Functional Reconstruction of Lower Eyelid Using Paramedian Forehead Flap Combined with Frontalis Muscle and Periosteum
Riku Katayama, Takako Fujii, Chie Kanayama, Hisashi Sakuma

TL;DR
This case report describes a two-stage surgical method to reconstruct the lower eyelid using a forehead flap combined with muscle and periosteum for functional and cosmetic recovery.
Contribution
A novel two-stage technique combining paramedian forehead flap with frontalis muscle and periosteum for lower eyelid reconstruction is presented.
Findings
The transferred frontalis muscle showed voluntary contraction during eyelid closure six months post-surgery.
Electromyography confirmed neurotization of the transferred muscle one year after the procedure.
The method effectively reconstructed horizontal skin defects involving the orbicularis oculi muscle.
Abstract
Both cosmetic and functional aspects are important in reconstructing the lower eyelid tissue defects. In this case report, we describe a two-stage reconstruction of a skin defect, including the orbicularis oculi muscle, after resection of a basal cell carcinoma using a paramedian forehead flap combined with the frontalis muscle and periosteum. In the first stage, the paramedian forehead flap, including the frontalis muscle and periosteum, was elevated, the periosteal flap was fixed to the outer orbital periosteum to lift the lower eyelid, and the skin flap, including the frontalis muscle, was sutured to the defect. In the second stage, the flap was divided