1) | 3.4 (3.5) | 0.1 (0.5) | ||||
| 3 (0–10) | 2.5 (0–10) | 0 (–3–4) | 3 (0–10) | 0 (–4–5) | ||||
| spasticity | 16 | 7.5 (1.3) | 5.7 (2.2) | 1.8 (1.6) |
| 7.4 (1.7) | 0.0 (1.3) | 0.898 |
| 7.6 (5–10) | 5 (2–10) | –2.1 (–4–2) | 7.5 (3–10) | 0 (–3.5–2) | ||||
| GRT | 8 | 52.8 (35.4) | 71.0 (49.1)* | 18.1 (20.5) | 67.2 (52.7) | 14.4 (20.9) | ||
| 42.5 (16–130) | 66 (15–167) | 24 (–15–38) | 52 (14–181) | |||||
|
| ||||||||
| Subtest 1 | 8 | 28.7 (47.0) | 38.7 (57.7) | 10 (15.2) | 30 (53.2) | 1.2 (8.3) | ||
| 0 (0–130) | 0 (0–150) | 0 (0–40) | 0 (0–150) | 0 (–10–20) | ||||
| Subtest 2 | 8 | 48.7 (46.7) | 71.2 (51.9) | 22.5 (19.1) | 58.7 (50.8) | 10 (15.2) | ||
| 55 (0–130) | 85 (0–150) | 20 (0–50) | 55 (0–150) | 5 (–10–30) | ||||
| Subtest 3 | 9 | 58.9 (59.5) | 89.9 (60.1) | 30 (28.7) | 74.4 (56.4) | 15.5 (17.4) | ||
| 70 (0–150) | 110 (0–150) | 40 (0–80) | 90 (0–150) | 20 (0–50) | ||||
| Subtest 4 | 16 | 87.5 (46.1) | 98.7 (45.6) | 11.2 (15.9) |
| 80.6 (51.8) | –6.9 (26.8) | 0.641 |
| 85 (0–150) | 105 (0–150) | 10 (–10–40) | 85 (0–150) | 0 (–70–20) | ||||
| Subtes 5 | 5 | 84.0 (46.7) | 106.0 (36.5) | 22 (19.2) | 98.0 (50.7) | 14 (20.7) | ||
| 70.0 (30–150) | 110.0 (50–150) | 20 (0–50) | 90 (40–150) | 10 (–10–40) | ||||
| COPM-P | 14 | 2.7 (1.4) | 4.5 (2.2) | 1.7 (1.4) |
| 3.8 (2.1) | 1.0 (0.4) |
|
| 2 (1–6) | 4.8 (1–9) | 1.6 (–0.6–5.0) | 3.5 (1–9) | 0.1 (–0.6–4.0) | ||||
| COPM-S | 12 | 2.1 (1.3) | 4.8 (2.8) | 2.7 (2.1) |
| 3.7 (2.4) | 1.6 (1.5) |
|
| 1.7 (1–5) | 5.6 (1–9) | 2.7 (–0.2–5.4) | 3.4 (1–9) | 1.5 (0.0–4.0) | ||||
| ArmA a | 17 | 14.1 (7.0) | 9.9 (5.9) | 4.1 (4.6) |
| 13.9 (7.8) | 0.2 (4.8) | 0.882 |
| 15 (1–23) | 8 (1–24) | –4 (–14–3) | 15 (1–30) | 0.0 (–6–13) | ||||
| ArmA b | 17 | 43.6 (10.5) | 41.1 (12.6) | 2.5 (7.1) | 0.163 | 42.1 (12.0) | 1.5 (4.3) | 0.175 |
| 49 (15–52) | 48 (9–52) | –1 (–18–16) | 48 (8–52) | 0 (–12–9) | ||||
| Eq5dl | 16 | 57.1 (25.4) | 59.1 (24.2) | 2.0 (16.5) | 0.634 | 66.1 (20.4) | 9.0 (13.9) |
|
| 55(13–100) | 65 (10–100) | 0 (–40–30) | 70 (25–100) | 3 (–10–35) | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBotulinum Toxin and Related Neurological Disorders · Cerebral Palsy and Movement Disorders · Stroke Rehabilitation and Recovery
Spasticity, characterized by involuntary and sustained muscle contractions, is a common complication of stroke, traumatic brain injury (TBI), spinal cord injury (SCI), and other central nervous system (CNS) lesion-inducing conditions (1). A widely used definition of spasticity is a velocity-dependent increase in the tonic stretch reflex (muscle tone) with exaggerated tendon jerks” (2). However, this definition has been challenged, and others have proposed different descriptions in the medical literature; as such, no universally agreed definition is available today. Commonly reported figures estimate that spasticity affects 80% of patients with SCI (3), 60% of patients with TBI (4), and 30–40% of patients with stroke (5).
