
TL;DR
A 12-year-old girl with a vegetarian diet was diagnosed with frontal lobe cysticercosis after experiencing seizures and cognitive decline due to a brain cyst.
Contribution
This case highlights the atypical cognitive symptoms and diagnostic challenges of cysticercosis in non-meat-eaters.
Findings
A CT scan confirmed a frontal lobe cyst containing a hyperdense scolex in a vegetarian patient.
Treatment with valproic acid, prednisolone, and albendazole resolved seizures over 24 months.
The case emphasizes the need to consider cysticercosis in patients with atypical cognitive symptoms and pig exposure.
Abstract
Cysticercosis, a brain infection caused by the parasite Taenia solium, presents considerable health challenges, especially in tropical and developing areas, where it contributes significantly to the incidence of epilepsy. The lifecycle of this parasite involves humans as the primary hosts and pigs as the intermediate hosts. In this case study, a 12-year-old girl exhibited unusual symptoms, such as fainting episodes and a decline in academic performance. Although she adhered to a vegetarian diet, her contact with pigs resulted in an infection, confirmed by a CT scan that revealed a cyst in the right frontal lobe containing a hyperdense scolex. The treatment regimen included valproic acid, prednisolone, and albendazole, which successfully resolved her seizures over a follow-up period of 24 months. This case underscores the diagnostic challenges associated with cysticercosis and highlights…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
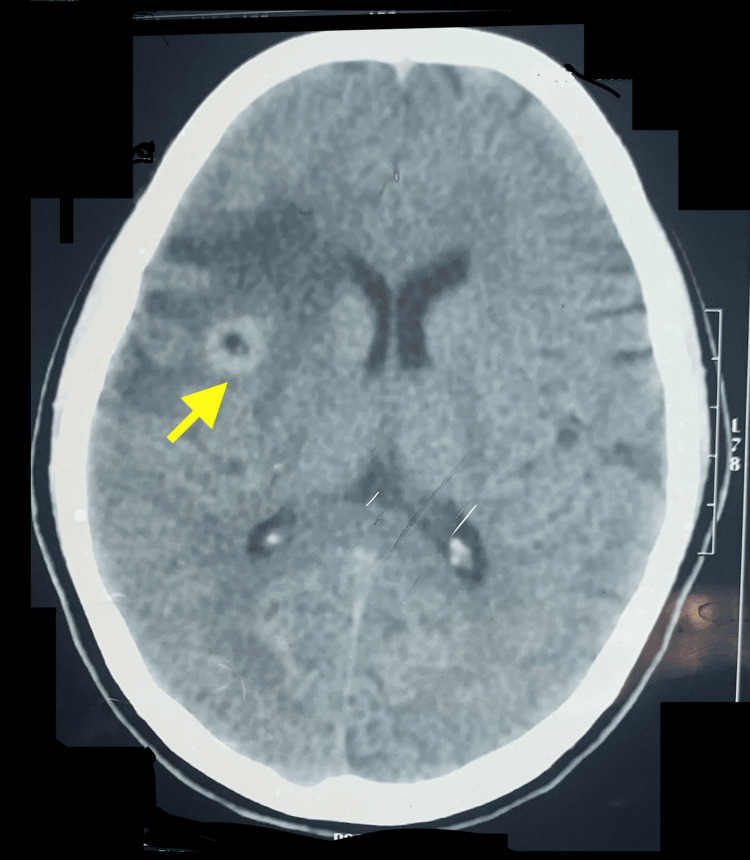 Figure 1
Figure 1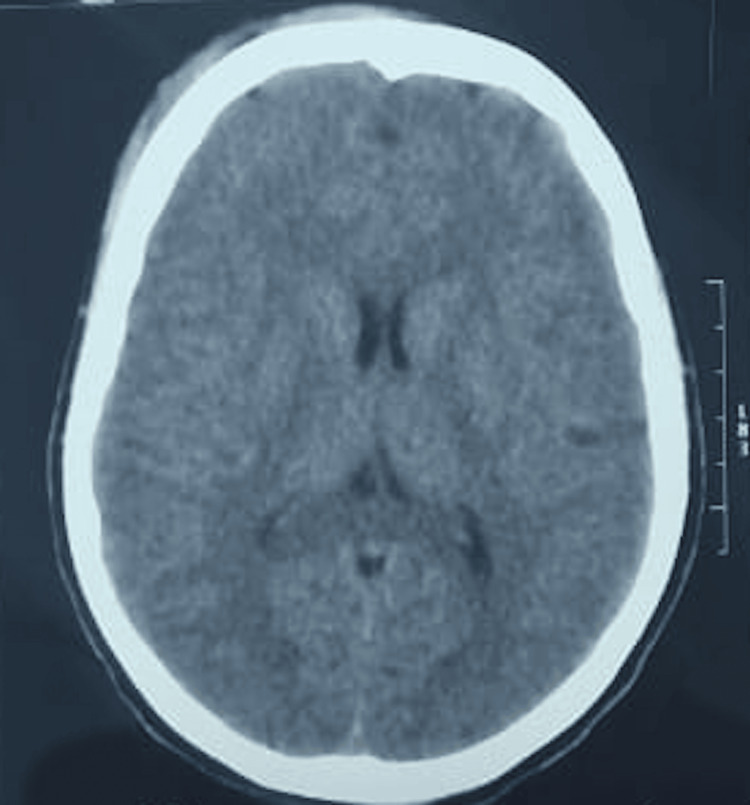 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Congenital Anomalies and Fetal Surgery
Introduction
Cysticercosis is the most common parasitic infection of the brain in tropical and developing countries and can cause epileptic seizures. Taenia solium completes its lifecycle in two hosts: humans (definitive host), and pigs (intermediate host). Humans harbor the adult tapeworm, while pigs carry the larval form (cysticercus cellulosae), which consist of fluid-filled vesicles containing a tapeworm head (scolex) and are typically ingested through contaminated pork by humans. Once ingested, the scolex attaches to the intestinal wall, maturing into a tapeworm. Gravid proglottids and eggs are excreted with feces, facilitating transmission. Humans can sometimes act as intermediate hosts, getting infected with larva or eggs from T. solium. These ova invade the intestinal wall into blood vessels and get established in the brain, eyes, and subcutaneous tissue [1].
In endemic regions, particularly tropical and subtropical areas, T. solium is a significant health concern, accounting for approximately 30% of epilepsy cases and correlating with up to 70% of cases in some studies [2,3]. Although T. solium is not endemic in the United States, cases can occur primarily due to immigration, with a prevalence of 0.2 to 0.6 per 1000 000 people in certain western states [1].
