Anomalous Origin of the Artery of Davidoff and Schechter Confirmed in a Case of Dural Arteriovenous Fistula of the Superior Sagittal Sinus
Masahiro Indo, Soichi Oya, Naoyuki Kakuda, Michihiro Tanaka, Shigeru Nemoto

TL;DR
A rare case confirms an unusual origin of the artery of Davidoff and Schechter in a dural arteriovenous fistula, highlighting the need for detailed angiographic evaluation.
Contribution
This case confirms an anomalous origin of the artery of Davidoff and Schechter from the P4 segment of the PCA in a dural AVF.
Findings
Angiography revealed a dural branch from the left P4 of the PCA feeding into the shunt.
Endovascular embolization significantly reduced shunt blood flow without complications.
ADS anomalies are poorly understood due to their low visibility in healthy individuals.
Abstract
Objective: The artery of Davidoff and Schechter (ADS) is a dural branch originating from the second segment of the posterior cerebral artery (PCA). ADS may not be discernible even with angiography and is identified when it develops as a feeder in arteriovenous malformations (AVMs), dural arteriovenous fistulas (AVFs), or tumors. Herein, we describe a case of dural AVF of the superior sagittal sinus (SSS) that caused seizures. Clinical presentation: A 72-year-old woman had a seizure caused by a dural AVF at the SSS with the bilateral middle meningeal and occipital arteries as major feeders and marked reflux into the bilateral cortical veins via bridging veins. The angiography revealed a dural branch from the left fourth segment (P4) of the PCA entering the falx via the medial surface of the cerebellar tentorium and feeding into the shunt, which was thought to be the anomalous origin of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
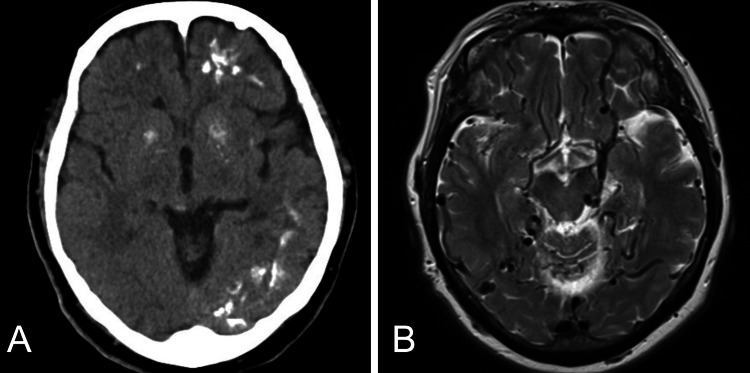 Figure 1
Figure 1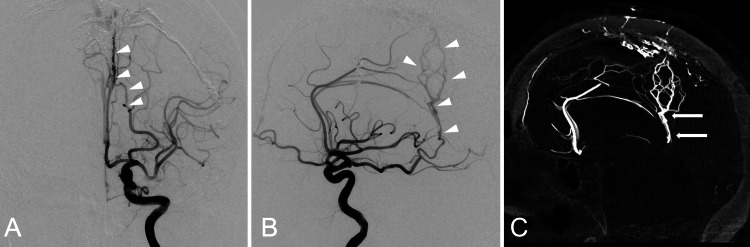 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Intracranial Aneurysms: Treatment and Complications · Trigeminal Neuralgia and Treatments
Introduction
The artery of Davidoff and Schechter (ADS) is a dural branch of the posterior cerebral artery (PCA), first described by Wollschlaeger and Wollschlaeger in a cadaver study [1]. It typically originates from the second PCA segment (P2), runs parallel to the PCA, travels posterolaterally around the midbrain, crosses the trochlear nerve to enter the cerebellar tentorium, supplies the medial and inferior surfaces of the tentorium, and eventually turns medially, reaching the falx [2,3]. In conventional cerebral angiography, it can be difficult to delineate but can be identified as a feeder in conditions like arteriovenous malformations (AVMs), dural arteriovenous fistulas (AVFs), and tumors [2-4]. The ADS is a dural branch; however, it has been reported that it may also have branches to the midbrain and cerebellum [5]. Here, we report on a case of a superior sagittal sinus (SSS) dural AVF in which the ADS, serving as one of the feeders, originated from the fourth segment (P4) of the PCA.
Case presentation
A 72-year-old woman without a significant medical history was transferred to our hospital because of a seizure. Computed tomography revealed numerous calcified lesions in the left cerebral hemisphere, and magnetic resonance imaging revealed marked dilatation of the cerebral veins throughout the cerebrum (Figure 1). Cerebral angiography showed a dural AVF at the SSS with the bilateral middle meningeal and occipital arteries as major feeders and marked reflux into the bilateral cortical veins via bridging veins. The diagnosis was dural AVF, Cognard type IIa+b, Borden type II. Selective left internal carotid angiography revealed a fetal posterior communicating artery and a dural branch from the left P4 entering the falx via the medial surface of the cerebellar tentorium and feeding into the shunt, which was thought to be the anomalous origin of the ADS (Figure 2). The embolization procedure was meticulously performed to prevent retrograde flow of the embolic material into the ADS, particularly due to potential small-branch occlusions invisible on pre-embolization angiography. This approach resulted in a significant reduction in the shunt blood flow. The patient’s postoperative course was favorable, and she was subsequently transferred to a rehabilitation hospital.