If left untreated, spasticity can lead to muscle shortening, contractures, joint deformities, pain, impairments in daily activities, and medical and psychological complications. However, in some patients, spasticity can be beneficial, aiding daily functions through key triggering strategies (6). Before planning an intervention, it is important to consider whether spasticity can be helpful in activity performance, or whether it is purely negative for the individual.
Various treatment options exist to manage spasticity, including nonpharmacologic treatments (stretching, muscle strength training, electrical stimulation) (7), pharmacologic treatments (oral medication and intramuscular injections with botulinum toxin (BoNT) (8) and surgical interventions (intrathecal pumps, orthopaedic, and neurosurgery) (9). In many countries, BoNT injections are considered the gold standard of treatment for focal spasticity (10). To optimize the effect of surgical interventions and BoNT injections, treatment is commonly combined with a specific individualized rehabilitation program (adjunct therapies), such as passive and active range of motion (AROM) exercises, splinting, and strengthening exercises, training in activity, and training to correct faulty movement patterns (11).
BoNT injection has been proven to be safe and has been shown to reduce muscle tone and pain and improve passive functions. However, the effect of BoNT injections on active voluntary muscle function remains unclear (12). The surgical procedure used in the present study has been proven to be safe, with negligible complications and has been shown to reduce muscle tone and improve passive function, such as hand hygiene and caregiver burden, and active functions such as grasp ability (13). However, studies evaluating the effectiveness of alternative treatment approaches for adult patients with upper limb (UL) spasticity following CNS injuries in comparison to gold-standard methods, such as BoNT, are lacking. In 1 recent review (14), the authors stated the need for clinical trials comparing surgery with BoNT. Therefore, this study was designed with the primary aim of evaluating the long-term efficacy of spasticity-corrective surgery vs BoNT in patients with disabling UL spasticity. As a secondary aim, we compared the peak effects of the 2 treatments, hypothesizing that surgery would be more beneficial to patients than BoNT in the long term, with respect to function and activity performance (defined as the assessment at 6 months post-surgery and 3 months post BoNT injection). However, we further hypothesized that these methods would produce equivalent improvements when comparing the 6-month postsurgical outcome with the point of maximum benefit of BoNT (5 weeks post-injection).
METHODS
Study design and participants
This study used a pretest-posttest quasi-experimental design. Enrolment began in 2019 and was completed in June 2024. Owing to the Covid-19 pandemic, inclusion was halted between March 2020 and February 2022. The eligibility criteria for this study were as follows: (i) 18 years or above; (ii) problematic spasticity, characterized by a velocity-dependent increase in tonic stretch reflexes or intermittent or sustained involuntary muscle activity in the UL after stroke, TBI, or SCI; and (iii) patients treated at least 6 months after the injury event; and (iv) ongoing BoNT treatment in the UL, (v) a minimum of 3 months passed since the last BoNT injection: (vi). At least two muscles in the hand and wrist were considered for treatment (vii). For the BoNT group, a community occupational or physical therapist was assigned for post BoNT treatment; (viii) For the surgery group, medically stable to undergo surgery; (ix) No other severe UL injuries affecting the functional level.
