Comparative Analysis of Hiatal Hernia Repair Techniques: A Meta-Analysis Review Study on Biological Mesh, Phasix™ Mesh, and Primary Repair
Samer Ganam, Chandler N Lentovich, Ryan Tang, Rahul Mhaskar, Joseph A Sujka, Christopher G DuCoin, Emily Coughlin

TL;DR
This study compares different hiatal hernia repair techniques and finds that Phasix™ ST mesh has the lowest recurrence and complication rates.
Contribution
The study provides a meta-analysis comparing Phasix™ ST mesh, biological mesh, and primary repair for hiatal hernia repair.
Findings
Phasix™ ST mesh had the lowest recurrence rate compared to biological mesh and primary repair.
No reoperations were reported with Phasix™ ST mesh.
Postoperative dysphagia was lowest with Phasix™ ST mesh.
Abstract
Mesh usage in hiatal hernia repair is debated regarding recurrence rates and complications. This study aims to compare the efficacy of Phasix™ ST mesh, biological mesh, and primary repair in terms of recurrence rates, reoperation rates, and mesh-related complications. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed to search literature in PubMed, Embase, and Web of Science from January 2011 to November 2023. Included studies focused on participants aged 18+ undergoing hiatal hernia repair with specific mesh types or repair methods. Data on recurrence rates, reoperation rates, and mesh-related complications were analyzed by BMI and follow-up time subgroups. Statistical analysis used the Mantel-Haenszel random-effects model. Bias in studies was assessed using the ROBINS-I and Cochrane risk of bias tools for non-randomized and randomized…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
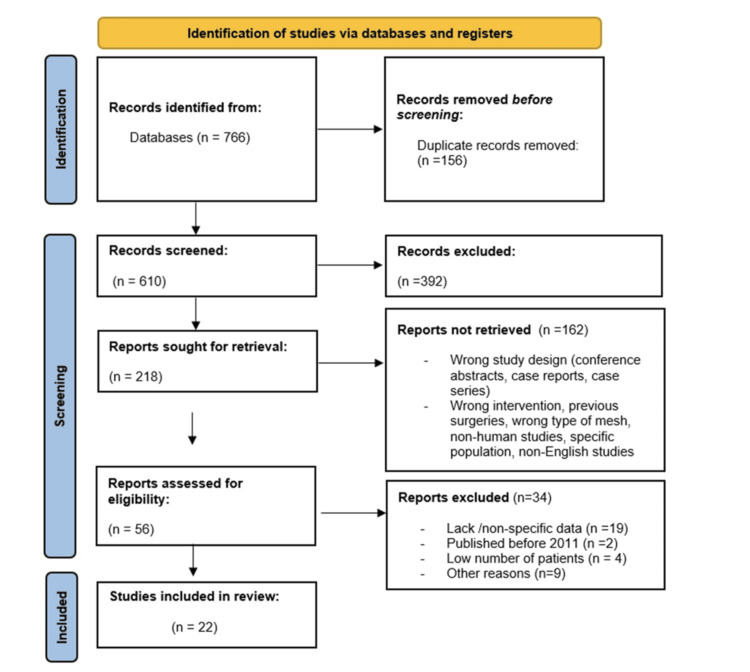 Figure 1
Figure 1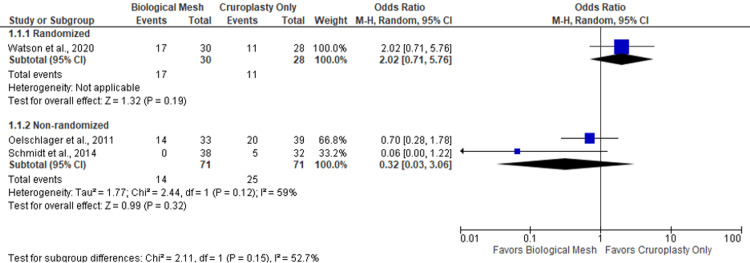 Figure 2
Figure 2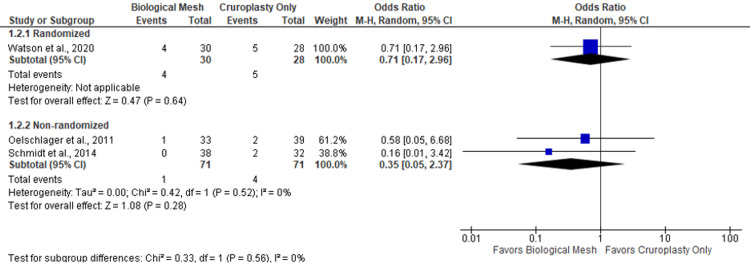 Figure 3
Figure 3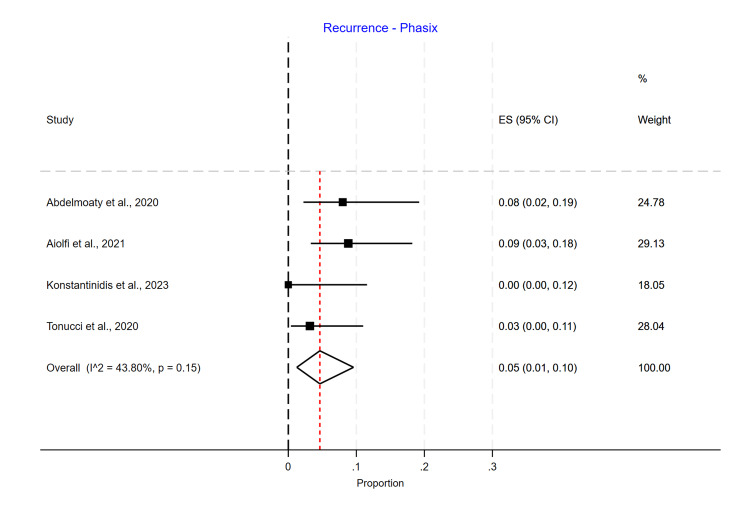 Figure 4
Figure 4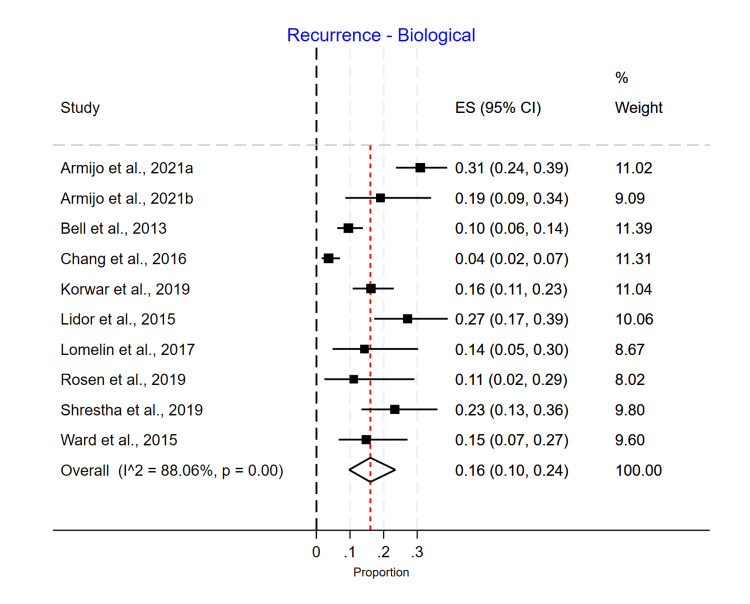 Figure 5
Figure 5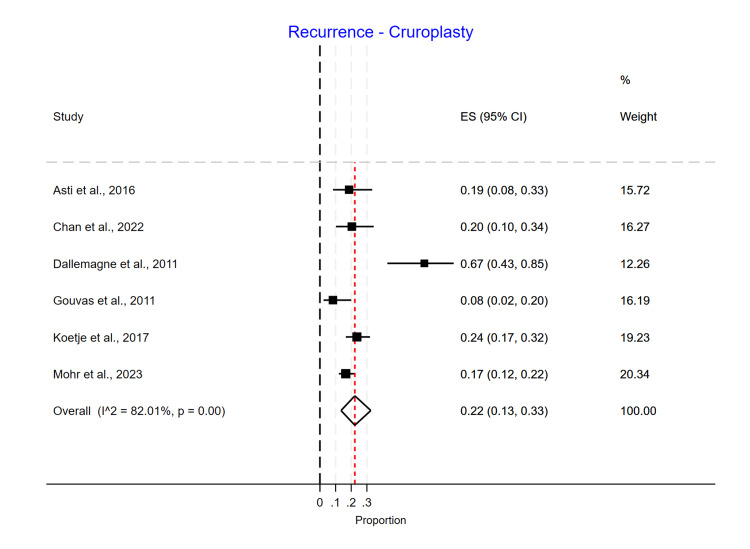 Figure 6
Figure 6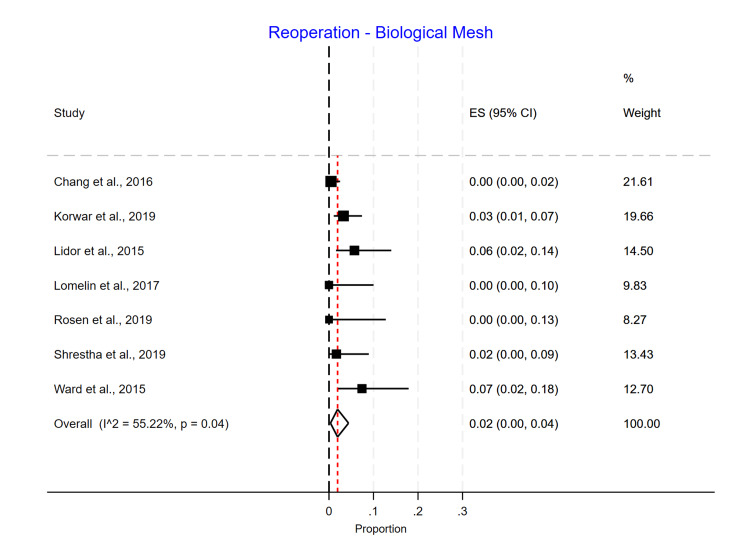 Figure 7
Figure 7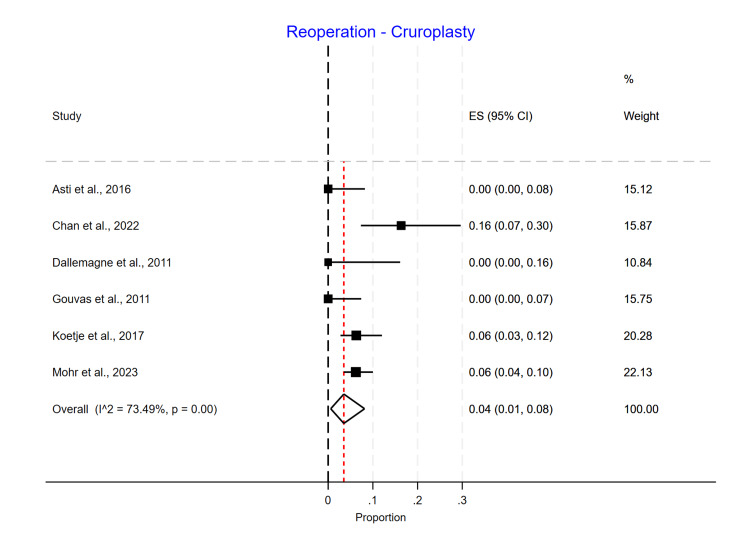 Figure 8
Figure 8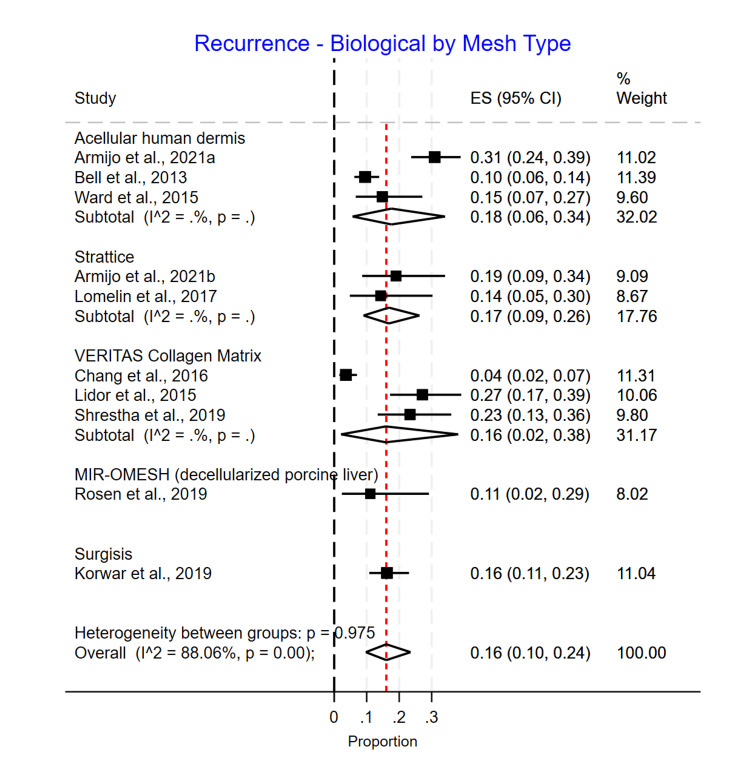 Figure 9
Figure 9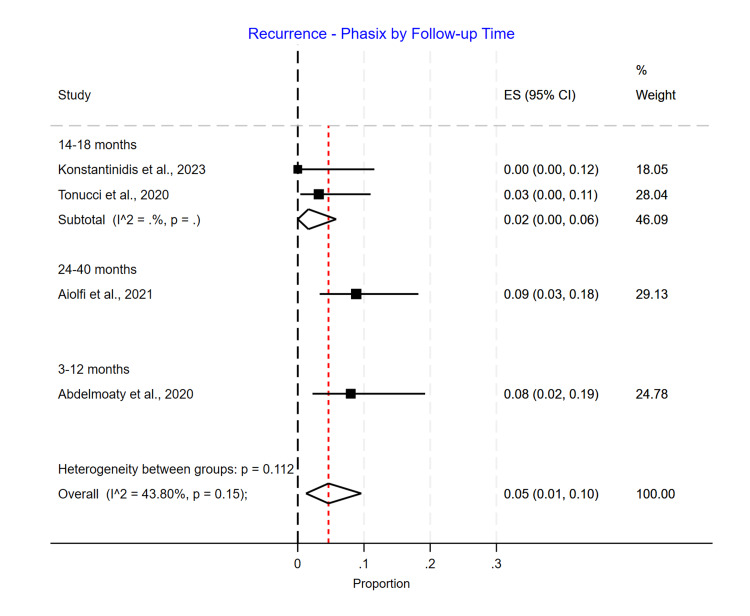 Figure 10
Figure 10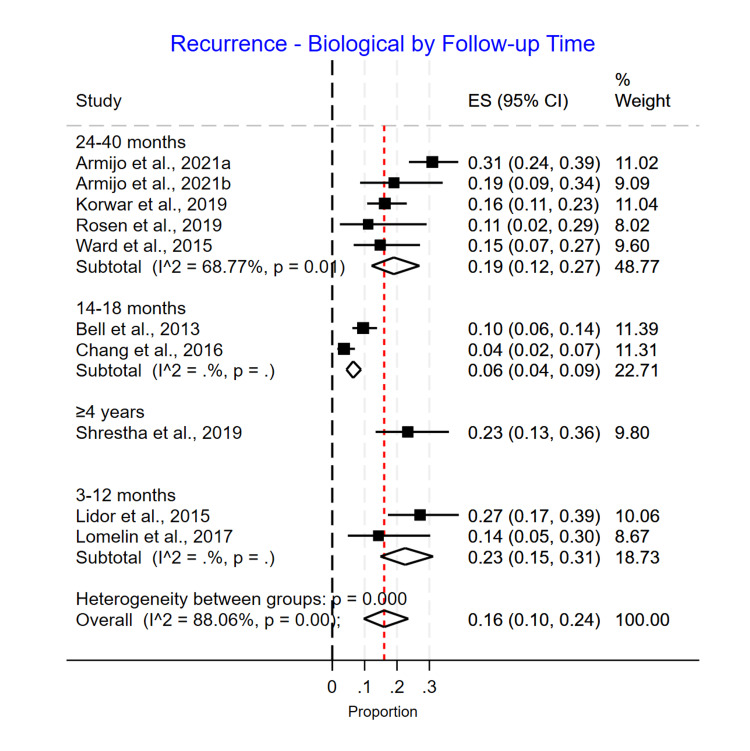 Figure 11
Figure 11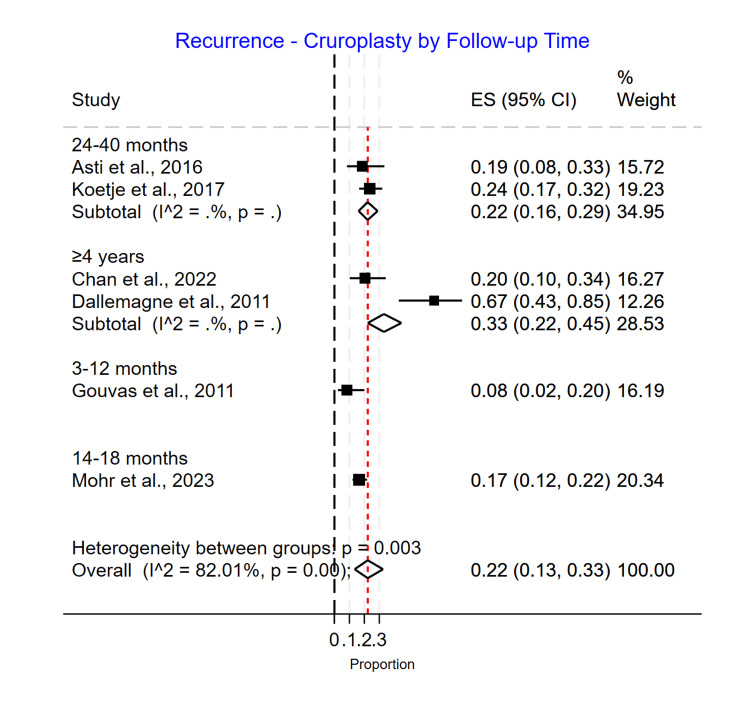 Figure 12
Figure 12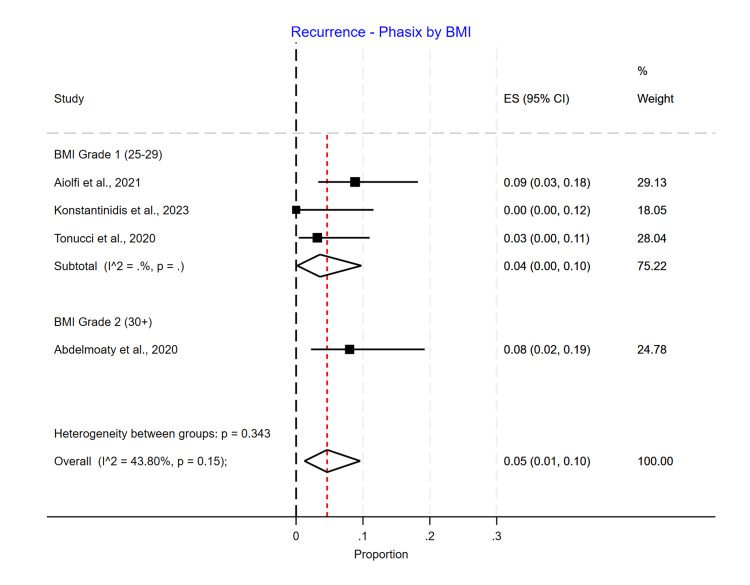 Figure 13
Figure 13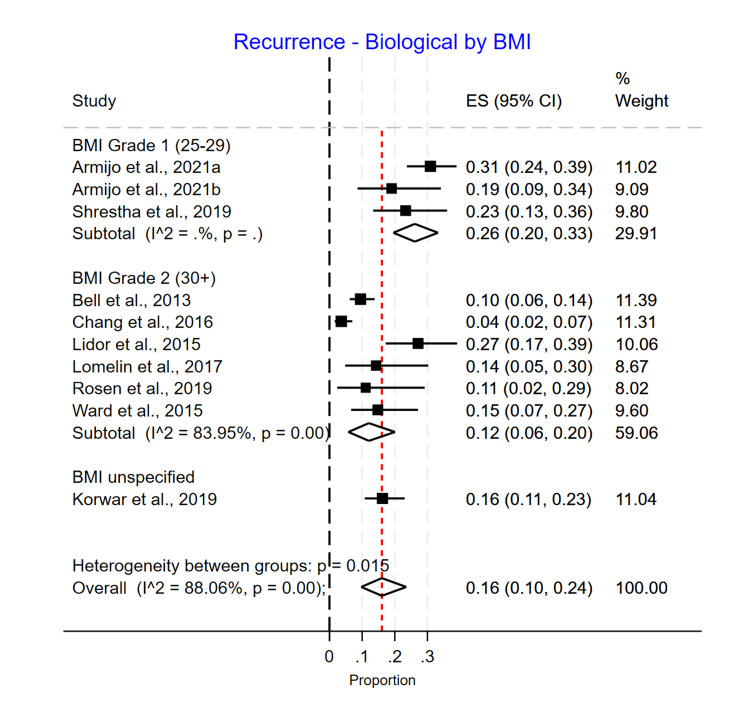 Figure 14
Figure 14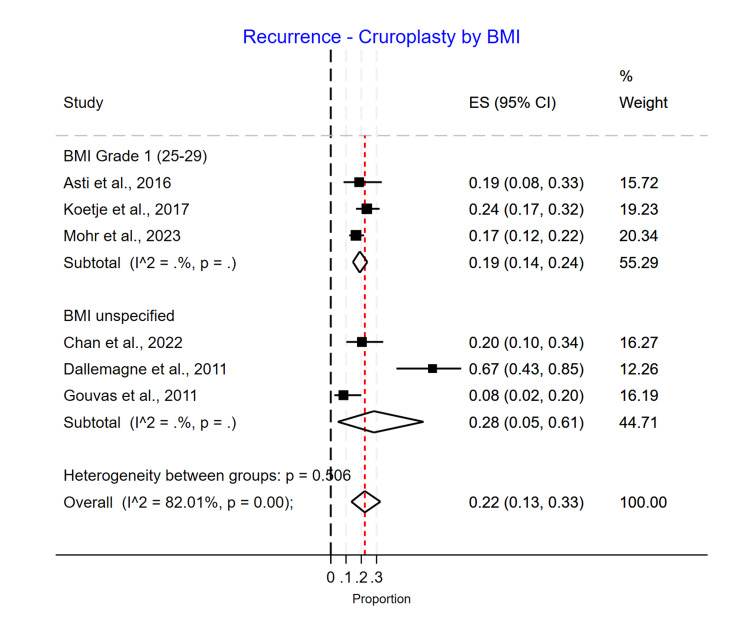 Figure 15
Figure 15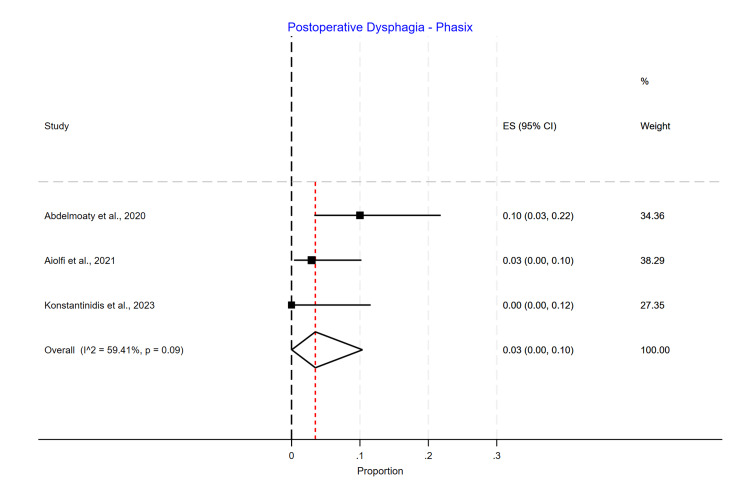 Figure 16
Figure 16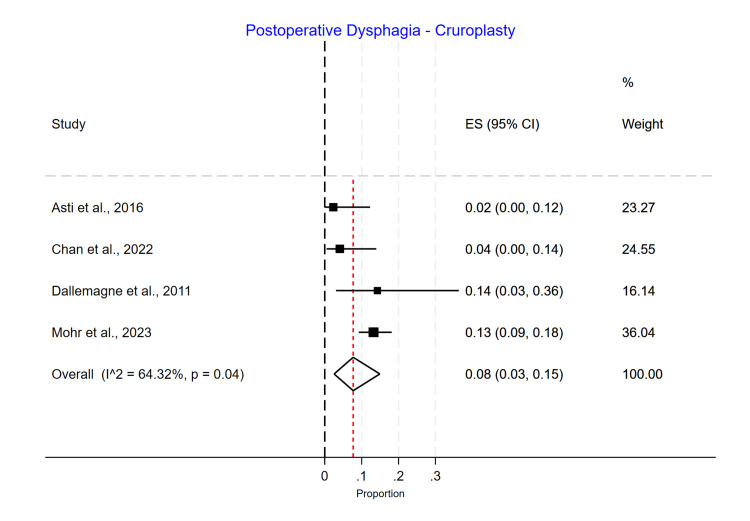 Figure 17
Figure 17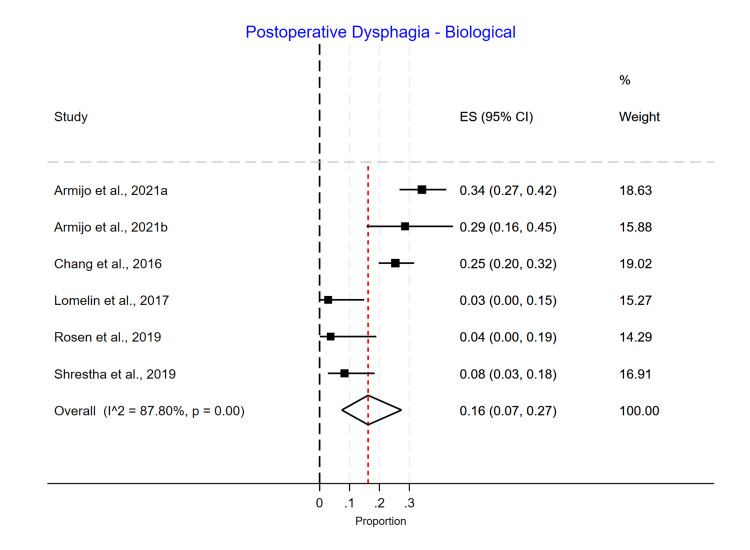 Figure 18
Figure 18| Authors | Year | Mesh subtype | N | Age | BMI | Median follow-up | Recurrence | Reoperation | Postoperative dysphagia N (%) | |
| Cruroplasty data | Watson et al. [ | 2020 | NA | 28 | Mean age: 67.8 (range: 64.7-70.9) | Mean BMI: 29.6 (range: 28.0-31.2) | 3-4 years | 39.29% | 17.86% | 5 (17.86%) |