Clinically, T. solium infection can lead to neurological symptoms such as seizures and headaches, which arise when the larvae invade the central nervous system. Peak incidence occurs between 20 and 50 years of age, while reports of infection in toddlers and children with atypical presentations are uncommon [4].
Case presentation
A 12-year-old girl had been suffering from repeated instances of fainting that lasted from a few seconds to a minute with a frequency of three to four times during the past three months. Her parents recently noted a decline in her academic performance. Although the family followed a vegetarian diet, there were pigs living nearby. A clinical examination revealed that her neurological functions were intact. Attention deficits were noted resulting in a score of 8 on the scale used in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Blood tests showed a hemoglobin level of 11.5 gm/dl, a white blood cell count of 108x10^9/L with 70% neutrophils and 10% eosinophils, and an erythrocyte sedimentation rate (ESR) of 30 mm in the first hour. An unenhanced computed tomography (CT) scan of the brain identified a lesion in the right frontal lobe, characterized by a single cyst containing a hyperdense dot (scolex) at its center, along with surrounding edema (Figure 1).
An unenhanced CT scan shows a single parenchymal cyst in the right frontal lobe of the cerebral cortex. Inside the cyst, there was a hyperdense dot with a ' hole-with-dot' sign; extensive edema around the cyst was also noted.
The imaging findings led to a diagnosis of cysticercosis. The patient was prescribed valproic acid at a dosage of 200 mg orally twice daily, along with prednisolone at 5 mg once daily and albendazole at a dose of 15 mg per kg of body weight for 14 days. Following this treatment, the prednisolone dosage was gradually reduced and ultimately discontinued after one week. Valproic acid was continued for three months before being tapered off over the next three months. Patient’s white blood cell count and serum alanine aminotransferase were monitored.
Before the initiation of treatment, the patient suffered from seizures occurring three to four times a day, with each episode lasting around one minute. However, there was a steady decline in the frequency of these seizures, and by the 10th day of treatment, all seizures had completely stopped. After three months of treatment, the cystic lesion was resolved on imaging, and the patient exhibited no signs of attention deficits or seizure activity. A follow-up period of 24 months included regular comprehensive clinical evaluations every three months to monitor for any neurological symptoms. The patient's epileptic seizures, which had decreased during the initial treatment phase, did not reappear throughout the 24-month follow-up. Additionally, a CT scan of the brain conducted at that time showed no residual lesions or calcifications (Figure 2).
A CT scan of brain shows no residual parenchymal lesion.