Study participants were recruited using 2 parallel procedures: (i) Review of a hospital-based register of patients who had been treated or referred to the tonus clinic identified eligible patients, who were then sent information about the study, along with their contact information to the researcher responsible for the study. (ii) Patients with ongoing BoNT treatment who had been referred to the Center for Advanced Reconstruction of Extremities (C.A.R.E.), and were eligible for the present study were informed about the study and enrolment procedure. All presumptive study participants underwent a screening procedure by a primary examiner, to assess whether they met the study’s eligibility criteria. Further information regarding the study was provided at this point, with the opportunity to ask questions. Written informed consent was obtained if the patient met the inclusion criteria and consented to participate. All patients were offered either of the 2 treatment methods, while the treatment allocation was based on individual preferences. The flowchart of this study is presented in Fig. 1. All procedures were performed in compliance with relevant laws and institutional guidelines and were approved by the Regional Ethical Review Board in Gothenburg (No. 999-18) on 17 December 2018. The study was conducted in accordance with relevant ethical guidelines (Declaration of Helsinki).
Flowchart of patient enrollment, treatment, and follow-up in botulinum toxin (BoNT) and surgery groups. (Explanation: This figure outlines the process of patient enrollment, treatment, and follow-up for individuals assigned to either the Botulinum Toxin (BoNT) group or the Surgery group. The flowchart provides a step-by-step overview, starting from the initial review of medical records to the final analysis of results. CARE: Center for advanced reconstruction of extremities; BoNT: Botulinum toxin; n = number).
Interventions
Spasticity-corrective surgery. Surgical treatment was conducted as part of the routine care at C.A.R.E, Sahlgrenska University Hospital/Mölndal. Surgery included lengthening or releasing a tendon from its insertion, resulting in the consequent relaxation of the entire muscle-tendon unit; hence, the degree of muscle tension is reduced. The spasticity correction procedures were performed using a stair-step incision technique, followed by reattachment in the lengthened position using a side-to-side cross-stitch technique (15). The degree of tendon lengthening was decided by aiming for a normal resting length, which was estimated at full relaxation during general anaesthesia and with the remembrance of the preoperative status; 2–3 cm was usually sufficient. The day after surgery, wrapping and custom-made splints were fashioned to facilitate prolonged soft tissue stretching and prevent postoperative oedema. When possible, AROM exercises of the antagonist muscles of the lengthened muscles were performed on the first day after surgery, as was passive or AROM activation of the treated muscles. AROM exercises were allowed to achieve the maximum ROM, with no restrictions on the lengthened muscles or their antagonists. All patients returned to the ward 3 weeks after surgery for follow-up and inpatient rehabilitation of varying lengths, depending on the treatment regimen. Three weeks after surgery, splints were only used at night until 3 months after surgery, and were readjusted if needed. The continued training was individually tailored to meet each patient’s goals. The treatment concept used in this study has been previously described in detail (13, 16).
Botulinum toxin treatment. BoNT treatment was administered as part of routine care at the Tonus Clinic, Rehabilitation Medicine, Sahlgrenska University Hospital/Högsbo. All patients had previously received BoNT injections, and only 1 injection cycle was used in this study. All injections were performed by an experienced physician with a special interest in spasticity. Electrical stimulation (ES) was used for muscle localization using a hollow insulated monopolar needle connected to a portable ES machine. The approximate location of the target muscle was determined using standard anatomic landmarks. Once the needle electrode was positioned in the target muscle, ES was delivered through the needle electrode to the muscle to produce muscle contraction. The visual feedback of appropriate muscle contraction confirmed that the needle electrode was likely in the target muscle, and the appropriate botulinum BoNT dose was injected. For some of the patients, ultrasound (US) guidance was used for musculoskeletal procedural guidance in addition to ES. BoNT blocks certain chemical signals from the nerves, resulting in temporary relaxation of muscles. Normally, the effect wears off after 3 months, and its maximum (peak) effect typically occurs 4–6 weeks after injection (10). In the present study, the dose and number of injected muscles varied depending on the degree and extent of spasticity. The post-injection treatment protocol varied but commonly involved stretching, strength training of the antagonists, and, in some cases, splinting.
