Medication adherence scales in non-communicable diseases: A scoping review of design gaps, constructs and validation processes
Maria Jose, Priyanka Rajmohan, T. S. Sulfath, Ravi Prasad Varma, Manoj Mohan, Nisha K. Jose, Jerin Jose Cherian, Mohan Lal Bairwa, Tulika Goswamy, Aditi Apte, Praveenlal Kuttichira, Joe Thomas

TL;DR
This review examines medication adherence scales for non-communicable diseases, finding many lack validation and fail to consider socioeconomic and cultural factors.
Contribution
The study identifies design gaps and psychometric limitations in existing adherence scales for non-communicable diseases.
Findings
140 articles identified 57 adherence scales, most developed using mixed methods but often neglecting cost-related and systemic barriers.
Psychometric properties varied widely, with many scales lacking validation in diverse settings.
The review highlights the need for more holistic, context-sensitive adherence tools that include socioeconomic and cultural factors.
Abstract
NCDs arise from complex interactions of modifiable factors such as unhealthy lifestyles, poor diet, and psychosocial challenges, along with non-modifiable factors like age and genetics. Notably, medication non-adherence is a widespread and growing concern, significantly contributing to disease progression and poor outcomes globally. This scoping review aims to synthesize evidence on medication adherence scales used for selected non communicable diseases. It examines their development methods, psychometric properties, and assessed domains, while identifying gaps or limitations in their design and application. The Joanna Briggs Institute methodological framework guided this scoping review and the protocol was registered prospectively to ensure methodological transparency and rigor. Electronic databases, the reference list of included articles, and grey literature were searched. Studies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
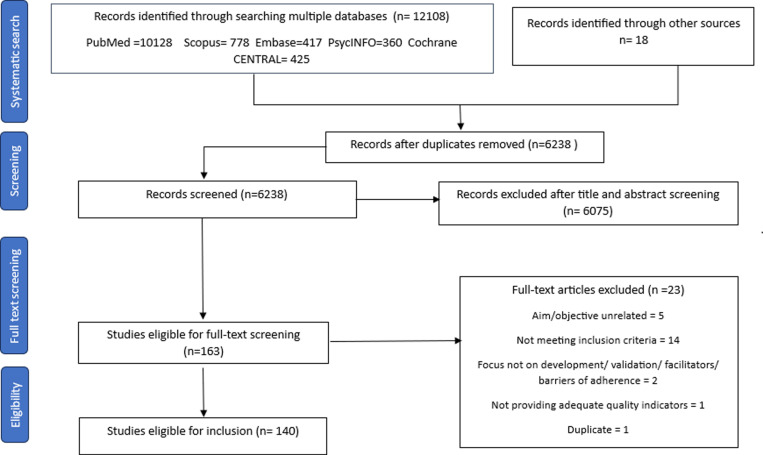 Fig 1
Fig 1- —http://dx.doi.org/10.13039/501100001411Indian Council of Medical Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedication Adherence and Compliance
Introduction
Background
‘Medication adherence’ is defined as the extent to which a person’s medication-taking behavior corresponds with agreed recommendations from a healthcare provider [1]. Adherence to medication is a crucial aspect of patient care and is indispensable for achieving clinical goals. The World Health Organization’s report on medication adherence states that “increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than any improvement in specific medical treatment” [1]. However, adherence rates remain suboptimal worldwide. In developed countries, only 50% of patients treated for chronic diseases adhere to prescribed treatments, with adherence rates being even lower in developing countries [2].
Non-communicable diseases (NCDs) contribute to a significant proportion of morbidity and mortality, with inadequate control of these conditions often linked to poor medication adherence. Socioeconomic constraints, language barriers, multimorbidity, mental health challenges, limited healthcare access, and lifestyle factors all influence adherence [3,4]. Patients with limited financial resources may be forced to prioritize daily expenses over purchasing medications, leading to treatment discontinuation [5].
Additionally, language barriers hinder effective communication between patients and healthcare providers, increasing the risk of misinterpretation of prescription instructions and improper medication use [6]. Patients with multimorbidity face greater medication burden, often requiring complex dosing regimens that heighten the risk of non-adherence due to polypharmacy and treatment fatigue. Studies have shown that as the number of prescribed medications increases, adherence tends to decline, particularly among elderly patients managing multiple chronic conditions [7].