| Biological mesh data | Watson et al. [ | 2020 | Surgisis mesh | 30 | Mean age: 68.0 (range: 65.1-70.9) | BMI 29.4 (range: 27.8-31.0) | 3-4 years | 56.67% | 13.33% | 3 (10%) |
| Repair type | Authors | Year | Mesh subtype | N | Age | BMI | Median follow-up | Recurrence | Reoperation | Postoperative dysphagia N (%) |
| Cruroplasty | Oelschlager et al. [ | 2011 | NA | 39 | Mean age: 63 (SD: 10) | Mean BMI: 31.3 (SD: 4.9) | 58 months | 51.28% | 5.13% | 0 (0%) |
| Cruroplasty | Schmidt et al. [ | 2014 | NA | 32 | Mean age: 41 (SD: NA) | Mean BMI: 29.5 (SD: NA) | 12 months | 15.63% | 6.25% | 1 (3.13%) |
| Biological mesh | Oelschlager et al. [ | 2011 | SIS mesh | 33 | Mean age: 64 (SD: 10) | Mean BMI: 30.2 (SD: 5.6) | 58 months | 42.42% | 3.03% | 0 (0%) |
| Biological mesh | Schmidt et al. [ | 2014 | Human acellular dermal matrix | 38 | Mean age: 51 (SD: NA) | Mean BMI 31.37 (SD: NA) | 12 months | 0% | 0% | 2 (5.26%) |
| Authors | Year | N | Age | BMI | Median follow-up | Recurrence | Reoperation | Postoperative dysphagia N (%) |
| Abdelmoaty et al. [ | 2020 | 50 | Median age: 67 (range: 44-84) | Mean BMI: 30.6 (range: 20-41.5) | 12 months | 8% | 0% | 5 (10%) |
| Aiolfi et al. [ | 2022 | 68 | Mean age: 66.3 (SD: 12.7) | Mean BMI: 26.3 (SD: 5.1) | 27 months | 8.82% | 0% | 2 (2.94%) |
| Konstantinidis and Charisis [ | 2023 | 30 | Median age: 56 (range: 27-81) | Median BMI: 27.5 (range: 21-38.5) | 14 months | 0% | 0% | 0 (0%) |
| Panici Tonucci et al. [ | 2020 | 63 | Mean age: 68.2 (SD: 23.2) | Mean BMI: 26.9 (SD: 3.5) | 17 months | 3.17% | 0% | NA |
| Authors | Year | Mesh subtype | N | Age | BMI | Median follow-up | Recurrence | Reoperation | Postoperative dysphagia N (%) |
| Armijo et al. [ | 2021 | AlloDerm human tissue matrix | 152 | Median age: 60 (range: 49-69) | Median BMI: 29.44 (range: 26.82-32.30) | 27 months | 44.08% | NA | 52 (85.25%) |
| Armijo et al. [ | 2021 | Strattice porcine tissue matrix | 42 | Median age: 62 (range: 58-74) | Median BMI: 29.74 (range: 25.86-34.43) | 27 months | 40.48% | NA | 12 (80%) |
| Bell et al. [ | 2013 | AlloGraft dermal matrix | 252 | Mean age: 57 (SD: 13.4) | Mean BMI: 30.0 (SD: 5.7) | 18 months | 9.5% | NA | NA |
| Chang and Thackeray [ | 2016 | Veritas Collagen Matrix | 221 | Mean age: 51.1 (SD: 12.7) | Mean BMI: 36.1 (SD: 7.1) | 14.5 months | 3.62% | 0.45% | 56 (25.34%) |
| Korwar et al. [ | 2019 | Surgisis mesh | 154 | Mean age: 65 (SD: 12) | NA | 35 months | 16.23% | 3.25% | NA |
| Lidor et al. [ | 2015 | Veritas Collagen Matrix | 70 | Mean age: 61.5 (SD: 13.5) | Mean BMI: 30.06 (SD: 6.74) | 12 months | 27.14% | 5.71% | NA |
| Lomelin et al. [ | 2017 | Strattice biologic mesh | 35 | Mean age: 63.1 (SD: 12.0) | Mean BMI: 30.8 (SD: 6.3) | 12 months | 14.29% | 0% | 1 (2.86%) |
| Rosen et al. [ | 2019 | MIROMESH derived from decellularized porcine liver | 27 | Mean age: 63.3 (range: 26-79) | BMI: 30.7 (range: 22-39) | 24 months | 11.11% | 0% | 1 (3.7%) |