and the frontalis muscle flap was sutured to the medial palpebral ligament. Electromyography at 1 year postoperatively confirmed neurotization of the transferred muscle, and at 6 months, voluntary contraction of the transferred muscle…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
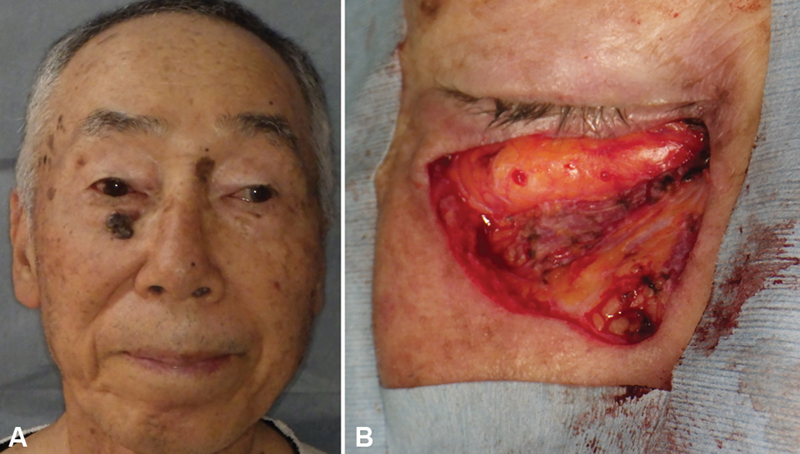 Fig. 1
Fig. 1 Fig. 2
Fig. 2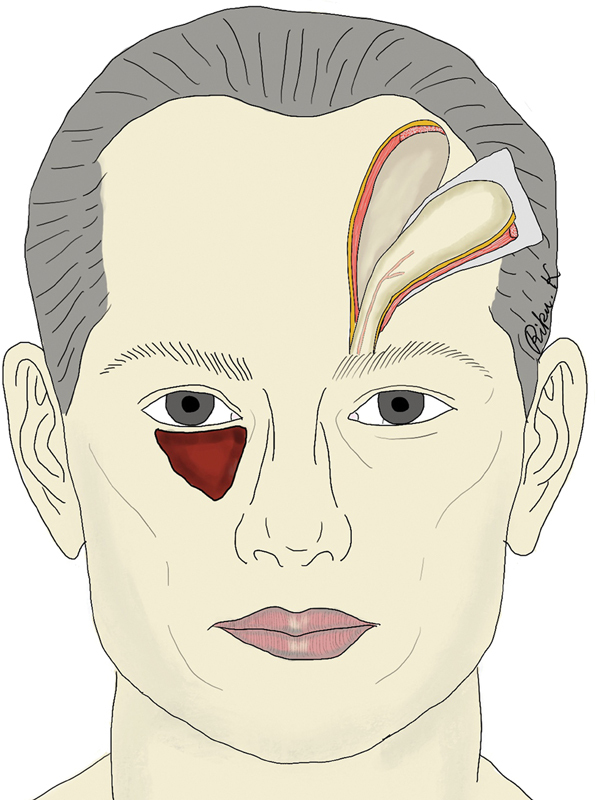 Fig. 3
Fig. 3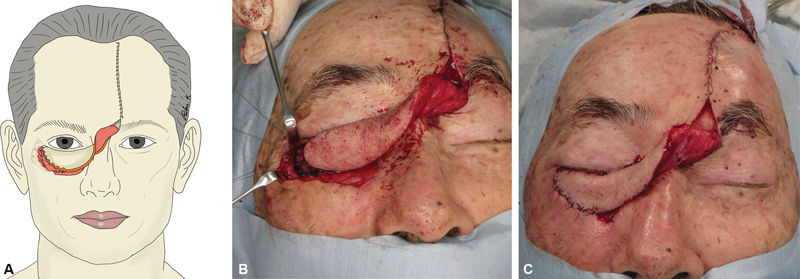 Fig. 4
Fig. 4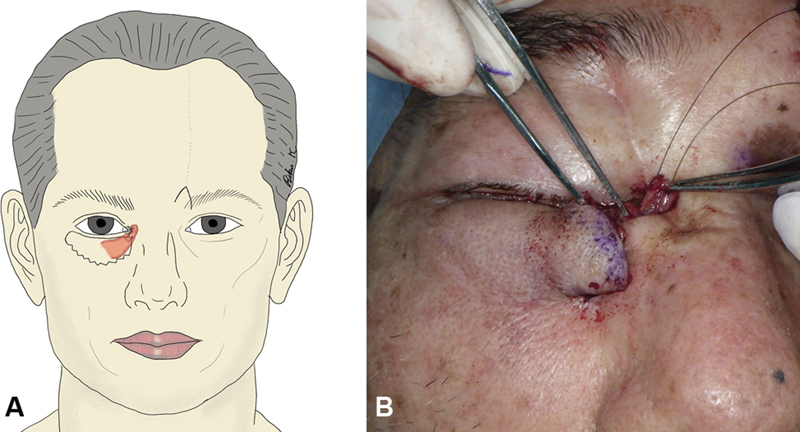 Fig. 5
Fig. 5 Fig. 6
Fig. 6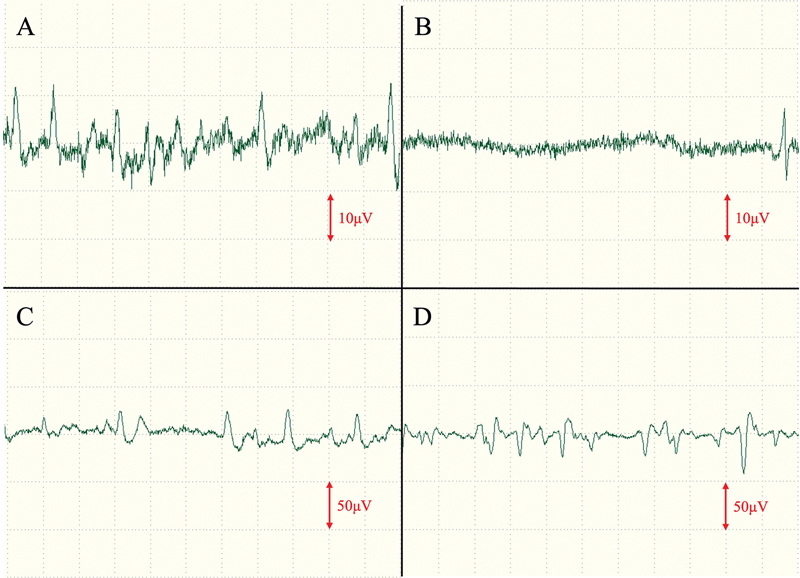 Fig. 7
Fig. 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFacial Rejuvenation and Surgery Techniques · Reconstructive Facial Surgery Techniques · Facial Nerve Paralysis Treatment and Research
Introduction
When reconstructing lower eyelid defects, it is necessary to consider not only cosmetic aspects but also the prevention of lower eyelid ectropion and eyelid closure dysfunction. We herein report a case in which the lower eyelid skin and orbicularis oculi muscle were lost due to basal cell carcinoma resection and were successfully reconstructed using a paramedian forehead flap combined with the frontalis muscle and periosteum, resulting in good lower eyelid morphology and function. The patient involved in this study signed an informed consent form after a detailed explanation of the benefits and risks of the procedure was provided.
Case
Video 1 Video showing eyebrow elevation and eyelid closure at 6 months postoperatively.
