Endoscopic and rectal tube management of pediatric sigmoid volvulus: A case series
Sapna Khemka, Micah Morris, Kevin Watson

TL;DR
This case series describes the successful endoscopic and rectal tube management of three pediatric patients with rare sigmoid volvulus, preventing severe complications.
Contribution
The paper presents a novel approach combining endoscopic detorsion and rectal decompression tube placement for initial stabilization in pediatric sigmoid volvulus.
Findings
Endoscopic detorsion and rectal decompression tube placement effectively stabilized three pediatric patients with sigmoid volvulus.
Two patients required subsequent surgical resection of redundant sigmoid colon after initial stabilization.
The approach prevented complications like perforation, necrosis, or sepsis in the studied cases.
Abstract
The process of the sigmoid colon twisting on its mesentery is known as sigmoid volvulus, a diagnosis rarely seen in the pediatric population. Volvulus can lead to blood flow obstruction of the colon and eventually perforation, necrosis, or sepsis. Predisposing factors include chronic constipation, chronic dysmotility, or Hirschsprung disease. This communication demonstrates three patients who presented to a tertiary pediatric care center with a diagnosis of sigmoid volvulus. All three patients underwent immediate endoscopic detorsion and rectal decompression tube placement. Two patients subsequently underwent surgical resection of redundant sigmoid colon. This communication highlights the use of sigmoidoscopy for detorsion of uncomplicated sigmoid volvulus with added support for initial rectal decompression tube placement, contributing to initial patient stabilization and positive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
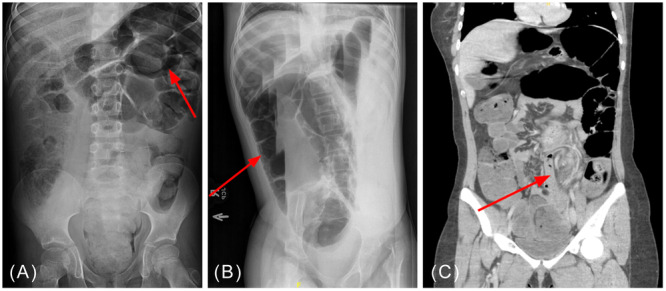 Figure 1
Figure 1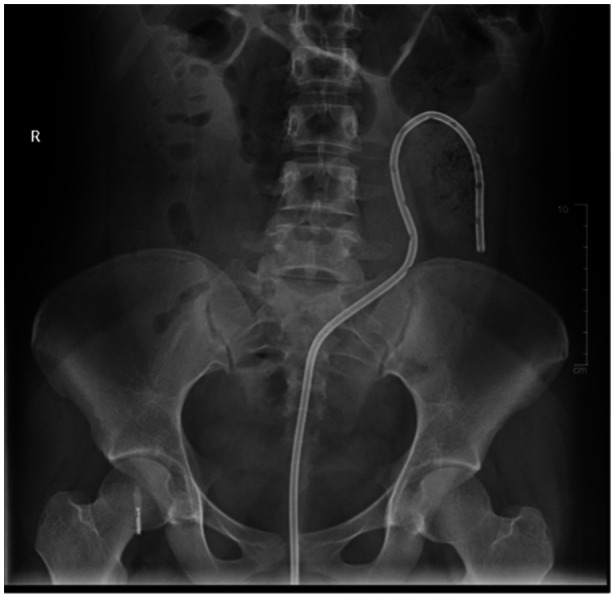 Figure 2
Figure 2- —None
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal Malrotation and Obstruction Disorders · Pediatric Hepatobiliary Diseases and Treatments · Intestinal and Peritoneal Adhesions
INTRODUCTION
1
Sigmoid volvulus occurs when the redundant sigmoid colon twists on its narrow and elongated mesentery, leading to vascular obstruction and closed loop distention.1, 2 Predisposing factors include older age, chronic constipation, dysmotility, especially in the setting of neurodevelopmental disorders, Hirschsprung disease (HD), and roundworm infection.1, 3, 4, 5 Patients can present with abdominal pain, distension, constipation, obstipation, nausea, and vomiting.1 Laboratory workup is often unremarkable but can exhibit leukocytosis, while abdominal imaging typically demonstrates dilated colon proximal to obstruction.1, 3 Diagnosis is considered a medical emergency, and patients may require endoscopic detorsion followed by colonic resection to prevent recurrence.1, 3 Without urgent intervention, the volvulus can lead to perforation, necrosis, or sepsis due to vascular infarction.3
CASE SERIES
2
We present three patients diagnosed with sigmoid volvulus on imaging at a pediatric tertiary care center, prompting sigmoidoscopic detorsion with rectal decompression tube placement. Management provided prompt relief of symptoms without immediate recurrence of sigmoid volvulus.