| Shrestha et al. [ | 2019 | Veritas Collagen Matrix | 60 | Median age: 71 (range: 42-89) | Median BMI: 29 (range: 19-42) | 60 months | 23.33% | 1.67% | 5 (8.33%) |
| Ward et al. [ | 2015 | Acellular human dermis | 54 | Mean age: 60.8±10.5 for the FlexHD group and 64.3±10.1 for the AlloDerm group | Mean BMI: 31.3±4.66 for the FlexHD group and 32.6±6.55 for the AlloDerm group | 33 months | 14.8% | 7.41% | NA |
| Authors | Year | N | Age | BMI | Median follow-up | Recurrence | Reoperation | Postoperative dysphagia N (%) |
| Asti et al. [ | 2016 | 43 | Mean age: 65.8 (SD: 13.6) | Mean BMI: 26.5 (SD: 3.3) | 24 months | 18.6% | 0% | 1 (2.33%) |
| Dallemagne et al. [ | 2011 | 21 | Median age of 66 (range: 37-85 years) | NA | 151 months | 66.67% | 0% | 3 (14.29%) |
| Chan et al. [ | 2022 | 49 | Mean age: 57.3 (SD: 10.7) | NA | 77.1 months | 20.41% | 16.33% | 2 (4.08%) |
| Gouvas et al. [ | 2011 | 48 | Median age: 65 (range: 38-84 years) | NA | 12 months | 8.33% | 0% | NA |
| Koetje et al. [ | 2017 | 127 | Mean age: 66.9 (SD: 10.3) | Mean BMI: 28.7 (SD: 4.2) | 39.3 months | 23.62% | 6.3% | NA |
| Mohr et al. [ | 2023 | 242 | Mean age: 51.1 (SD: 13.0) | Mean BMI: 29.7 (SD: 5.6) | 17 months | 16.53% | 6.2% | 32 (13.22%) |
| Author | Selection bias: random sequence generation | Selection bias: allocation concealment | Reporting bias: selective reporting | Other sources of bias | Performance bias: blinding (participants and personnel) | Detection bias: blinding (outcome assessment) | Attrition bias: incomplete outcome data |
| Watson et al. [ | Unclear: method of random sequence generation not stated | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Author | Bias due to confounding | Bias in the selection of participants | Bias in the classification of interventions | Bias due to deviations from intended interventions | Bias due to missing data | Bias in the measurement of outcomes | Bias in the selection of the reported result | Overall |
| Abdelmoaty et al. [ | Low risk | Low risk | Low risk | Unclear: not stated if any procedures were converted to open | Low risk | Low risk | Low risk | Fair |
| Aiolfi et al. [ | Low risk | Low risk | Low risk | Unclear: not stated if any procedures were converted to open | Low risk | Low risk | Low risk | Fair |
| Konstantinidis and Charisis [ | High risk: comorbidities that increase the intra-abdominal pressure are part of the inclusion criteria but are not elucidated in the paper | Low risk | Low risk | Low risk | High risk: different hernia sizes were recorded, but recurrence rates were compared as one group | Low risk | Low risk | Poor |
| Panici Tonucci et al. [ | Low risk | Low risk | Low risk | Low risk | Low risk | Unclear: upper gastrointestinal endoscopy and/or barium/Gastrografin swallow study used for the determination of recurrent hiatal hernia | Low risk | Fair |
