Safe transanal drainage tube placement using a tapered-tip sheath system for obstructive colorectal cancer
Fumioki Toyoda, Masataka Yokode, Tomoaki Matsumori, Munehiro Ikeda, Takahiro Utsumi, Yuki Nakanishi, Hiroshi Seno

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
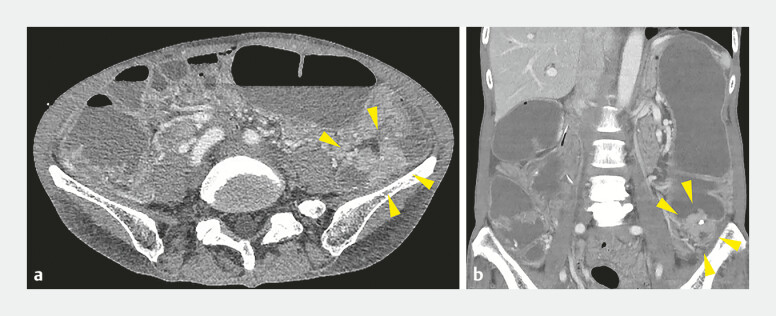 Fig. 1
Fig. 1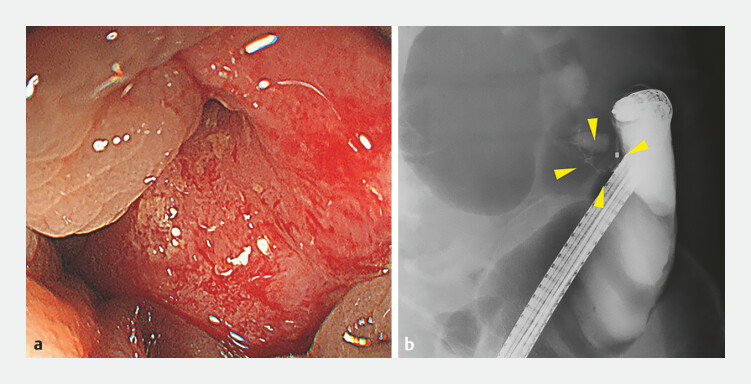 Fig. 2
Fig. 2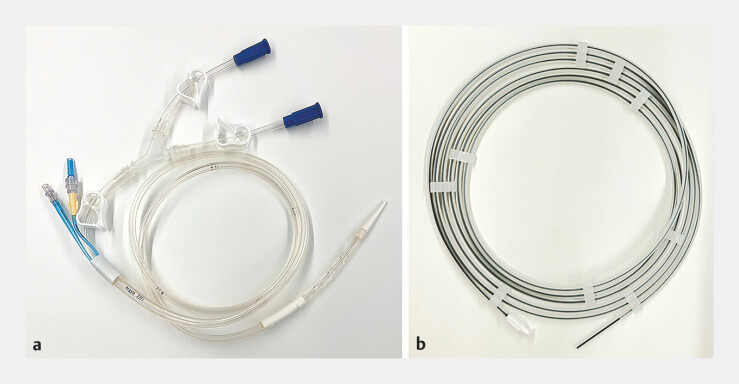 Fig. 3
Fig. 3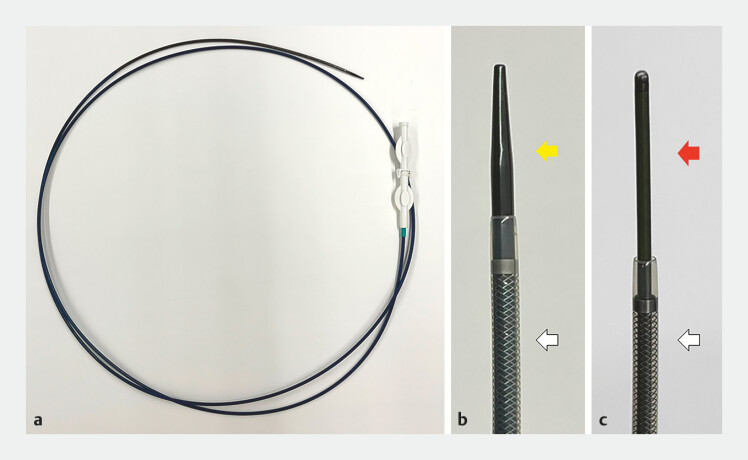 Fig. 4
Fig. 4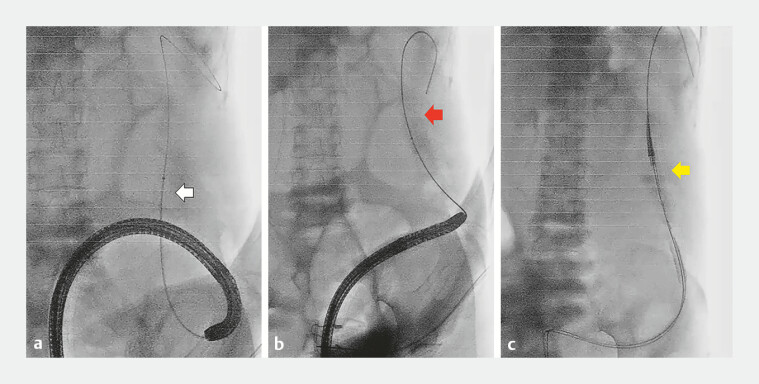 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Colorectal and Anal Carcinomas · Gallbladder and Bile Duct Disorders
A 67-year-old woman presented at our hospital with abdominal bloating and pain. Abdominal computed tomography revealed sigmoid colon thickening and proximal bowel dilatation ( Fig. 1 ). Emergency colonoscopy revealed advanced colorectal cancer with almost complete obstruction ( Fig. 2 ). Consequently, endoscopic decompression using a transanal drainage tube (TDT) (Argyle Fukuroi Dennis Colorectal tube, Cardinal Health) was attempted ( Fig. 3 ). However, the equipped 0.055-inch guidewire could not pass through the stenosis because of its stiffness. Therefore, a 0.035-inch hydrophilic biliary guidewire (Hydra Jagwire, Boston Scientific) preloaded through a biliary catheter (MTW, MTW Endoskopie) was used and successfully passed through the stenosis. The biliary catheter was then exchanged with a tapered-tip sheath system (EndoSheather, Piolax) composed of a tapered inner catheter and outer sheath ( Fig. 4 a, b ). The system passed smoothly through the stenosis. After the inner catheter and biliary guidewire were withdrawn, the equipped guidewire was inserted into the outer sheath ( Fig. 4 c , Fig. 5 a, b ). Subsequently, the colonoscope and outer sheath were removed, and the sigmoid colon was straightened using the equipped guidewire. Finally, the TDT was successfully placed ( Fig. 5 c , Video 1 ).
Abdominal contrast-enhanced computed tomography images. Horizontal ( a ) and coronal ( b ) images show wall thickening in the sigmoid colon (yellow arrowheads) and proximal bowel dilatation.
Colonoscopy and fluoroscopy. a Colonoscopy image showing almost complete bowel obstruction caused by colorectal cancer. b Fluoroscopic image of severe stenosis due to the tumor (yellow arrowheads).
Images of the transanal drainage tube. a Overall view of a transanal drainage tube (Argyle Fukuroi Dennis Colorectal Tube, Cardinal Health). b The 0.055-inch guidewire equipped with the tube.