NCDs contribute to around 38 million (68%) of all deaths globally and to about 5.87 million (60%) of all deaths in India [2]. Medication non-adherence rates range from 18.7% to 74% [8–11], with 30% of medicine-related hospital admissions attributed to non-adherence [12,13]. Given the dynamic nature of patient behaviors, accurately assessing adherence remains a challenge for healthcare professionals [14,15].
Non-adherence is multifactorial, influenced by patient beliefs, therapy-related barriers, asymptomatic conditions, and social determinants. Stigma, concerns about treatment efficacy, financial difficulties, and medication access further exacerbate the issue. A study conducted in Bangalore by Thomas D et al. [12] highlighted these barriers, reporting that 39.14% of patients were non-adherent due to specific beliefs about their treatment, 78.62% cited financial difficulties in affording medication, and 54.93% faced challenges in obtaining refills.
Measuring adherence is critical for understanding these challenges and designing effective interventions. While objective adherence measures (e.g., pill counts, electronic monitoring, biochemical tests) provide accuracy, they are resource-intensive [16–18]. Subjective measures, such as self-reports and healthcare assessments, are cost-effective, non-intrusive, and capture patient concerns, though they may be influenced by biases [19]. Selecting the appropriate adherence scale requires evaluating its development process, psychometric properties, and contextual applicability.
This scoping review aims to synthesize evidence on medication adherence scales used for major NCDs, specifically Type 2 Diabetes Mellitus (T2DM), Hypertension (HTN), Coronary Artery Disease (CAD), and Bronchial Asthma (BA)/Chronic Obstructive Pulmonary Disease (COPD). These conditions were chosen based on their high global prevalence [20], significant burden of nonadherence [10] and the distinct adherence challenges they pose—ranging from asymptomatic progression (HTN) to symptom-driven adherence patterns (BA/COPD) [21,22]. Additionally, these diseases often require long-term pharmacotherapy, making adherence measurement crucial for optimizing patient outcomes [23].
The global burden of NCDs, particularly in resource-constrained settings, emphasizes the need for culturally and contextually relevant tools. A detailed analysis of existing scales is necessary to identify their strengths, limitations, and gaps, enabling the development of robust, evidence-based tools that support tailored interventions and improve health outcomes while reducing healthcare costs. This would be done by considering their psychometric characteristics, including delineation of quality benchmarks such as sensitivity, specificity, convergent validity, and reliability metrics, along with the development process and the context of testing these scales.
By evaluating their strengths and limitations, this review aims to inform the selection and adaptation of adherence measurement tools, ultimately guiding the development of evidence-based interventions to improve adherence and health outcomes.
Materials and methods
We prepared a study protocol and predefined the data sources, search strategy, study eligibility criteria, data extraction and criteria for quality assessment of the studies. This review was conducted following the Joanna Briggs Institute (JBI) methodology [14,24]. The reporting of the scoping review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) (S3 Text) [25] and the protocol (S4 Text) was registered with Open Science Framework (OSF) (https://doi.org/10.17605/OSF.IO/VNMGH).
Concept
The review considered the studies on the development and validation of all globally available medication adherence scales in selected NCDs (T2DM, HTN, COPD/ BA, CAD) to synthesize evidence using systematic search strategies, quality assessment, and data charting.
Context
This scoping review considered medication adherence scales developed, validated and evaluated in the context of selected NCDs (T2DM, HTN, COPD/ BA, CAD) in community and hospital settings.
Eligibility criteria/Inclusion criteria
English-language studies on the development or validation of adherence scales for adults with T2DM, HTN, COPD/BA, or CAD, published from January 1950 to June 2024, were included. Studies from 1950 onwards were included to ensure a comprehensive review of medication adherence assessment. While standardized adherence scales were developed later, earlier literature contributed to the conceptual understanding of adherence, influencing the design and validation of later tools.
The quality assessment of the included studies was conducted using the JBI critical appraisal criteria [14] (Table B, S1 Appendix) to ensure methodological rigor. As no predefined scoring system exists, we developed one based on expert judgment and established methodological frameworks (Table C, S1 Appendix). Although critical appraisal is optional in scoping reviews, we incorporated it to strengthen the synthesis rather than as an exclusion criterion [26]. All included studies were deemed to be of high quality.