| Armijo et al. [ | Low risk | Low risk | Low risk | Unclear: not stated if any procedures were converted to open | High risk: retention of only 59.2% of patients at the long-term follow-up | Low risk | Low risk | Poor |
| Bell et al. [ | Low risk | Low risk | Low risk | Unclear: not stated if any procedures were converted to open | Low risk | Unclear: recurrence was only evaluated anatomically if patients presented with symptoms, "objective testing" to determine anatomy was stated, but specific methods were not described | Low risk | Fair |
| Chang and Thackeray [ | Low risk | Low risk | Low risk | Unclear: not stated if any procedures were converted to open | Low risk | Low risk | Low risk | Fair |
| Korwar et al. [ | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Good |
| Lidor et al. [ | Low risk | Low risk | Low risk | Unclear: not stated if any procedures were converted to open | Low risk | Low risk | Low risk | Fair |
| Lomelin et al. [ | Low risk | Low risk | Low risk | Low risk | Low risk | Unclear: patients had barium swallow and/or EGD at 12 months postoperatively to assess for recurrence | Low risk | Fair |
| Oelschlager et al. [ | Low risk | Low risk | Low risk | Unclear: not stated if any procedures were converted to open | Low risk | Low risk | Low risk | Fair |
| Rosen et al. [ | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Good |
| Schmidt et al. [ | High risk: statistically significant age difference between groups | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Fair |
| Shrestha et al. [ | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Good |
| Ward et al. [ | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Good |
| Asti et al. [ | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Good |
| Dallemagne et al. [ | Low risk | Low risk | Low risk | Low risk | High risk: GIQLI did not exist when the study began, and no preoperative values were collected as a result | Low risk | Low risk | Fair |
| Chan et al. [ | Low risk | Low risk | Low risk | Unclear: not stated if any procedures were converted to open | Low risk | Low risk | Low risk | Fair |
| Gouvas et al. [ | Low risk | Low risk | Low risk | Low risk | High risk: different hernia sizes were recorded, but recurrence rates were compared as one group | Low risk | Low risk | Fair |
| Koetje et al. [ | High risk: a statistically significant difference in the American Society of Anesthesiologists Physical Status scores between groups | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Fair |
| Mohr et al. [ | High risk: statistically significant age difference between groups | Low risk | Low risk | Low risk | Low risk | Unclear: the method of assessing radiographic recurrence is not stated, and patients were not evaluated for radiographic recurrence if asymptomatic | Low risk | Poor |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Dysphagia Assessment and Management · Esophageal and GI Pathology
Introduction and background