Effects and functional implications of spastic muscles. Spasticity in muscles can profoundly affect posture, breathing, and upper-body function. Spastic pectoral muscles promote shoulder internal rotation and adduction, leading to poor posture, restricted breathing, and challenges with dressing and washing the upper body.
Spasticity in the elbow flexors (biceps brachii, brachioradialis, and brachialis) keeps the elbow flexed and the forearm supinated (due to the biceps brachii), restricting reach and grasp. This can impair balance and walking and interfere with hygiene and dressing of the upper body.
The pronator teres, when spastic, forces the arm into a pronated position, making object grasping difficult and leading to compensatory shoulder movements during hand use.
Spastic wrist flexors (flexor carpi radialis, flexor carpi ulnaris, and palmaris longus) hold the wrist in a flexed position, making grasping difficult and sometimes interfering with dressing.
Spastic finger flexors (flexor digitorum superficialis and flexor digitorum profundus) cause the fingers to remain clenched, making it difficult to open the hand, release objects, maintain hand hygiene, or cut fingernails.
Thumb flexor spasticity pulls the thumb into the palm, preventing key pinch and making it difficult to hold or place objects in the hand. An overactive thumb abductor positions the thumb too close to the index finger, restricting cylindrical grasp and pinch. Additionally, spastic intrinsic muscles keep the metacarpophalangeal (MCP) joints flexed, further restricting hand opening.
The treated muscles of the 2 groups are presented in Fig. 2. Table II presents the target muscles and the objectives with the treatment, case by case, and Table III presents the effects and functional implications of spastic muscles.
Distribution of target Muscles in surgery and Botulinum toxin treatment groups. (Explanation: The figure illustrates the distribution of muscle involvement between the 2 groups, Surgery and Botulinum Toxin (BoNT). The numbers indicate the count (n) and percentage (%) of patients in each group whose specific muscles were treated. Each group consisted of 17 patients. Abbreviation: Surg group: surgery group; BoNT group: Botulinum Toxin group; n: number).
Outcome measures
The baseline data included demographics, clinical characteristics, and study-specific measurements. Owing to the differing time-course effects of BoNT and surgery, the assessment time points differed between the groups. For the primary research question (long-term effectiveness), the primary time point for the surgery group was the assessment at 6 months post-surgery and 3 months post-injection for the BoNT group, with an additional assessment at 1–5 weeks post-injection to capture the peak effects. The collected data included treated muscles, side effects, medication changes, and events from baseline to follow-up that could have affected the results. Participants also rated their satisfaction and perceived exertion with the treatment on a visual analogue scale (VAS) at the long-term follow-up.
All measures included in this study were based on the International Classification of Functioning, Disability, and Health (ICF) constructs (17). The primary outcome measure was muscle tone, measured using the Modified Ashworth Scale (MAS). The single-item MAS was measured on a 6-point scale from 0 (no increase in muscle tone) to 4 (affected part rigid in flexion or extension), with an additional point allocated at 1+ (slight increase in muscle tone). As such, the MAS provides a single score to represent spasticity in a specific movement. For analysis, the MAS scores of the treated muscles were summed to obtain a “composite spasticity score” for each participant.
Secondary outcomes included measures within the following ICF domains
Body function. Self-rated pain intensity and experienced UL spasticity were measured using a VAS (18). AROM and passive range of motion (PROM) in the target joints were measured using a handheld goniometer in a sitting position, following a standard procedure (19). The capacity to achieve passive and active hand opening was rated using the following scale: hand closed, ¼ open, ½ open, ¾ open, or fully open. For analysis, the scale was scored from 0 (hand-closed) to –5 (fully open). The same grading system was applied to describe the resting position of the hands (20). Maximum handgrip strength was measured with a hydraulic hand dynamometer (JAMAR^®^ 5030J1, Sammons Preston Rolyan, USA) (21). Maximum pinch grip strength was measured using a Preston Pinch Gauge (European Bissel Healthcare Ltd., Winchester, England) (21).