For cohort studies, the parameters were (a) eligibility criteria (defined or not), (b) source of cohort (specified or not), (c) methods of selection and (d) methods of follow up. The maximum score possible was 4 and the minimum was 0. The parameters for quality criteria for case–control studies were (a) eligibility criteria (defined or not), (b) sources (methods of case ascertainment and control selection) and (c) rationale for the choice of cases and controls. The quality criteria for cross-sectional studies were (a) eligibility criteria, (b) sources and (c) methods of selection. The maximum score for case–control and cross-sectional study was 3 and the minimum was 0.
Studies that were not in English, focused on non-adult populations, addressed conditions outside the selected NCDs (T2DM, HTN, COPD/BA, or CAD) or did not involve the development or validation of adherence scales were excluded.
Data sources
This scoping review considered quantitative studies, mixed methods studies, and systematic and scoping reviews. To ensure that no validated scales were overlooked, we initially considered SRs to identify any potentially unique scales discussed within them. Quantitative designs include any experimental study designs (e.g., randomized controlled trials, non-randomized controlled trials, or other quasi-experimental studies, including before and after studies), and observational designs (e.g., descriptive, cohort, and cross-sectional studies). Mixed methods include quantitative and qualitative designs used to validate medication adherence scales.
Search strategy
A detailed search of MEDLINE (PubMed), Embase and Embase Classic, Scopus, Cochrane CENTRAL Register of Clinical Trials, and APA PsycINFO was conducted (Table A in S1 Appendix). The search for unpublished studies was carried out in GreyNet, OpenGrey, and Shodhganga. The reference list of included articles was also searched.
Study selection/Screening
Development, validation and translational studies of medication adherence scales in the context of select NCDs (T2DM, HTN, COPD/ BA, CAD), published in peer-reviewed journals were included in this review. Two independent reviewers (STS and PR) systematically searched the literature using the prespecified strategy and scrutinized the titles and abstracts against the inclusion criteria for the scoping review. Full text of screened-in studies were obtained. Any disagreement between the two reviewers was confirmed by consulting a third reviewer.(JT) We eliminated duplicates using the Zotero Software version 12 (Thomson Reuters, New York). Critical appraisal of the screened-in articles was done using JBI critical appraisal scales.(STS and MJ)
Data charting
The ‘descriptive-analytical’ method within the narrative tradition was utilized in data charting following the scoping review methodology established by JBI methodology for scoping reviews [24]. Two reviewers independently screened each study and independently mapped the studies (STS and PR) using the data extraction form, and any discrepancy between the reviewers was resolved by a third reviewer.(JT) The following data were extracted under different categories (S2 Dataset): 1)Study characteristics: author, year of publication, country, type of study, study setting, and sample size (Table 1). 2) Details of participants and scales: population, disease, Self-report scale, cut-off score, medication, age, gender, and percentage of non-adherence. 3) Psychometric properties of development and translational studies (Table 2 and Table E in S1 Appendix). 4) Medication adherence assessment scale comparison from development and translational validation studies: scale developed based on, number of questions, time to complete, and how scale administered (Table 3).
Table 1: Study characteristics.
Table 2: Psychometric properties of scales with the methods and standards from developmental studies.
Table 3: Medication adherence assessment scale comparison.
The psychometric properties of the included scales were extracted based on key measurement attributes, including reliability (internal consistency, test-retest reliability), validity (content, construct, criterion), sensitivity, specificity, and response rate. These details were derived from the original development and validation studies of each scale. While no single framework was explicitly followed, our approach aligns with established principles of psychometric evaluation [27] to provide a comprehensive synthesis of scale properties. The extracted information is presented in Table 2 and S5 Dataset.
Two different investigators (MJ and PR) verified the data independently for accuracy after extraction. Discrepancy was resolved by discussion with a third investigator (JT). Missing data were addressed systematically by contacting corresponding authors and investigators for full texts and missing data, but no responses were received. Therefore, we included studies that validated medication adherence tools with psychometric properties for analysis. We employed an available data analysis approach, assuming data were missing at random, ensuring reliable and robust results.
Data synthesis
The data from the included studies were compiled as a descriptive summary. The findings were presented in the form of summary tables based on an initial overview of the general characteristics of the included studies and scales, followed by psychometric properties of scales, and a comparison of medication adherence assessment scales from development and translational validation studies.
Ethics and dissemination
An ethics review was not required, as only publicly available data was analyzed. Findings from the scoping review will be published in a peer-reviewed journal and disseminated to health professionals and policymakers involved in NCD care.
