Technical tips for EUS for pancreatic lesions in patients undergoing total gastrectomy and Roux-en-Y reconstruction (with videos)
Tatsuya Koshitani, Kumpei Kadosaka, Hiroshi Takihara, Takahiro Takemoto

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
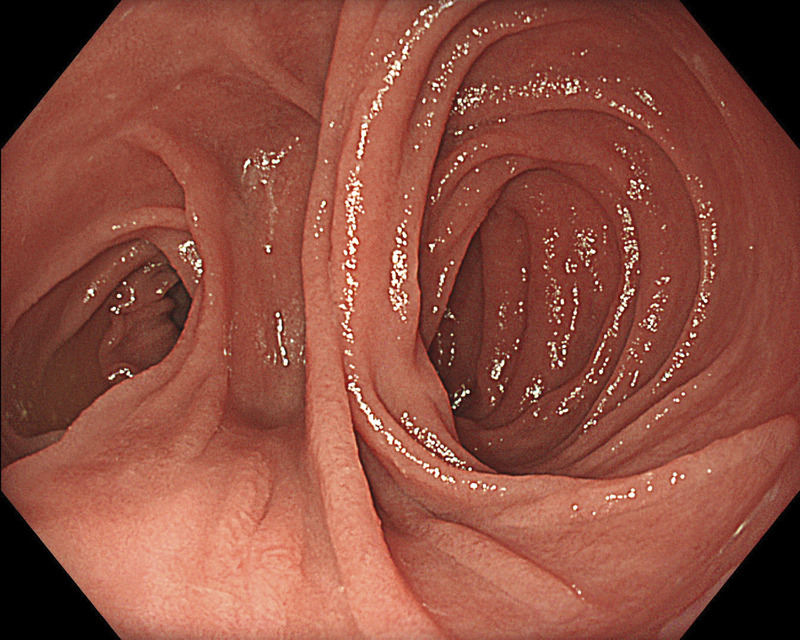 Figure 1
Figure 1 Figure 2
Figure 2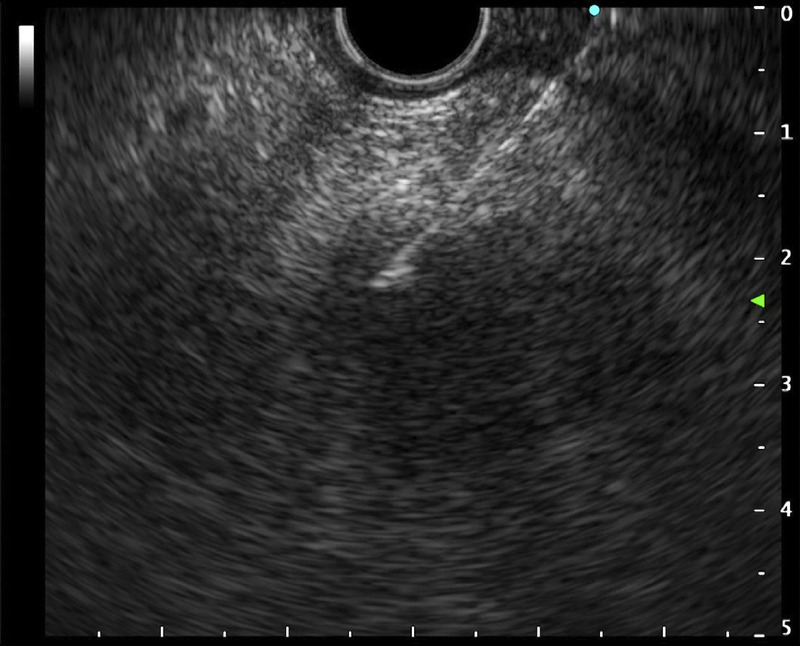 Figure 3
Figure 3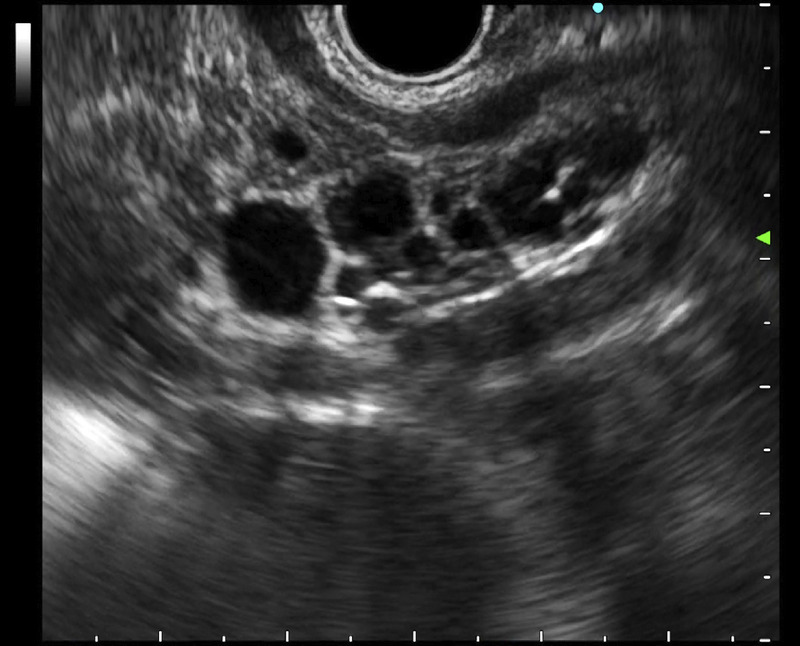 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal and GI Pathology · Gastrointestinal Tumor Research and Treatment
EUS for pancreatic lesions in patients with altered gastrointestinal anatomy has technical challenges.^[1–3]^ This study aims to provide technical tips for EUS for pancreatic lesions in patients who underwent total gastrectomy and Roux-en-Y reconstruction. EUS and fluoroscopic imaging were presented during pancreatic observation in such patients, and EUS-guided fine-needle aspiration (EUS-FNA) was performed. A convex echoendoscope (GF-UCT-260; Olympus) and EUS video processors (EU-ME2 and ME3; Olympus) were used.
First, the echoendoscope was positioned proximal to the efferent jejunal loop. Pancreatic visualization from the body to the tail was achieved using a clockwise rotation, similar to normal anatomical conditions, whereas an anticlockwise rotation was used for visualization from the tail to the body. Next, the echoendoscope was advanced slightly deeper into the efferent loop to observe the pancreatic head. Visualization of the pancreatic head required adjusting the position of echoendoscope while rotating the endoscope. Pancreatic observation from the head to the tail was then feasible using a clockwise rotation while gradually withdrawing the echoendoscope. Fluoroscopic imaging confirmed that the echoendoscope was positioned at a deeper site in the efferent loop, and the tip of the scope was angulated [Figure 1 and Video 1].
Supplementary Videos
Video 1: EUS and fluoroscopic imaging during pancreatic observation after total gastrectomy and Roux-en-Y reconstruction;