A hiatal hernia is characterized by the displacement of the upper stomach and possibly an additional organ, such as the colon, small intestine, or spleen, into the thoracic cavity via a widening of an esophageal hiatus within the diaphragm [1].
Hiatal hernias may be congenital or acquired, and loss of muscle strength and elasticity with increased age may be a risk factor. Other risk factors include conditions that increase intra-abdominal pressure, such as obesity, pregnancy, chronic constipation, and chronic obstructive pulmonary disease (COPD). Hiatal hernias typically present with similar symptoms to gastroesophageal reflux disease (GERD), such as heartburn, regurgitation, and chronic cough. To diagnose whether a patient has a hiatal hernia, endoscopy, manometry, pH monitoring, and/or esophagography should be performed.
Recommendations regarding when to perform a hiatal hernia repair depend on both the presence of symptoms and hernia size. Any patient experiencing symptoms secondary to the hiatal hernia, such as heartburn, regurgitation, or difficulty swallowing, is recommended to undergo hiatal hernia repair. In addition, patients who are asymptomatic with a large hiatal hernia, such as one in which over half of the stomach protrudes through the hiatus, are also recommended to undergo hiatal hernia repair if they are under the age of 60 with no severe comorbidities. Even after repair, hiatal hernias tend to have a high recurrence rate. Surgeons have tried to reduce the recurrence rate of hiatal hernias by reinforcing suture repair with prosthetic mesh. Still, erosion and shrinkage of the mesh have led the surgical community to explore other ways to strengthen the surgical repair [2,3]. Bioabsorbable mesh has been suggested as an adjunct to surgical repair, and studies have suggested that it is safe and has a low complication rate [4].
One bioabsorbable mesh of interest is Phasix™ ST mesh. Other institutions have reported that Phasix™ ST mesh is not associated with mesh-related complications and is more effective in reducing hiatal hernia recurrence in both short- and medium-term follow-ups when compared to simple suture cruroplasty [5-9]. However, there is limited literature that directly compares the use of Phasix™ ST mesh to biological mesh, and typically, if there is an attempt at comparing the two, it is inconclusive due to limited data [9]. Therefore, in this paper, we will compare patient outcomes, including recurrence rate and mesh type-related complications, between those who have undergone hiatal hernia repair using biological mesh and those who have undergone hiatal hernia repair using Phasix™ ST bioabsorbable mesh and both with primary repair (suture cruroplasty).
Therefore, the objective of this study is to determine whether there is a significant difference in hiatal hernia recurrence rate and reoperation between suture cruroplasty, biological mesh, or Phasix™ ST mesh usage in hiatal hernia repair.
Review
Methods