Results
Study selection
A total of 12108 records were initially identified, which consisted of 6238 articles after removing duplicates. Title and abstract screening excluded 6075 articles, leaving 163 for full-text review (Fig 1: PRISMA flow diagram). A further 23 articles [15,28–42] were excluded for various reasons listed in Table D in S1 Appendix. Ultimately, 140 studies met the inclusion criteria for this review [43–182].
PRISMA flow diagram.
All included studies were appraised using the JBI critical appraisal scales to ensure methodological rigor. Based on established conventions and guidelines [24], cross-sectional studies with scores ≥4 and RCTs with scores ≥6 were considered to be of ‘good quality’ for inclusion. These thresholds were chosen as they represent the minimum level of methodological integrity needed to provide reasonably reliable evidence.
The appraisal revealed that, among cross-sectional studies, 120 scored between 4 and 6 [43–162], while 17 scored between 7 and 8 [163–179]. All three RCTs scored between 8 and 9 (Table B in S1 Appendix) [180–182]. While all included studies met our definition of ‘good quality,’ we acknowledge that there was still some heterogeneity within this range. However, we did not find any significant differences in our review’s overall findings based on whether studies had scores at the higher or lower end of our ‘good quality’ range.
Given that all included studies met our pre-defined quality thresholds, we believe this strengthens the reliability and robustness of our findings. The consistent application of sound methodologies across studies provided a solid foundation for our synthesis and supported the rigor with which we drew our conclusions.
Study characteristics
A total of 140 studies [43–182], published between January 1950 and June 2024, were analyzed. Among these, 131 studies (93.6%) assessed a single self-report scale [43–51,53–67,70–75,77–91,93–143,145–156,158–165,167–175,177–182], while 9 studies (6.4%) utilized more than one scale [52,68,69,76,92,144,157,166,176]. The sample size ranged from 26 [95] to 6237 [143] with a median of 174.5 participants. Across these studies, fifty-seven individual self-reported adherence scales were identified, with adherence cutoff scores varying from 1 [146] to 87 [150] and non-adherence rates ranging from 0.6% [176] to 89.4% [127].
The most frequently studied scale was the MMAS-8 (n=24, 17.14%) [51,56,59,60,64,69,76,78,81,84,90,97,99,103,106,109,121,126,132,135,168,174,177], followed by the BMQ (n=13, 9.2%) [46,52,54,58,86,88,120,124,133,134,155,157,166], GMAS (n=11, 7.9%) [82,83,101,102,115–118,130,148,175], MMAS-4 (n=9, 6.4%) [92,94,108,112,143–145,166,178], MARS (n=9, 6.4%) [49,52,67,98,105,111,136,138,144] and ARMS (n=7, 5%) [53,77,91,93,107,152,181]. For all the scales, both developmental and translational validation studies were considered. However, the developmental study for the MMAS-8 [183] was excluded from data extraction because it has been retracted.
The MMAS-8 was primarily studied in patients with T2DM (n=12) [51,56,59,69,81,99,103,106,126,135,177] and HTN (n=11) [56,64,76,78,90,97,109,121,132,168,174]. Meanwhile, the GMAS was predominantly used in chronic diseases (n=7) [83,115–117,130,148,175] involving more than 1 select NCD. The detailed study characteristics are summarized in Table 1.
Psychometric properties of scales with the methods and standards from developmental studies (Table 2)
The scales were developed through a combination of qualitative methodologies (n=4,10.8%) [47,146,147,182], including focus group discussions, semi-structured interviews with patients and experts, as well as an extensive literature review (n=13,35%) [66,67,71,73,85,89,110,112,140,162,165,167,183]. Additionally, mixed methods were employed (n=17,45.95%) in the development process [46,48,61,79,93,114,115,122,123,142,153,154,156,158,161,164].
Response rates were documented in 17 studies (45.95%) [46–48,61,66,67,71,85,110,115,140,146,158,161,162,164,182], ranging from 50.2% [66] to 100% [67]. Sensitivity of scales was assessed in 11 studies (28.9%) [74,79,110,112,114,115,122,146,165,167,169], while specificity was evaluated in 10 studies (26.3%) [74,79,110,112,114,122,146,165,167,169]. Five scales demonstrated high sensitivity [74,110,112,114,167], and one scale exhibited high specificity (80–100%) [114], indicating their efficacy in accurately measuring medication adherence and medication non-adherence. Feasibility was not reported for any of the scales. Heterogeneity in psychometric properties refers to the significant inconsistency in measurement characteristics of a tool (reliability, validity, sensitivity, and specificity) across different medication adherence scales or when the same scale is used in different settings.