The patient was a 75-year-old man, who was aware of a black lesion on his right lower eyelid for approximately 5 years. After the biopsy, the patient was diagnosed with basal cell carcinoma, and resection was performed. The tumor measured 22 mm × 20 mm, the margin was set at 5 mm, and the orbicularis oculi muscle was excised. An artificial dermis made from collagen (Integra®; Integra LifeSciences Corporation, NJ), equipped with drainage holes, was applied to the resected area. This artificial dermis acted as a temporary dressing until pathology results were confirmed, with the dual purpose of minimizing scar contracture of the lower eyelid and optimizing wound bed preparation for subsequent surgery. After pathological examination confirmed negative surgical margins, the patient underwent reconstruction 27 days after the initial surgery ( Fig. 1 and Supplementary Fig. S1 [available in the online version only]). The patient provided informed consent for the use of his medical information, including photography and video, for this case report and publication.
Pre- and post-resection images of the tumor. ( A ) Photograph of the tumor prior to resection. ( B ) Post-resection image of the tumor, showing the excision of both the tumor and the orbicularis oculi muscle.
Due to the significant loss of the orbicularis oculi muscle and the expected postoperative development of lower eyelid ectropion, a paramedian forehead flap with frontalis muscle and periosteum was used. The flap, sourced from the contralateral side and pedicled by the supratrochlear artery, was chosen to align the frontalis muscle with the course of the orbicularis oculi muscle after the transfer. The skin island was designed to be 2.5 cm wide and 8.0 cm long, and slightly outward, in line with the running of the frontalis muscle ( Fig. 2 and Supplementary Fig. S2 [available in the online version only]).
Design of the paramedian forehead flap.
The periosteum was slightly larger than the skin island, and the flap was dissected under the periosteum ( Fig. 3 and Supplementary Figs. S3 and S4 [available in the online version only]). The periosteum was fixed to the outer orbital periosteum with a nonabsorbable thread and used to suspend the lower eyelid. The frontalis muscle was sutured to the residual orbicularis oculi stump to increase the adhesive area. The skin island and surrounding skin were created with a zigzag incision to prevent a trapdoor deformity ( Fig. 4 ).
Schematic representation of the flap elevation procedure.
Flap suturing process. ( A ) Schematic view. ( B ) Intraoperative photograph showing the suturing of the periosteum to the outer orbital periosteum. ( C ) Postoperative photograph.
Twenty-seven days after flap elevation, flap division was performed, and good bleeding was observed from the stump of the transferred frontalis muscle. A “W” incision was made in the medial canthus, and the stump of the transferred frontalis muscle was sutured to the medial palpebral ligament using a nonabsorbable thread ( Fig. 5 ).
Flap division procedure. ( A ) Schematic view. ( B ) Intraoperative photograph showing the suturing of the frontalis muscle to the medial palpebral ligament.
At 6 months postoperatively, the lower eyelid morphology was good, with no evidence of eyelid closure disorders, although a mild degree of ectropion persisted ( Fig. 6 and Supplementary Fig. S5 [available in the online version only]). During eyelid closure, the transplanted frontalis muscle showed voluntary movements ( Video 1 ), and an electromyogram was performed 3 months and 1 year postoperatively to evaluate the neural reinnervation of the transferred frontalis muscle. The results showed a partial resting denervation potential, with voluntary contraction displaying almost the same amplitude as the normal side, suggesting neurotization of the frontalis muscle ( Fig. 7 ). Perceptual evaluation using the Semmes–Weinstein monofilament showed G (3.84) perception at 3 months postoperatively and B (2.36) perception at 1 year postoperatively in the central area of the skin island.
Photograph at 6 months postoperatively.
Electromyogram results at 1 year postoperatively. ( A ) Normal side, rested. ( B ) Skin island, rested. ( C ) Normal side, eyelid closed. ( D ) Skin island, eyelid closed.