The nature of our meta-analysis study exempted us from requiring Institutional Review Board (IRB) approval. A literature search was performed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. PubMed, Embase, and Web of Science were queried for records between January 2011 and November 2023 using relevant search terms. Exclusion criteria included case reports, case series, conference abstracts, non-human studies, specific populations (neonatal patients), non-English records, and studies where patients had secondary or concomitant surgery. Inclusion criteria were studies with participants 18 or older who underwent primary hiatal hernia repair using Phasix™ ST mesh, biological mesh, or primary repair.
Data Extraction
The following data were extracted from each study: study design type, follow-up time, number of patients, mean age, mesh type, hernia size, recurrence events/rates, reoperation events/rates, mean BMI, complications, GERD, and dysphagia. BMI was divided into two groups: the "Grade 1" group consisted of patients with a BMI of 25-29, and the "Grade 2" group consisted of patients with a BMI of 30+. Groups were assessed in terms of the following follow-up times: 3-12 months, 14-18 months, 24-40 months, and greater than four years. Hernia size was not included in the statistical analysis due to variability in reporting. To assess the risk of bias, we used the Cochrane risk of bias tool for randomized controlled trials and the ROBINS-I risk of bias tool for non-randomized trials.
Statistical Methods
Meta-analysis of studies comparing biological mesh and cruroplasty was conducted using RevMan Version 5.4 (The Cochrane Collaboration, London, England, United Kingdom). The Mantel-Haenszel random-effects model reported odds ratios (OR) and 95% confidence intervals (95% CI). Single-arm studies were pooled using a random-effects model reporting pooled proportions and 95% CI. Single-arm analysis was conducted using Stata Statistical Software: Release 17.0 (April 2021; StataCorp LLC, College Station, Texas, United States). All analyses were assessed for heterogeneity using the I2 statistic.
Results
Our initial search yielded 766 records, and 22 studies were deemed eligible for inclusion (Figure 1). Overall, a total of 2,008 patients who received different types of mesh (211 Phasix™ ST mesh, 1,168 biological mesh, and 629 cruroplasty) were assessed (Tables 1-5).
PRISMA diagramPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
A double-arm meta-analysis was done with three studies [3,10,11] comparing biological mesh (N=101) and cruroplasty (N=99). One trial was randomized and showed no evidence of a significant difference in recurrence in patients with biological mesh vs. cruroplasty (OR 2.02; 95% CI 0.71-5.76). Two studies were non-randomized, and they showed no evidence of a significant difference in recurrence among biological mesh vs. cruroplasty (OR 0.32; 95% CI 0.03-3.06). This analysis did not show significant heterogeneity (I2=59%; p=0.12) (Figure 2) (Tables 1-2).
