Same-session endoscopic ultrasound-guided gallbladder drainage for acute cholecystitis with lumen-apposing metal stent and rendezvous for biliary stones in invisible papilla
Davide Scalvini, Aurelio Mauro, Stefano Mazza, Carlo Ciccioli, Marco Bardone, Francesca Torello Viera, Andrea Anderloni

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
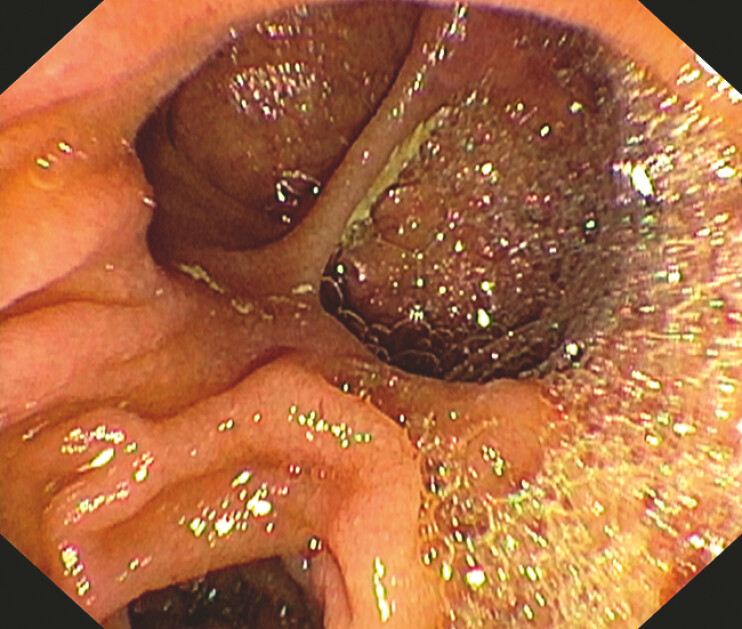 Fig. 1
Fig. 1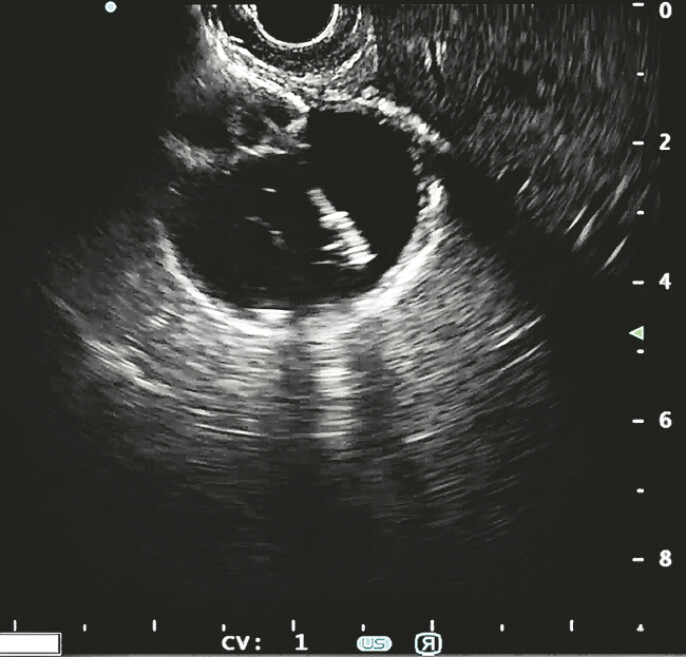 Fig. 2
Fig. 2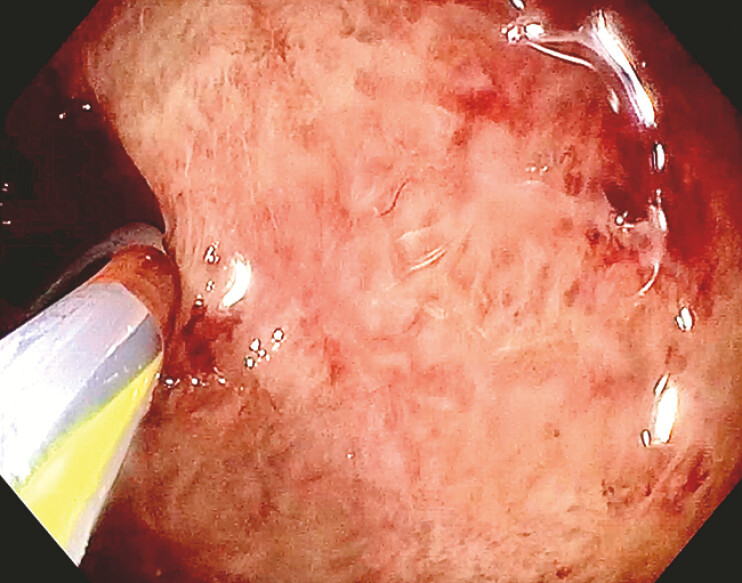 Fig. 3
Fig. 3 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Biliary and Gastrointestinal Fistulas
EUS-guided gallbladder drainage (EUS-GBD) is increasing its use for distal biliary malignant obstruction and in case of acute cholecystitis in frail or unfit for surgery patients 1 . However, in the case of concomitant choledocholithiasis, an ERCP is usually necessary to remove biliary stones, and new techniques have been explored 2 . In this video-case report, we present a single-session EUS-GB for acute cholecystitis with LAMS and an innovative biliary stones clearance with a gallbladder rendezvous ( Video 1 ).
Video of a EUS-gallbladder drainage for acute cholecystitis with lumen-apposing metal stent and a gallbladder rendezvous for biliary stones in invisible papilla done in a single session.Video 1
This case involves an 85 year-old woman who was admitted for acute cholecystitis and common bile duct (CBD) stones, after multidisciplinary evaluation, she has been considered frail and unfit for surgery, thus an EUS-GB and an ERCP were proposed.
ERCP was started but it was suspended for inability to find the major papilla which seems to be dislocated by a duodenal diverticulum ( Fig. 1 ). EUS-GBD was effectively performed from the antrum, with a 15 × 10 mm EC-LAMS (Hot Axios, Boston Scientific) ( Fig. 2 ). Subsequently, a large balloon dilation