Reliability.
Cronbach’s alpha was reported by 34 studies (89.5%) [46–48,57,61,65–67,71,74,79,85,89,93,110,112,114,115,122,123,140,142,147,153,154,156,158,161,164,165,179,181,182], with 30 studies demonstrating an acceptable range exceeding 0.7, indicating an excellent level of internal consistency [46–48,57,61,66,67,71,79,85,89,93,110,114,115,122,123,140,142,147,153,154,156,158,161,164,179,181,182]. Test-retest reliability, indicating the stability of measurements over time, was reported using Pearson’s or Spearman’s correlation coefficient. Three scales demonstrated high reliability (>0.90) [57,67,115], one scale exhibited moderate reliability (0.8–0.9) [110], and nine scales showed insufficient reliability (<0.8) [66,74,79,85,93,114,123,142,165]. Other reliability measures are summarized in Table 2.
Validity.
Ten scales (26.3%) [61,67,74,110,112,122,123,156,179,182] were assessed for their correlation with an objective measure of adherence, with one scale evaluated using MEMS [182], while the others were compared against clinical outcomes such as blood pressure [61,67,112,156] and HbA1c levels [74,110,179]. Criterion-related validity was examined for 56.8% (n=21/37) of the scales [46,47,61,67,71,74,85,93,110,112,114,115,122,123,153,154,156,158,165,167,179], revealing significant correlations with various measures including clinical outcomes [61,67,74,110,112,123,156,179], electronic adherence measurements [122,182], subscales of the current scale [46,93,115,154], and other self-report scales [47,61,65–67,74,79,85,93,110,114,122,123,142,146,153,158,164,167,169,182]. Construct validity, a pivotal aspect that assess whether a scale accurately measures the theoretical construct, it is intended to evaluate- which was undertaken for 73% (n=27) of the scales [46–48,61,65–67,74,79,89,110,112,114,115,122,140,142,146,153,154,158,161,164,165,181,182].
On reviewing psychometric properties of translational studies, 6 scales showed high sensitivity [49,100,109,113,116,133], while 11 demonstrated high specificity (80–100%) [56,76,80,113,116,133,137,143,144,150,152]. Sixty six studies (47.14%) reported good internal consistency with Cronbach’s alpha >0.7 [45,49,52–56,58,59,62,63,68–70,75,77,78,80–82,86–88,91,92,95–97,99,101,102,104,107,111,113,116–120,124,125,127–132,134,137–139,148,149,151,152,155,157,159,160,163,166,171,173,175,180], whereas only 3 studies demonstrated high reliability (>0.90) [102,109,128]. Seventy-four studies (52.9%) utilized a correlation with a comparative measure. The response rates in these studies varied between 24.7% [150] and 99% [96]. Among these, 37 studies (26.4%) compared adherence against objective measures such as pill count, the MedSignals pillbox, and HbA1c levels, while the remaining studies were against self-report questionnaires. Other measures are summarized in Table E in S1 Appendix.
Medication adherence assessment scale comparison
Out of the 140 studies in total, 37 focused specifically on the development of scales [46–48,57,61,65–67,71,74,79,85,89,93,110,112,114,115,122,123,140,142,146,147,153,154,156,158,161,162,164,165,167,169,179,181,182], whereas 103 (73.6%) were primarily concerned with translating the original scales and then validating them in different settings or languages [43–45,49–56,58–60,62–64,68–70,72,73,75–78,80–84,86–88,90–92,94–109,111,113,116–121,124–139,141,143–145,148–152,155,157,159,160,163,166,168,170–178,180].
The number of questions in these scales varied from 4 [112] to 30 [46] questions, with a median count of 11 questions. The time taken to complete answering the scales varied from 1 minute [137] to approximately 40 minutes [132], with a median duration of 5.53 minutes. A scale of 13 questions took a minimum of 1–3 minutes [114], while 40 minutes were required to answer the scale with 8 questions [132]. Regarding adherence, 22 scales specified a cut-off score, with the reported range varying from 0–1 [146] to 87 [150]. Implementation and discontinuation stages of medication taking were considered in 8 scales [48,49,67,93,112,142,160,181], whereas, only the implementation stage was considered in 8 scales [45,48,70,79,87,89,180,182].