Activity. The ability to grasp, move, and release objects was measured using the Grasp and Release Test (GRT) (22). The ability to actively and/or passively open one’s hand and actively grasp and release a cylindrical object was measured using a Cylinder Test. The test was divided into 5 subtests; (i) active cylinder grip-normal, (ii) active cylinder grip-adapted, (iii) active cylinder grip self-assisted, (iv) passive cylinder grip-self-assisted, and (v) passive cylinder grip-examiner-assisted. Self-rated arm and hand function (usefulness) were measured using the VAS (18). The Arm-Activity Measure (ArmA) questionnaire was used to capture difficulties in passive and active real-life arm functions (23).
Participation. Limitations in the prioritized daily activities were measured using the Canadian Occupational Performance Measure (COPM). The patients’ health-related quality of life (HRQoL) was assessed using the EuroQol 5-dimension questionnaire (EQ5D 5 L) (24).
Sample size calculation
The calculation of sample size was based on the a priori defined difference to be detected, with an alpha level of 5% and a power goal of 80%, as well as the primary outcome variable MAS and previous findings (25, 26). The estimated changes in MAS-score in the surgery and BoNT groups were –1.3 standard deviation (SD) (0.7) and –0.6 (0.5), respectively. Based on this estimate, for the results to satisfy a power criterion of 80%, at least 14 participants were required in each of the 2 groups. We expected a dropout rate of 15%, and therefore aimed to include 17 individuals in each group to achieve 80% power.
Statistical analyses
The demographic and baseline characteristics of the study participants were summarized using descriptive statistics. Due to the small number of participants, nonparametric tests were used. Significant analyses were conducted for outcome measures with 10 or more data points. Between-group differences in treatment efficacy were analysed by comparing pretest-posttest changes. The Mann-Whitney U-test was used for all comparisons. The main effect size was calculated using the equation r = Z/√N. For interpretation, the following guidelines were applied: an effect size r less than 0.3 indicates a small effect; r between 0.3 and 0.5 indicates a medium effect; and r greater than 0.5 indicates a large effect. The Wilcoxon signed-rank test was used for within-group treatment efficacy analyses. The statistical significance was set at 5%. The Holm-Bonferroni method was applied to reduce the possibility of Type I errors resulting from testing multiple hypotheses. To enable a comparison with previously reported findings, the results are presented using both mean values and medians.
RESULTS
Seventeen patients in each group were included in the final analysis; the study flow is presented in Fig. 1.
The mean ages of the surgery and BoNT groups were 60 (26–76) and 55 (24–81) years, respectively, while the male: female ratios were 12:5 and 9:8, respectively. The detailed clinical characteristics of the 2 groups are presented in Table I.
Six participants (2 in surgery group, 4 in BoNT group) reported changes in their routine or health condition which may have influenced the study results. In the surgery group, 1 participant’s focus on rehabilitation was negatively impacted by a family member’s stroke, while another had a reduction in their baclofen dose. In the BoNT group, 1 participant who had previously combined BoNT with intensive rehabilitation did not do so this time, another had an intensive rehabilitation period, and 2 participants had less training due to the pandemic.
The most commonly treated muscles in the surgery group were the finger flexors, wrist flexors, thumb flexors, and pronator teres. In the BoNT group, the most commonly targeted muscles were the fingers, wrist, thumb, and elbow flexors.
Primary outcome measure
Between-group analyses revealed that surgery produced significantly greater improvement in MAS scores from baseline to follow-up compared to the BoNT group at both the peak and 3-month assessments (p < 0.001). The effect sizes were r 0.78 and r 0.85 between the surgery and BoNT peak and long-term assessment, respectively, indicating large effects.