Double-arm meta-analysis, recurrence rate
Additionally, the randomized and non-randomized trials comparing biological mesh vs. cruroplasty showed no evidence of a significant difference in reoperations (OR 0.71; 95% CI 0.17-2.96 and OR 0.35; 95% CI 0.05-2.37, respectively). This analysis did not show significant heterogeneity (I2=0%; p=0.52) (Figure 3).
Double-arm meta-analysis, reoperation rate
Single-arm meta-analyses were conducted for each mesh type, showing that Phasix™ ST mesh [5-7,12] had the lowest recurrence rate of 0.05 (95% CI 0.01-0.10) (Figure 4), followed by biological mesh [2,13-20] 0.16 (95% CI 0.10-0.24) (Figure 5) and suture cruroplasty [21-26] 0.22 (95% CI 0.13-0.33) (Figure 6). No reoperations were reported with Phasix™ ST mesh. The biological mesh had a reoperation rate of 0.02 (95% CI 0.00-0.04) (Figure 7), and cruroplasty had a reoperation rate of 0.04 (95% CI 0.01-0.08) (Figure 8). The Phasix™ mesh was used in four studies, and the pooled analysis did not show significant heterogeneity (I2=44%; p=0.15). However, considerable heterogeneity was found among biological mesh studies reporting recurrence (I2=88%; p<0.001) and cruroplasty studies reporting recurrence (I2=82%; p<0.001). For studies reporting reoperation, heterogeneity was significant for biological mesh (I2=55%; p=0.04) and cruroplasty pooled analyses (I2=73%; p<0.001).
Recurrence rate of Phasix™ mesh studies
Recurrence rate of biological mesh studies
Recurrence rate of suture cruroplasty studies
Reoperation rate of the biological mesh group
Reoperation rate of the cruroplasty group
Biological Mesh Type Subgroup Analysis
For the biological mesh subgroup analysis, we observed that MIROMESH [18] (decellularized porcine liver) had the lowest recurrence rate of 0.11 (95% CI 0.02-0.29), followed by Surgisis [3] and Veritas Collagen Matrix [14,16,19] with a recurrence rate of 0.16 (95% CI 0.11-0.23) and 0.16 (95% CI 0.02-0.38), respectively. This is followed by Strattice mesh [2,17] (0.17; 95% CI 0.09-0.26) and acellular human dermis [2,11,13,20] (0.18; 95% CI 0.06-0.34) (Figure 9).
Biological mesh subgroup recurrence rate
The reoperation rate for the biological subgroup was as follows: Strattice and MIROMESH (decellularized porcine liver) had similar rates of reoperation 0.00 (95% CI 0.00-0.10) and 0.00 (95% CI 0.00-0.13), respectively, followed by Veritas Collagen Matrix with 0.02 (95% CI 0.00-0.06), Surgisis with 0.03 (95% CI 0.01-0.07), and acellular human dermis with 0.07 (95% CI 0.02-0.18) (Figure 7).
Length of Follow-Up Subgroup Analysis
As regards subgroup analysis based on the duration of the follow-up for the outcome of recurrence, Phasix™ ST mesh showed no statistically significantly different rates with 0.08 (95% CI 0.02-0.19) for the 3-12-month follow-up, 0.02 (95% CI 0.00-0.06) for the 14-18-month follow-up, and 0.09 (95% CI 0.03-0.18) for the 24-40-month follow-up (p=0.15) (Figure 10).
Recurrence rate for Phasix™ mesh based on length of follow-up
For the biological mesh group, the recurrence rates for patients were noticed to be significantly different based on the duration of follow-up with 0.23 (0.15-0.31) for 3-12 months, 0.06 (0.04-0.09) for 14-18 months, 0.19 (0.12-0.27) for 24-40 months, and 0.23 (0.13-0.36) for more than four years of follow-up (p>0.001) (Figure 11). For the suture cruroplasty group, the recurrence rates increased with longer follow-up, with 0.08 (0.02-0.20) for 3-12 months, 0.17 (0.12-0.22) for 14-18 months, 0.22 (0.16-0.29) for 24-40 months, and 0.33 (0.22-0.45) for more than four years of follow-up (p=0.00) (Figure 12).
Recurrence rate for biological mesh based on length of follow-up
Recurrence rate for cruroplasty based on length of follow-up
BMI Subgroup Analysis
In a subgroup analysis by average BMI, the recurrence rate did not significantly differ (p=0.15). However, recurrence appeared to be higher in the Grade 2 BMI group in the Phasix™ ST mesh group, with 0.08 (0.02-0.19) recurrence compared to 0.04 (0.00-0.10) in the Grade 1 BMI group. However, only one study had patients with an average BMI greater than 30 (Grade 2) (Figure 13). For the biological mesh group, the recurrence rate was higher in the Grade 1 BMI group, with 0.26 (0.20-0.33) recurrence compared to 0.12 (0.06-0.20) in the Grade 2 BMI group and 0.16 (0.11-0.23) in the unspecified BMI group (Figure 14). For the suture cruroplasty group, 50% of studies did not report BMI, and the recurrence rate was higher for the unspecified BMI group with 0.28 (0.05-0.61) recurrence compared to 0.19 (0.14-0.24) in the Grade 1 BMI group (Figure 15).
Recurrence rate for Phasix™ mesh based on BMI
Recurrence rate for biological mesh based on BMI
Recurrence rate for cruroplasty based on BMI
Postoperative Dysphagia
Phasix™ ST mesh had the lowest dysphagia rate (3%; 95% CI 0.00-0.10) (Figure 16), followed by suture cruroplasty (8%; 95% CI 0.03-0.15) (Figure 17) and biological mesh (16%; 95% CI 0.07-0.27) (Figure 18). Studies reporting postoperative dysphagia showed moderate heterogeneity among Phasix™ mesh (I2=59%; p=0.09) and cruroplasty (I2=64%; p=0.04), but high heterogeneity among biological mesh (I2=88%; p<0.001).
Postoperative dysphagia following Phasix™ mesh repair
Postoperative dysphagia following cruroplasty repair
Postoperative dysphagia following biological mesh repair
Risk of Bias
To assess the risk of bias, we used the Cochrane risk of bias tool for randomized controlled trials and the ROBINS-I risk of bias tool for non-randomized trials. We believe that the included studies demonstrate fair or better quality (Tables 6-7). Additionally, we believe that the Phasix™ group had a lower follow-up compared to the others, which may have affected the results. We consider this to be a risk of bias.
Discussion
We conducted a meta-analysis review study comparing Phasix™ ST bioabsorbable mesh to biological mesh. We compared both of these options to primary repair (suture cruroplasty) in terms of recurrence rate, reoperation rate, and postoperative dysphagia. We analyzed 22 articles involving 2,008 patients who received different types of mesh or suture cruroplasty alone.