Discussion
Although local flaps, such as the malar and lateral orbital propeller flaps, have been reported as reconstruction methods for lower eyelid defects, the reach of the flap is limited when the defect is horizontal and extends to the medial canthus. 1 2 3 In addition, it is necessary to prevent postoperative lower eyelid ectropion in patients with orbicularis oculus muscle defects. The surgical procedure reported here has the advantage that not only can the lower eyelid be suspended by a periosteal flap, but the orbicularis oculi muscle defect can also be reconstructed with the muscle. The frontalis muscle is considered to have a dehiscence in the midline of the frontal forehead. By designing a skin island toward the lateral side of the head, it is possible to elevate the skin flap in accordance with the running of the frontalis muscle while simultaneously increasing the length of the skin flap. 4 5 6 The paramedian forehead flap is effective in reconstructing extensive defects of the lower eyelid, especially those with a vertical dimension of approximately 2 cm. 7 8 9 10 The forehead flap used for eyelid reconstruction, while effective, lacked pliability and remained somewhat thick when the eye was closed. Nevertheless, the color and texture of the flap matched that of the lower eyelid, and in this case, the patient did not report any concerns or requests for revision regarding scarring at the frontal donor site. It should also be noted that the defect, in this case, was not full-thickness, and partial loss of the orbicularis oculi muscle may not always necessitate reconstruction of the muscle layer. The decision to proceed with this reconstruction was made after providing a thorough explanation and obtaining informed consent from the patient. Furthermore, this method may not be suitable for all similar defects.
Neurotization by collateral sprouting has been reported in the past. In the present case, muscle-to-muscle neurotization (muscular neurotization) from the surrounding residual orbicularis oculi muscle to the transferred frontalis muscle or nerve-to-muscle neurotization (direct intramuscular neurotization) from a small branch of the cut zygomatic branch of facial nerve to the transferred frontalis muscle might have occurred. 11 Neurotization may prevent ectropion by maintaining muscle tone at rest and reconstructing dynamic function during eyelid closure. Although there have been several reports on lower eyelid reconstruction using a paramedian forehead flap, our case is the first to report the use of a paramedian forehead flap combined with the frontalis muscle and periosteum, as well as the possibility of neurotization of the transferred frontalis muscle.
Despite its disadvantages, such as scarring in the frontal area and being a two-stage procedure, the paramedian forehead flap with the frontalis muscle and periosteum is a useful reconstruction method for vertically extensive lower eyelid tissue defects, including the orbicularis oculi muscle, because it delivers both cosmetic and functional restoration of the lower eyelid. However, the postoperative persistence of mild ectropion in the lower eyelid highlights the need for further refinement of the surgical technique.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ding J P Chen B Yao J Lateral orbital propeller flap technique for reconstruction of the lower eyelid defect Ann R Coll Surg Engl 201810005 e 103e 10529607727 10.1308/rcsann.2018.0005 PMC 5956590 · doi ↗ · pubmed ↗
- 2Kim K P Sim H S Choi J H The versatility of cheek rotation flaps Arch Craniofac Surg 2016170419019728913282 10.7181/acfs.2016.17.4.190PMC 5556835 · doi ↗ · pubmed ↗
- 3Ogawa Y Takemoto T Suzuki K Kusumoto K Application of the lateral orbital flap to reconstruction of the upper and lower eyelids and the eye socket after enucleation Ann Plast Surg 2011660436036320841995 10.1097/SAP.0b 013e 3181 d 9aa 21 · doi ↗ · pubmed ↗
- 4Raveendran S S Anthony D J Classification and morphological variation of the frontalis muscle and implications on the clinical practice Aesthetic Plast Surg 2021450116417032926184 10.1007/s 00266-020-01937-2 · doi ↗ · pubmed ↗
- 5Costin B R Plesec T P Sakolsatayadorn N Rubinstein T J Mc Bride J M Perry J D Anatomy and histology of the frontalis muscle Ophthalmic Plast Reconstr Surg 20153101667225417794 10.1097/IOP.0000000000000244 · doi ↗ · pubmed ↗
- 6Spiegel J H Goerig R C Lufler R S Hoagland T M Frontalis midline dehiscence: an anatomical study and discussion of clinical relevance J Plast Reconstr Aesthet Surg 2009620795095418468501 10.1016/j.bjps.2007.10.087 · doi ↗ · pubmed ↗
- 7Ang T W Juniat VO'Rourke M The use of the paramedian forehead flap alone or in combination with other techniques in the reconstruction of periocular defects and orbital exenterations Eye (Lond)2023370356056535241795 10.1038/s 41433-022-01985-9PMC 9905546 · doi ↗ · pubmed ↗
- 8Gupta R John J Hart J Chaiyasate K Medial canthus reconstruction with the paramedian forehead flap Plast Reconstr Surg Glob Open 20221007 e 441935919689 10.1097/GOX.0000000000004419 PMC 9278924 · doi ↗ · pubmed ↗