Patient A, an 8‐year‐old male with developmental delay and chronic constipation, presented in January 2018 with 2 days of emesis, abdominal pain, and abdominal distension concerning for bowel obstruction. The previous HD evaluation was negative. At the outside emergency department (ED), he received Fleet® enema and produced two large bowel movements before any diagnostic imaging. Upon transfer to a tertiary care center, an abdominal x‐ray demonstrated colonic distension consistent with sigmoid volvulus (Figure 1A). The next day, Patient A underwent endoscopic detorsion with rectal decompression tube placement. After 2 days, he returned to the operating room (OR) for redundant sigmoid colon resection with end‐end anastomosis. Patient A was discharged home 7 days after detorsion and 5 days after surgical resection with no recurrence of volvulus after initial presentation.
Radiographic images demonstrating classic signs seen in sigmoid volvulus. (A) Patient A's abdominal x‐ray demonstrating dilated colon. (B) Patient B's left lateral decubitus x‐ray demonstrating “coffee bean sign.” (C) Patient C's abdominal computed tomography demonstrating “whirl sign.”
Patient B, an 11‐year‐old female with spastic tetraplegic cerebral palsy and gastrostomy‐jejunostomy (GJ) tube feed dependence, presented in March 2017 with 3 days of constipation, abdominal distension, and feeding intolerance to a routine outpatient pulmonology appointment. Chest x‐ray was obtained for evaluation of chronic respiratory failure where colonic gaseous distension was noted. Patient B had not previously undergone HD evaluation. Subsequent abdominal x‐ray demonstrated colonic dilation measuring 12 cm in diameter with air in the nondependent side on the left lateral decubitus film, concerning for sigmoid volvulus (Figure 1B). The patient was immediately taken to the OR for colonoscopic detorsion. The sigmoid colon was redundant and dilated despite the absence of converging colonic mucosa (whirl sign), prompting rectal decompression tube placement. Four days after endoscopic detorsion, Patient B tolerated feeds and was discharged home. This patient did not undergo interval sigmoidectomy due to diagnostic uncertainty of volvulus versus ileus in the setting of chronic medical illness. She has had no recurrence of volvulus but has had further episodes of ileus.
Patient C, a 16‐year‐old female with history of abdominal migraines, presented with 4 days of abdominal pain, constipation, and worsening abdominal distention in January 2023. An abdominal computed tomography (CT) scan performed at the referring ED demonstrated concern for sigmoid volvulus (Figure 1C), prompting transfer to the tertiary care center. She successfully underwent endoscopic detorsion and rectal decompression tube placement the same day. Tubing was displaced with bowel movement 3 days after placement. Patient C was discharged home with no acute issues. Surgical intervention was postponed due to the initial severity of Patient C's symptoms and marked improvement after detorsion; instead, proceeding with an elective surgery after discharge. Patient C did not have any volvulus recurrence before undergoing sigmoidectomy of redundant colon with end‐end anastomosis 2 months after detorsion. Rectal biopsy at the time was negative for HD. Patient C has had no recurrence of volvulus.
DISCUSSION
3
Volvulus in the pediatric population is often isolated in the small bowel due to association with malrotation or internal hernia, making sigmoid volvulus a rare pediatric diagnosis.2, 6 Damkjaer et al. reports only 100 pediatric cases of sigmoid volvulus from 1940 to 2021.6 Common associations with pediatric sigmoid volvulus include chronic constipation and neuropsychiatric disorders. Other predisposing factors include a high‐fiber diet, dysmotility, pregnancy, and HD.2 In this case series, Patient A had a history of chronic constipation, which most likely contributed to his episode of sigmoid volvulus. Patient B may have had underlying dysmotility requiring GJ tube feedings. Patient C did not have a notable history of increased risk of sigmoid volvulus. Previous studies demonstrate an incidence of HD in up to 18% of patients with sigmoid volvulus, making it imperative that this etiology is ruled out during evaluation to prevent recurrence and further complications such as constipation.3 Evaluation for HD was performed in both Patients A and C, whereas Patient B had not undergone evaluation.
Imaging can be useful in the diagnosis of sigmoid volvulus when patients present with relevant symptoms, including abdominal pain, constipation, and/or emesis. Abdominal x‐ray is the first choice imaging modality.7 Classic signs of sigmoid volvulus include a dilated colon with a “U shape,” also known as a coffee bean sign or a bird beak appearance such as that seen in Figure 1A,B.6 The addition of barium enema increases radiographic diagnostic sensitivity when abdominal x‐rays are nonspecific for sigmoid volvulus in pediatrics.6, 7 An abdominal CT scan may be performed if x‐ray is inconclusive despite a high index of suspicion. Abdominal CT imaging would be expected to demonstrate the rotation of the colonic mesentery represented by a “whirl sign,” as seen in Figure 1C.6 Inflammation of the colonic wall, distension of the sigmoid colon, and bowel obstruction with proximal dilation may also represent sigmoid volvulus on imaging.6
While most literature describes the treatment of sigmoid volvulus to be in the adult population given larger diagnostic and treatment incidence, a systematic review conducted by Parolini et al. describes initial management of sigmoid volvulus in childhood to include water contrast enema along with endoscopic detorsion and decompression if no other contraindications such as bowel necrosis, gangrene, perforation, or peritonitis are already present.3, 4, 5 After initial detorsion, rectal decompression tube placement remains a topic of discussion for mainstay treatment to prevent early relapse of volvulus, while definitive treatment has been demonstrated by colonic resection.2 Damkjaer et al. has demonstrated up to 35% recurrence of volvulus without sigmoidectomy.6 There has also been increased recurrence noted in patients who have spontaneous decompression of sigmoid volvulus, which Aksunger et al. describe as up to 2% of cases worldwide.8 These data make Patient B's presentation possibly a spontaneously reduced sigmoid volvulus or, more likely, an ileus versus a sigmoid volvulus despite initial imaging given the absence of recurrence.