Discussion
An electroencephalogram (EEG) was not deemed necessary in this case due to the CT finding providing definitive evidence of cysticercosis, which is a known cause of epileptic seizures and other neurological symptoms. Neuroimaging is an established modality for the diagnosis of neurocysticercosis. The definitive identification of a scolex within a cystic lesion on a CT scan, appearing as a hyperdense dot, confirms the absolute diagnostic criteria of cysticercosis. Del Brutto et al. [5] proposed a diagnostic criterion for neurocysticercosis that is widely acknowledged. WHO’s recent guidelines on the management of Taenia solium neurocysticercosis suggests magnetic resonance imaging (MRI) is the tool of choice for the diagnosis of neurocysticercosis; CT scan should be used if MRI is not available or contraindicated; however, CT is the tool of choice for detection of small calcified lesion [6].
The clinical presentation of a single neurocysticercosis can include neurological symptoms. A parenchymal cyst in the brain typically presents with epileptic seizures, often starting as simple partial seizures before progressing to generalized seizures. Cognitive impairments and dementia are also reported manifestations in adults. While the occurrence of attention deficits in children with neurocysticercosis is rarely reported, the presence of a cystic lesion accompanied by significant edema in the frontal lobe can cause this due to dysfunction of the frontostriatal track [7]. The clinical symptoms, such as intermittent short episodes of loss of consciousness and a noticeable decrease in academic performance, highlight the atypical presentation of a frontal lobe cyst, which can be associated with cognitive impairments and seizure activity.
There are differing opinions on the use of antiparasitic medication (albendazole) and steroids in the management of single neurocysticercosis cases. Nevertheless, a dosage of 15 mg/kg of body weight of albendazole for a duration of 10 to 14 days is recommended for patients with a single viable cyst [8]. Albendazole, in combination with corticosteroids, should be given to individuals with symptomatic neurocysticercosis or a single enhancing lesion for better outcomes in terms of cyst resolution and seizure control. Conversely, it should be avoided in calcific cysticercosis [6]. In cases where cerebral edema is present, steroids should be administered at minimal doses for the shortest necessary duration [8].
A close differential diagnosis in developing countries is tuberculoma, especially in the Indian subcontinent, which is hard to distinguish from neurocysticercosis at times. Tuberculomas can be seen in a plain CT scan as hypodense, isodense, or hyperdense lesions with surrounding oedema, while a cystic lesion and a scolex visible inside the cyst are characteristic of cysticercosis [9].
Conclusions
This case study emphasizes the complexities involved in diagnosing frontal lobe cysticercosis in a 12-year-old girl who exhibited atypical symptoms, including attention deficits, in addition to the more common seizures. An unenhanced CT scan revealed a characteristic cyst with a hyperdense scolex, confirming this diagnosis.
Effective treatment with valproic acid, prednisolone, and albendazole led to the resolution of seizures without any residual lesion or calcification on imaging over a 24-month follow-up, reinforcing the importance of a tailored treatment approach. This case emphasizes the need for awareness regarding cysticercosis, particularly in endemic regions or in populations with potential exposures, as cognitive symptoms can be significant and may mimic other neurological disorders.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical symptoms, diagnosis, and treatment of neurocysticercosis Lancet Neurol Garcia HH Nash TE Del Brutto OH 120212151320142545346010.1016/S 1474-4422(14)70094-8PMC 6108081 · doi ↗ · pubmed ↗
- 2Neurocysticercosis. A frequent cause of seizures, epilepsy, and other neurological morbidity in most of the world J Neurol Sci Bustos J Gonzales I Saavedra H Handali S Garcia HH 11752742720213414795710.1016/j.jns.2021.117527 PMC 8800347 · doi ↗ · pubmed ↗
- 3Taeniasis/cysticercosis 3 2025 2022 https://www.who.int/news-room/fact-sheets/detail/taeniasis-cysticercosis
- 4Neurocysticercosis in infants and toddlers: report of seven cases and review of published patients Pediatr Neurol Del Brutto OH 4324354820132366886610.1016/j.pediatrneurol.2013.02.001 · doi ↗ · pubmed ↗
- 5Revised diagnostic criteria for neurocysticercosis J Neurol Sci Del Brutto OH Nash TE White AC Jr 20221037220172801721310.1016/j.jns.2016.11.045 · doi ↗ · pubmed ↗
- 6Guidelines on management of Taenia solium neurocysticercosis 4 2025 2021 http://www.who.int/publications/i/item/978924003223134520139 · pubmed ↗
- 7Frontal neurocysticercosis and attention deficit Colomb Med Barboza M Sepúlveda S Montalvo D 2127382007
- 8Management of neurocysticercosis in children: Association of Child Neurology consensus guidelines Indian Pediatr Sankhyan N Kadwa RA Kamate M 87188058202134338221 · pubmed ↗