The within-group analyses demonstrated a significant reduction in the MAS score for the surgery group at 6 months, –2.7 (0.8), p < 0.001 and for the BoNT group at the peak assessment –1.1 (0.6), p < 0.001. In the long-term assessment, beneficial gains in MAS were still present in the BoNT group, yet diminished by –0.3 (0.5) p = 0.02. Fig. 3 summarizes the changes in the MAS scores.
*Comparison of mean differences in Modified Ashworth scale composite scores between surgery and Botulinum Toxin treatment groups. Explanation: This box plot illustrates the mean differences in MAS composite scores among 3 groups: the surgery group, BoNT peak assessment group, and BoNT long-term assessment group. The MAS score is a measure used to evaluate muscle spasticity, with lower scores indicating reduced spasticity. The box plot provides the median, interquartile range, and the overall range (whiskers) of the MAS scores for each group. The comparison highlights the differences in the effectiveness of the treatments over different periods, with the surgery group showing the most substantial reduction in MAS scores, followed by the BoNT peak and BoNT long-term assessments. *Indicates significantly difference below 0.005, *indicates significantly difference below 0.001. Abbreviation: MAS: modified Ashworth scale; BoNT: Botulinum toxin.
Secondary outcome measures
Between treatment groups. In the between-group analyses of secondary outcomes, the surgery group demonstrated significantly greater improvements than the BoNT group in 7 of the 17 secondary outcomes (peak assessment), including the resting position of the hand, pinch strength, perceived hand function, perceived spasticity, passive opening of the hand (subtest 4 of the cylinder test), and passive and active real-life arm function (Arma A and B). After applying the Holm-Bonferroni adjustment, 5 outcomes still showed significant improvement (Table IV). In the long-term assessment, 11 outcomes showed significant differences between the surgery and BoNT groups, with results in favour of the surgery group. After Holm-Bonferroni adjustment, 7 outcomes were still significantly improved: active opening of the hand, resting position of the hand, pinch strength, perceived spasticity, passive opening of the hand (subtest 4 of the cylinder test), and passive and active real-life arm function (Arma A and B, Table IV).
Following treatment completion, all patients were asked to rate their satisfaction with the results on a VAS, as well as how demanding they perceived the treatment. They were also asked as to whether they would recommend the treatment to someone else (yes or no). The mean satisfaction score was 7.4 (1.8) and 5.9 (2.6) in the surgery and BoNT groups, respectively. The mean score of how demanding they perceived the treatment was 3.5 (2.8) in the surgery group and 3.5 (3.2) in the BoNT group. Seventeen patients would recommend surgery to others, while 15 would endorse BoNT injections. However, 2 patients would not recommend BoNT treatment.
Within the treatment group. The findings of the secondary outcome measures are presented in Table VA–B. Within-group analyses demonstrated that the participants who underwent surgery showed significantly greater improvements in 21 of the 26 secondary outcomes. After applying the Holm-Bonferroni adjustment, 11 outcomes remained significantly improved. Within-group analyses revealed significant improvements in 10 out of 18 secondary outcomes in the BoNT group (peak assessment) and 3 out of 18 in the long-term assessment. After applying the Holm-Bonferroni adjustment, 5 outcomes remained significantly improved at the peak assessment and 2 at the long-term assessment.
DISCUSSION
The findings of the present study indicate that spasticity-corrective surgery produces beneficial gains that exceed and last beyond those achieved with BoNT. Primarily, surgery appears to suppress the symptoms of spasticity, as measured by the MAS, to a greater extent than BoNT. The mean reduction in the composite MAS score was significantly higher in the surgery group than in the BoNT group at both the peak and long-term assessments. These results are in accordance with prior studies investigating the efficacy of tendon lengthening techniques in reducing muscle hypertonia (13, 26, 27), and contribute to the existing body of knowledge in the field.