Pediatric patients require general anesthesia while undergoing colonic detorsion in the OR. As the endoscope enters the colon, a whirl sign may be present at the recto‐sigmoid junction indicating the distal end of the sigmoid volvulus.3, 9 The endoscope is advanced into the dilated colon and immediate suctioning is performed as the scope is torqued clockwise.9 The endoscope is further advanced to the proximal point of the volvulus, where additional suctioning is performed.9 Once detorsion and initial decompression of the dilated sigmoid loop have been completed, a rectal decompression tube may be placed to provide patient stabilization and prevent early volvulus relapse.3, 10, 11 A guidewire is inserted through the endoscopic channel and advanced into the descending colon as the endoscope is withdrawn. The rectal tube catheter is placed over the guidewire and advanced under fluoroscopy past the point of colonic obstruction (Figure 2). The guidewire is removed, and the rectal tube is secured via tape to the perianal skin and left in place for several days.9 The endoscope may be reintroduced to secure tubing to the colonic mucosa with endoscopic clip before surgical resection.3, 10 The goals of endoscopic detorsion with the placement of rectal decompression tube focus on relieving the obstruction while preventing bowel ischemia and recurrence.9 The complications that may occur with colonic detorsion include the risk of bleeding, infection, and perforation. These risks are increased in an emergent surgical intervention setting compared to an elective operation.9 Broad‐spectrum antibiotic administration is only necessary in the setting of concern for peritonitis, sepsis, or ischemia.9 Another risk that must be considered is the inability to endoscopically reduce the torsion, requiring further and emergent surgical intervention.
Patient C's abdominal x‐ray demonstrating rectal decompression tube catheter after placement.
Although sigmoid volvulus is rarely seen in the pediatric population, a high index of suspicion allows for early detection and intervention, preventing the development of consequences including perforation, necrosis, and septic shock.2, 3 All three patients described successfully underwent endoscopic detorsion within 24 h of presentation, allowing for early intervention and reduced risk of morbidity. This case series suggests that sigmoidoscopy may be an effective approach for detorsion of uncomplicated pediatric sigmoid volvulus. It also highlights the use of rectal decompression tubes, as none of the patients experienced acute recurrence during hospitalization, contributing to initial patient stabilization and positive patient outcomes.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
ETHICS STATEMENT
This case series was reviewed and deemed exempt from institutional review board oversight. Informed consent was obtained from the parents/guardians of all patients for the publication of case details.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Baiu I , Shelton A . Sigmoid volvulus. JAMA. 2019;321(24):2478. 10.1001/jama.2019.2349 31237646 · doi ↗ · pubmed ↗
- 2Madhavnarayan Totadri V , Vetri R , Sainath S . Pediatric sigmoid volvulus: a report on two cases. Cureus. 2022;14(8):e 28400. 10.7759/cureus.28400 36168370 PMC 9506677 · doi ↗ · pubmed ↗
- 3Parolini F , Orizio P , Bulotta AL , et al. Endoscopic management of sigmoid volvulus in children. World J Gastrointest Endosc. 2016;8(12):439‐443. 10.4253/wjge.v 8.i 12.439 27358669 PMC 4919692 · doi ↗ · pubmed ↗
- 4Destro F , Maestri L , Meroni M , et al. Colonic volvulus in children: surgical management of a challenging condition. Children. 2021;8(11):982. 10.3390/children 8110982 34828695 PMC 8625683 · doi ↗ · pubmed ↗
- 5Hencke J , Loff S . Recurrent sigmoid volvulus in children—our experience and systematic review of the current literature. Children. 2023;10(9):1441. 10.3390/children 10091441 37761402 PMC 10528811 · doi ↗ · pubmed ↗
- 6Damkjaer MB , Farooqui W , Ifaoui I , Penninga L . Sigmoid volvulus in children. BMJ Case Rep. 2021;14(5):e 241869. 10.1136/bcr-2021-241869 PMC 811799533980558 · doi ↗ · pubmed ↗
- 7Chang PH , Jeng CM , Chen DF , Lin LH . A case report and literature review of sigmoid volvulus in children. Medicine. 2017;96(52):e 9434. 10.1097/MD.0000000000009434 29384922 PMC 6392894 · doi ↗ · pubmed ↗
- 8Aksungur N , Peksoz R , Disci E , Atamanalp SS . Spontaneous decompression of sigmoid volvulus. Pak J Med Sci. 2023;39(6):1616‐1619. 10.12669/pjms.39.6.8052 37936730 PMC 10626113 · doi ↗ · pubmed ↗