was employed to dilate the LAMS up to 15 mm and to do a direct cholecystoscopy with a standard gastroscope ( Fig. 3 ). Using a 0.035 × 450 cm guidewire on a sphincterotome, the cystic duct was cannulated, and then the guidewire was advanced anterograde into the CBD and further into the duodenum. Anterograde cholangiography confirmed the presence of choledocholithiasis. The papilla was anterograde dilated with a balloon up to 12 mm, and the guidewire was maintained in the duodenum. Then, a duodenoscope with a lateral-view was reintroduced, and, with the guidewire still in place to facilitate an easier cannulation ( Fig. 4 ), the CBD was cleared from three small stones using an extractor balloon.
Invisible papilla dislocated by a duodenal diverticulum.
EUS-guided gallbladder drainage.
Cholecystoscopy evaluating gallbladder inflamed mucosa.
Fluoroscopic image of rendezvous from the gallbladder and retrograde biliary cannulation with a second guidewire.
This is another evidence on the potentiality of EUS-GBD with LAMS. The use of larger LAMS allowed access to the gallbladder, to perform biliary rendezvous for invisible papilla for a concomitant acute cholecystitis drainage and CBD stones clearance.
Endoscopy_UCTN_Code_TTT_1AR
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Binda C Anderloni A Forti EEUS-Guided Gallbladder Drainage Using a Lumen-Apposing Metal Stent for Acute Cholecystitis: Results of a Nationwide Study with Long-Term Follow-Up Diagnostics 20241441338396453 10.3390/diagnostics 14040413 PMC 10887962 · doi ↗ · pubmed ↗
- 2Fugazzola P Bianchi CM Calabretto F Intraoperative transcystic laparoscopic common bile duct stone clearance with Spy Glass discover during emergency and elective cholecystectomy: a single-center case series World J Emerg Surg 202419838438899 10.1186/s 13017-023-00529-0PMC 10913229 · doi ↗ · pubmed ↗