Preoperative imagings(A) Computed tomography revealing multiple calcified lesions in the left cerebral hemisphere. (B) Magnetic resonance imaging showing vein dilatation in the whole cerebrum
Preoperative angiogramsAVF: arteriovenous fistulaLeft internal carotid angiograms show the anteroposterior view (A) and lateral view (B). The artery of Davidoff and Schechter (ADS) originates from the P4 of the posterior cerebral artery, running in the medial upper anterior direction. It reaches the median and then runs along the falx to the shunt point of the superior sagittal sinus (white arrowheads). The sagittal image of 3D-rotational angiography (C) shows that the ADS (white arrows) entered the cerebellar tentorium at the falcotentorial junction, running into the falx and becoming feeders of dural AVF
Discussion
In this article, we reported the first case of a very rare vascular anomaly in which ADS originates from P4 of the PCA on cerebral angiography. Few reports have detailed the anatomical characteristics of ADS [2]. ADS on cerebral angiography was initially described by Weinstein et al. [3]. According to this report, the ADS originates from the PCA, travels around the midbrain, runs toward the falcotentorial junction, and turns anteriorly upward when it reaches the midline. However, the exact location of the origin is difficult to identify in their report. Bojanowski et al. demonstrated that the ADS originates from P2 in cerebral angiography and emphasized that the ADS is difficult to identify using conventional cerebral angiography, with confirmation only possible in diseases in which the ADS is a feeder [4]. All ADSs documented in the literature were identified as feeders for AVFs, AVMs, and tumors using cerebral angiography. There have been no reports of ADS identified on conventional cerebral angiography in patients without these abnormalities [2-4,6-8]. A medial tentorial dural branch may also originate from the superior cerebellar artery, and this dural branch is called the artery of Wollschlaeger and Wollschlaeger (AWW) [9]. In some papers, the two have been conflated and discussed [10]; however, ADS is defined as the dural branch of the PCA, which is distinct from the AWW.
ADS may be clinically significant in falcotentorial lesions. It typically does not supply brain tissue other than the dura mater, but it may provide blood supply to the vermis cerebelli and inferior colliculus [5]. Given that this anomalous ADS originated in the P4, we cautiously considered the potential risk of temporal or occipital lobe infarction during embolization. Onyx is a liquid embolic material commonly used for dural AVFs embolization. Although this allows for efficient embolization of feeders, extreme caution is necessary because it can suddenly and unpredictably flow back into numerous other branches at the shunt point. Although a previous report describes a favorable outcome from embolization via the ADS [6], caution is warranted regarding the procedure because of the risk of embolic complications from the branches supplying the brain tissue. In our opinion, ADS should be considered as a potentially hazardous anastomosis even if it is not visualized on cerebral angiography. Although this anomaly is rare, the presence of such variants can be critical during endovascular interventions to treat feeders in shunt-related conditions such as AVF and AVM of the cerebellar or falcotentorial regions.
Conclusions
The understanding of the frequency and pattern of anomalies in ADS remains insufficient owing to their limited visibility in angiographic studies of normal patients. This report demonstrates that ADS can originate from the P4 of the PCA. In order to prevent ischemic complications during embolization in the cerebellar or falcotentorial region, it is essential to consider the potential presence of rare feeders via the falx and the cerebellar tentorium. The presence of such variants can be crucial when conducting endovascular treatments for lesions in the cerebellum or falcotentorial region.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An infratentorial meningeal artery (Article in German)Radiologe Wollschlaeger PB Wollschlaeger G 45145251965 https://pubmed.ncbi.nlm.nih.gov/5888134/5888134 · pubmed ↗
- 2The artery of Davidoff and Schechter: an anatomical study with neurosurgical case correlates Br J Neurosurg Griessenauer CJ Loukas M Scott JA Tubbs RS Cohen-Gadol AA 815818272013 https://doi.org/10.3109/02688697.2013.7988562370558110.3109/02688697.2013.798856 · doi ↗ · pubmed ↗
- 3Meningeal branch of the posterior cerebral artery Neuroradiology Weinstein M Stein R Pollock J Stucker TB Newton TH 12913171974 https://doi.org/10.1007/BF 00344317484203510.1007/BF 00344317 · doi ↗ · pubmed ↗
- 4Angiographic demonstration of the meningeal branch of the posterior cerebral artery AJNR Am J Neuroradiol Bojanowski WM Rigamonti D Spetzler RF Flom R 80891988 https://pubmed.ncbi.nlm.nih.gov/3135732/3135732 PMC 8332018 · pubmed ↗
- 5Microsurgical anatomy of the region of the tentorial incisura J Neurosurg Ono M Ono M Rhoton AL Jr Barry M 365399601984 https://doi.org/10.3171/jns.1984.60.2.0365669396410.3171/jns.1984.60.2.0365 · doi ↗ · pubmed ↗
- 6Angiography and selective microcatheter embolization of a falcine meningioma supplied by the artery of Davidoff and Schechter: case report J Neurosurg Hart JL Davagnanam I Chandrashekar HS Brew S 7107131142011 https://doi.org/10.3171/2010.4.JNS 102182048689210.3171/2010.4.JNS 10218 · doi ↗ · pubmed ↗
- 7Treatment of dural fistulas involving the deep cerebral venous system AJNR Am J Neuroradiol Halbach VV Higashida RT Hieshima GB Wilson CB Hardin CW Kwan E 393399101989 https://pubmed.ncbi.nlm.nih.gov/2494859/2494859 PMC 8331397 · pubmed ↗
- 8Tentorial dural fistulas: endovascular management and description of the medial dural-tentorial branch of the superior cerebellar artery AJNR Am J Neuroradiol Byrne JV Garcia M 179818043420132366029310.3174/ajnr.A 3519 PMC 7965633 · doi ↗ · pubmed ↗