Surgery was associated with significant improvements that exceeded those achieved in the BoNT group in the MAS primary outcome and many secondary outcome measures. Specifically, surgery showed superior results in 7 of 17 secondary outcomes compared to the peak effect of BoNT, and in 11 of 17 secondary outcomes compared to the long-term effect of BoNT. These findings indicate that surgery not only reduces spasticity, but also enhances UL use. Although previous studies have shown that the effect of BoNT on active voluntary muscle function is limited (12), other studies have revealed that surgery improves active voluntary muscle function (13, 26, 28, 29), which is consistent with our findings.
The long-term effect of surgery compared with that of BoNT is anticipated to be more effective, as demonstrated in the present study. The peak effect of BoNT is transient, typically lasting for approximately 3 months. While BoNT showed significant improvements at the peak effect, these gains decreased over time, necessitating repeated injections to maintain the associated benefits. In contrast, surgical intervention requires an initial higher input from healthcare and patient but provided lasting improvements, reduced the need for continuous medical interventions, and potentially lowered associated healthcare costs. While further studies are required to determine the exact duration of these effects, prior studies have shown lasting results up to 6 years postoperatively (27).
Patient satisfaction ratings of the treatments confirmed the quantitative findings, with higher satisfaction scores in the surgical group (Mean VAS score=7.4 vs 5.9). Although both groups found their respective treatments equally demanding, the willingness of all 17 patients in the surgery group and most patients in the BoNT group to recommend the procedure to others highlighted the perceived value and acceptability of surgery and BoNT as treatment options for spasticity.
The results of the present study have significant implications for clinical practice, indicating that spasticity-corrective surgery should be considered as a treatment option for patients with UL spasticity, particularly when long-term management is the goal. Although BoNT remains a valuable tool for both immediate and short-term relief, its limitations in sustaining functional improvements necessitate the exploration of surgical options for eligible patients. Prior studies have emphasized the need for improved spasticity management (3, 7, 30, 31). Surgery is generally considered in severe cases, or as the last option for adult patients when noninvasive treatments fail (32), and is sometimes not mentioned as an option at all (33, 34). A recent review of focal spasticity management recommended surgery in 4 of 13 papers (35). The underutilization of UL surgery has been criticized by surgeons who see it as a missed opportunity (36–39). The reasons for this underutilization include a lack of knowledge about surgical options, a variety of procedures without a clear algorithm, limited outcome evidence or consensus, unfavourable past experiences, limited access to surgery, and insufficient collaboration between surgeons and rehabilitation therapists (36, 38). It is estimated that 10% of patients with spasticity could benefit from surgery (37). Some surgeons advocate considering surgery in patients with significant spasticity (36). Reports indicate that less than 1% of patients with TBI or stroke with residual spasticity undergo surgery (38). The promising results of this study could lead to increased referrals and evaluations of surgery as a treatment option for spasticity.
It is essential to note the individualized nature of spasticity management, in which treatment plans should consider patient-specific factors, including the severity of spasticity, functional and activity goals, and overall health status. One multidisciplinary approach integrating surgical interventions with comprehensive rehabilitation programs can optimize outcomes and enhance the quality of life of patients with CNS-induced spasticity.
Limitations and future research
This study has several limitations that should be considered. Firstly, the quasi-experimental design and relatively small sample size of this study warrant cautious interpretation of our findings. Allocation based on patient preferences, while reflecting real-world scenarios, may introduce a selection bias. Future randomized controlled trials (RCT) with larger cohorts are required to confirm these results, and to further explore the comparative effectiveness of different spasticity management strategies (40). The surgical field has lagged behind other specialities in performing RCTs (41). Indeed, it has been reported that only 7% of articles published in surgical journals are RCTs (40). The reasons for the lack of RCTs on surgery include ethical issues, patient and surgeon preferences, irreversibility of surgical treatment, increased expense and follow-up time, and difficulty with randomization and blinding. In a review of meta-analyses (40), the authors concluded that the results of well-designed observational studies did not systematically overestimate the magnitude of the effects of treatment compared with those of RCTs on the same topic. Another limitation is that the outcome assessors were not blinded. Owing to the physical components of interventions, blinding is not easily applicable in surgical studies.