Our study found that the use of bioabsorbable mesh (Phasix™ ST mesh) for hiatal hernia repair resulted in a lower recurrence rate (5%) compared to biological mesh (16%) and suture cruroplasty (22%). We found no reoperation cases with the Phasix™ ST mesh, while the reoperation rates were 2% for biological mesh and 4% for suture cruroplasty. The recurrence rate was the lowest for Phasix™ ST mesh at all points of follow-up. In the biological mesh group, we observed a higher incidence of recurrence in the first year and after more than four years compared to intermediate follow-up times. Additionally, in the suture cruroplasty group, the incidence of recurrence increased over time. The biological mesh subgroup showed a higher recurrence incidence than Phasix™ ST mesh and a lower incidence compared to suture cruroplasty. Regarding the relationship between BMI and recurrence rate, we believe that we cannot rely on our results to determine the effect of BMI on the recurrence rate because many studies do not mention the mean BMI (unspecified BMI).
Recurrence Rate of Hiatal Hernia
A meta-analysis revealed that the recurrence rate of hiatal hernia was found to be higher in patients undergoing suture cruroplasty alone (42%) compared to repair with mesh (9%), but it was not stated whether these findings were statistically significant [27]. This literature supports our meta-analysis findings, which demonstrated a lower recurrence rate in hernia mesh repair, whether using Phasix™ ST or biological mesh, compared to cruroplasty.
Bioabsorbable Phasix™ ST Mesh Recurrence Versus Biological Mesh Recurrence
Limited studies on the use of Phasix™ ST mesh in hiatal hernia repair have shown recurrence rates between 0% and 9%, without significant differences [5-7,12]. The studies with biological mesh reported recurrence rates between 4% and 31%. The included biological mesh studies demonstrated significant differences in the overall recurrence rate, likely due to the various types of biological mesh used in each study. Our meta-analysis found that even within the subgroup of biological mesh, there was a significant difference in recurrence rates between mesh types (p=0.00). This highlights the importance of prospective studies comparing each specific type of biological mesh with Phasix™ ST mesh. Regardless, our included Phasix™ ST mesh studies showed lower recurrence rates than those observed with biological mesh.
Phasix™ ST mesh repair has demonstrated significantly higher strength compared to the natural abdominal wall at different time points after implantation. For example, in a porcine model, differences between the natural abdominal wall and Phasix™ ST mesh strength of reinforcement were as follows: 80% greater strength at eight weeks, 65% greater strength at 16 weeks, 58% greater strength at 32 weeks, and 37% greater strength at 48 weeks [28]. Moreover, Phasix™ ST mesh plays a crucial role in the initial healing phase, providing essential strength with rapid tissue ingrowth and vascularization due to its open-pore monofilament structure [29].
Reoperation Rate Following Hiatal Hernia Repair
We found that the reoperation rate was lower in the biological mesh group compared to the non-mesh group (suture cruroplasty) [3,10,11]. However, it is important to note that there was only a statistically significant difference between groups in one study [11]. As confirmed in our study, in all four studies where Phasix™ ST mesh was used for hiatal hernia repair, there was a 0% reoperation rate [4-7], compared to the biological mesh group, where the reoperation rate ranged from 2% to 7% [14-20], with an overall reoperation rate of 2%. For suture cruroplasty, we found a range of reoperation rates from 0% to 16%, with an overall reoperation rate of 4%. Additionally, in the double-arm meta-analysis, the randomized and non-randomized trials comparing biological vs. cruroplasty showed higher odds of reoperation among the cruroplasty group.
Postoperative Dysphagia Following Hiatal Hernia Repair
In our study, we found that postoperative dysphagia in the Phasix™ ST mesh group ranged from 0% to 10%, with an overall incidence of 3% without a significant difference between the studies. For studies using biological mesh, the postoperative dysphagia ranged from 3% to 34%, with a substantial difference between the studies (p=0.00) and an overall incidence of 16%. Regarding suture cruroplasty, we found that postoperative dysphagia ranged from 2% to 14%, with an overall incidence of 8% and a significant difference between the studies (p=0.04).
Limitations
Our meta-analysis has a few limitations. During our extensive research on hiatal hernia projects, we observed discrepancies in how hernia size is reported. We believe the existing literature requires new methods for reporting hiatal hernia to establish a consensus and promote a uniform approach to reporting hernia size. Another limitation includes the unavailability of data for BMI in many studies, which makes it difficult to conclude the effect of BMI on recurrence rate and reoperation. Accurate information regarding factors such as age, sex, the type of fundoplication, and other technical issues was lacking and varied between the studies. Moreover, in the Phasix™ mesh group, we found only one study with a follow-up of more than two years (24-40 months). We need longer follow-up periods to establish the possibility of late recurrence. We strongly believe that this issue has a significant impact when comparing hernia recurrences, reoperations, and complications and needs to be accurately addressed in future studies.
Conclusions
Phasix™ ST mesh showed the lowest recurrence, reoperation, and dysphagia rates compared to biological mesh and suture cruroplasty in hiatal hernia repair, making it a preferred option. However, our double-arm meta-analysis between patients who underwent suture cruroplasty and those who had reinforcement of the hiatal hernia repair with biological mesh showed no significant difference in recurrence and reoperation rates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hiatal hernia Stat Pearls [Internet] Smith RE Sharma S Shahjehan RD Treasure Island (FL)Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 562200/32965871 · pubmed ↗
- 2Surgical and clinical outcomes comparison of mesh usage in laparoscopic hiatal hernia repair Surg Endosc Armijo PR Krause C Xu T Shostrom V Oleynikov D 272427303520213255675710.1007/s 00464-020-07703-4 · doi ↗ · pubmed ↗
- 3Laparoscopic repair of very large hiatus hernia with sutures versus absorbable mesh versus nonabsorbable mesh: a randomized controlled trial Ann Surg Watson DI Thompson SK Devitt PG 28228926120152511912010.1097/SLA.0000000000000842 · doi ↗ · pubmed ↗
- 4Coated poly-4-hydroxybutyrate (Phasix ST™) mesh is safe and effective for hiatal hernia repair: our institutional experience and review of the literature Surg Endosc Fair L Ward M Adhikari P 8308363820243808201310.1007/s 00464-023-10604-x · doi ↗ · pubmed ↗
- 5Medium-term safety and efficacy profile of paraesophageal hernia repair with Phasix-ST® mesh: a single-institution experience Hernia Aiolfi A Cavalli M Sozzi A 2792862620223471683210.1007/s 10029-021-02528-z · doi ↗ · pubmed ↗
- 6Safety and efficacy of crura augmentation with Phasix ST mesh for large hiatal hernia: 3-year single-center experience J Laparoendosc Adv Surg Tech A Panici Tonucci T Asti E Sironi A Ferrari D Bonavina L 3693723020203191034810.1089/lap.2019.0726 · doi ↗ · pubmed ↗
- 7Surgical treatment of large and complicated hiatal hernias with the new resorbable mesh with hydrogel barrier (Phasix™ ST): a preliminary study J Robot Surg Konstantinidis H Charisis C 1411461720233539710710.1007/s 11701-022-01406-9 · doi ↗ · pubmed ↗
- 8Does bioabsorbable mesh reduce hiatal hernia recurrence rates? A meta-analysis Surg Endosc Clapp B Kara AM Nguyen-Lee PJ 229523033720233595112010.1007/s 00464-022-09514-1 · doi ↗ · pubmed ↗