Images of the tapered-tip sheath system. a )Overview of the tapered-tip sheath system (EndoSheather, Piolax). b The tapered-tip inner catheter tip (yellow arrow) and outer sheath (white arrow). ( c ) Tip of the 0.055-inch equipped guidewire (red arrow) and outer sheath (white arrow).
Fluoroscopic images of transanal drainage tube placement. a Placement of the tapered-tip sheath system over the hydrophilic biliary guidewire (white arrow). b Insertion of the 0.055-inch guidewire (red arrow) into the outer sheath. c Insertion of the transanal drainage tube (yellow arrow) through the stenosis over the 0.055-inch guidewire.
This video shows the procedure for transanal drainage tube placement using a tapered-tip sheath system for obstructive colorectal cancer.Video 1
TDT placement is effective in preventing emergency surgery for patients with malignant colorectal obstruction 1 2 . The equipped guidewire is rigid enough to facilitate TDT placement; however, its stiffness may make it difficult to pass through the stenosis and may cause perforation 3 . Hydrophilic biliary guidewires are useful in such cases 4 , but cannot be exchanged with an equipped guidewire through a biliary catheter because of their thickness. As in this case, the tapered-tip sheath system, first developed for bile duct biopsy 5 , enables a hard-equipped guidewire to pass through the malignant colorectal stenosis. This system may be useful for safe TDT placement in cases of unsuccessful insertion of an equipped guidewire using the usual method.
Endoscopy_UCTN_Code_TTT_1AQ_2AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lelcuk S Ratan J Klausner JM Endoscopic decompression of acute colonic obstruction. Avoiding staged surgery Ann Surg 198620329229410.1097/00000658-198603000-000133954481 PMC 1251093 · doi ↗ · pubmed ↗
- 2Horiuchi A Maeyama H Ochi Y Usefulness of Dennis Colorectal Tube in endoscopic decompression of acute, malignant colonic obstruction Gastrointest Endosc 20015422923210.1067/mge.2001.11645611474399 · doi ↗ · pubmed ↗
- 3Ohnita K Shikuwa S Isomoto HA new thin endoscopic method of transanal drainage tube insertion for acute colonic obstruction due to colorectal cancer Dig Endosc 20092125225410.1111/j.1443-1661.2009.00901.x 19961524 · doi ↗ · pubmed ↗
- 4Ichise Y Horiuchi A Nakayama Y Techniques and outcomes of endoscopic decompression using transanal drainage tube placement for acute left-sided colorectal obstruction Gastroenterol Res 2010320120610.4021/gr 233w PMC 513971627956997 · doi ↗ · pubmed ↗
- 5Matsumori T Uza N Shiokawa M Clinical impact of a novel device delivery system in the diagnosis of bile duct lesions: A single-center experience J Gastroenterol Hepatol 2022371360136635434844 10.1111/jgh.15866 · doi ↗ · pubmed ↗