Herein, we present 3 cases: cases 1 and 2 involved heterogeneous hypoechoic lesions with irregular margins in the pancreatic tail and head, respectively. EUS-FNA was performed, and pathological examination revealed adenocarcinoma in each case. In case 3, EUS was performed to investigate a dilated common bile duct. Incidentally, a multilocular cystic lesion was found in the pancreatic head and was diagnosed as a branch-duct intraductal papillary mucinous neoplasm [Figures 2, 3, 4, and Video 2].
EUS for pancreatic lesions in patients who had underwent total gastrectomy and Roux-en-Y reconstruction remains challenging, particularly for pancreatic head lesions. However, such examination could be facilitated by initiating EUS at a slightly deeper site in the efferent loop. This technique appears applicable to most patients with Roux-en-Y reconstruction. Nevertheless, careful echoendoscope handling is essential to minimize the risk of injury to the efferent loop. Once a pancreatic lesion is identified, conventional techniques for EUS-FNA can be applied.
Ethical Approval
The study was conducted according to the guidelines of the Declaration of Helsinki.
Informed Consent
Informed consent was obtained from all the patients for the study.
Conflicts of Interest
The authors indicated no potential conflicts of interest.
Author Contributions
T.K. designed and directed the study and wrote the manuscript. K.K. assisted with the procedure. All authors critically revised the manuscript and approved the final manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wilson JA Hoffman B Hawes RH, . EUS in patients with surgically altered upper GI anatomy. Gastrointest Endosc 2010;72:947–953.21034896 10.1016/j.gie.2010.07.016 · doi ↗ · pubmed ↗
- 2Brozzi L Petrone MC Poley JW, . Outcomes of biliopancreatic EUS in patients with surgically altered upper gastrointestinal anatomy: A multicenter study. Endosc Int Open 2020;8:E 869–E 876.32617391 10.1055/a-1161-8713 PMC 7297615 · doi ↗ · pubmed ↗
- 3Tanaka K Hayashi T Utsunomiya R, . Endoscopic ultrasound-guided fine needle aspiration for diagnosing pancreatic mass in patients with surgically altered upper gastrointestinal anatomy. Dig Endosc 2020;32:967–973.31912558 10.1111/den.13625 · doi ↗ · pubmed ↗