In the present study, the Holm–Bonferroni method was used for multiple statistical tests. Sample size calculations were not performed for secondary outcome measures or subgroup analyses; therefore, we may have failed to detect some important treatment effects. Therefore, the results should be interpreted with caution. Patients with varying levels of residual muscle function (different treatment regimens) and diagnoses were analysed. In the surgery group, 47% of the patients suffered from a SCI, whereas the proportion of individuals with SCI was limited to 6% in the BoNT group. In the surgery group, 29% were stratified into the HFR group compared to 35% in the BoNT group. To address the issue of differing clinical characteristics between the 2 treatments, a future experimental study using a paired design, in which different treatment regimens are analysed separately, could be of significant interest.
Overall, the findings of the present study suggest that surgical options should be included in the treatment paradigm for spasticity, tailored to the individual needs of the patient, and complemented by targeted rehabilitation programs. The high patient satisfaction ratings further validated our quantitative findings, with higher satisfaction scores and a unanimous willingness to recommend surgical treatment, demonstrating its acceptability and perceived value. The implications for clinical practice are profound, advocating for the inclusion of surgical options in spasticity management paradigms, particularly for patients seeking long-term improvements in UL function.
Conclusion
Spasticity-corrective surgery produces beneficial gains that exceed and last beyond those achieved with BoNT in patients with disabling UL spasticity. The composite MAS scores were higher in the surgical group. Although BoNT remains a valuable tool for immediate relief, its transient nature necessitates repeated interventions, making surgery a more viable long-term solution for managing spasticity. The study’s quasi-experimental design and small sample size warrant a cautious interpretation of the results. Future studies with larger cohorts are essential to confirm these findings and further explore the comparative effectiveness of different spasticity management strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mayer NH, Esquenazi A. Muscle overactivity and movement dysfunction in the upper motoneuron syndrome. Phys Med Rehabil Clin N Am 2003; 14: 855–883. 10.1016/S 1047-9651(03)00093-714580042 · doi ↗ · pubmed ↗
- 2Lance JW. The control of muscle tone, reflexes, and movement: Robert Wartenberg Lect. Neurol 1980; 30: 1303–1313. 10.1212/WNL.30.12.13037192811 · doi ↗ · pubmed ↗
- 3Holtz KA, Lipson R, Noonan VK, Kwon BK, Mills PB. Prevalence and effect of problematic spasticity after traumatic spinal cord injury. Arch Phys Med Rehabil 2017; 98: 1132–1138. 10.1016/j.apmr.2016.09.12427780743 · doi ↗ · pubmed ↗
- 4Wedekind C, Lippert-Grüner M. Long-term outcome in severe traumatic brain injury is significantly influenced by brainstem involvement. Brain Inj 2005; 19: 681–684. 10.1080/0269905040002518216195181 · doi ↗ · pubmed ↗
- 5Zeng H, Chen J, Guo Y, Tan S. Prevalence and risk factors for spasticity after stroke: a systematic review and meta-analysis. Front Neurol 2020; 11: 616097. 10.3389/fneur.2020.61609733551975 PMC 7855612 · doi ↗ · pubmed ↗
- 6Zorowitz DR, Gillard JP, Brainin JM. Poststroke spasticity: Sequelae and burden on stroke survivors and caregivers. Neurology 2013; 80: 45–52. 10.1212/WNL.0b 013e 3182764 c 8623319485 · doi ↗ · pubmed ↗
- 7Khan F, Amatya B, Bensmail D, Yelnik A. Non-pharmacological interventions for spasticity in adults: an overview of systematic reviews. Ann Phys Rehabil Med 2017; 62: 265–273. 10.1016/j.rehab.2017.10.00129042299 · doi ↗ · pubmed ↗
- 8Howard IM, Patel AT. Spasticity evaluation and management tools. Muscle Nerve 2023; 67: 272–283. 10.1002/mus.2779236807901 · doi ↗ · pubmed ↗