Self-efficacy has been found to be a crucial predictor of adherence, with 9 scales reported for its assessment [46,65,70,89,123,156,161,162,169]. Notably, SEAMS [123], TSQM [161], and MASES [156] were specifically developed to integrate self-efficacy into the measurement of adherence. The majority of the scales, 59.6%, were self-administered, while researcher-administered scales, conducted in consultation with patients, followed closely at 17.5%. Only 22.8% of scales were administered by both methods. Only Twenty-eight scales (49%) were validated for patients with low literacy [44,51,52,57,61,69–71,74,79,87,93,108,110,115,122,124,129,139,140,146,147,150,158,163,165,167], making them suitable for use across all literacy levels (Table 3).
Forty-two (73.7%) self-report scales were developed to assess medication adherence among multiple conditions [44–48,51,61,65–71,74,76,79,85,93,111,112,115,123,128,131,140,142,146,150,156–158,160–163,167,169,171,176,180], whereas 15 (26.3%) were tailored to specific conditions [43,57,62,69,72,75,110,113,114,137,147,154,164,165,182]. These scales evaluated adherence to particular medications such as antihypertensives [89] or inhalers [147]. Some either created new tools, like the Diabetes Medication Adherence Scale (DMAS) [165] or adopted established validated measures, like the Hill-Bone Medication Adherence scale (HBMA) [131].
Among these, 4 scales were designed for assessing medication adherence in HTN [62,75,89,182]. with the HBCTS [89] being the most commonly utilized. For T2DM, 4 scales were identified [57,69,110,165], while 3 were tailored for BA [114,154,164], and 4 others focused on inhalational medicines [43,113,137,147] applicable to both BA and COPD. Conversely, non-condition-specific measures evaluated adherence more broadly [44–48,51,61,65–71,74,76,79,85,93,111,112,115,123,128,131,140,142,146,150,156–158,160–163,167,169,171,176,180], with most studies employing pre-existing validated questionnaires, such as MMAS-8 and ARMS.
Domains and gaps of existing scales
Among the 57 individual medication adherence assessment scales identified, most of the scales evaluated medication-taking behavior, while only a few did not assess this domain [43,46,70,123,154,156–158,161,162]. The BMQ [46], HBM-based questionnaire [157], and ITBQ [43] concentrate on beliefs, concerns, and perceptions. Whereas, the TSQM [161], SATMED-Q [158], and PSAM [154] focus on domains such as convenience, satisfaction, and effectiveness. SEAMS [123] and MASES [156] address patients’ self-efficacy, motivation, and confidence.
Although some scales, like the GMAS [115], LMAS [167], MAR-Scale [142], and DMAS [165], consider the cost factor, they do not adequately address the out-of-pocket expenditure, which is an important area of health economics especially in developing countries where most patients pay direct medical costs which is a crucial aspect of health economics in developing countries where most patients bear direct medical costs.
The best known and most widely used is the Morisky Scale developed from the 4-item MMAS-4 [112] to the 8-item MMAS-8 [183]. The scale identifies barriers such as forgetfulness and adverse effects and fails to capture cost-related non-adherence (CRNA), self-efficacy, and health care system-related factors. In addition, there is overlap between the questions which could result in scoring ambiguity.
The MARS [49] explores beliefs and barriers to medication-taking behavior. It includes ten questions that assess adherence behavior and disease control over the past week and used for patients with chronic mental illness. The major limitations were the scale not validated in low literacy patients and did not assess self-efficacy.
The ARMS [93], evaluates taking medications as prescribed and refilling medications on schedule. Cost factor and out of pocket expenditure, and patient self-efficacy dimensions of medication adherence were not considered in this scale. Additionally, sensitivity, specificity of ARMS are not reported and compared to clinical outcomes. We do not find any studies that have validated ARMS in the Indian setting.
The SEAMS [123] and the BMQ [46] have three main question headings and multiple sub questions. Both assess self-efficacy, barriers and are validated in patients with low literacy. However, the sensitivity and specificity of SEAMS is not estimated, and it lacks the ability to rapidly estimate adherence at point of care/bedside. Additional information on the domains and gaps of scales are provided in Table 4.
Table 4: Domains and gaps of medication adherence assessment scales.
Discussion
This scoping review synthesizes evidence on medication adherence scales for NCDs, identifying critical gaps in their design, validation, and applicability. While many scales, such as MMAS, GMAS, and BMQ, are widely used, they often fail to capture the multifaceted nature of adherence, particularly in populations with low literacy and multimorbidity. Developing countries facing an epidemiological transition are witnessing a rising burden of multiple NCDs. Given the prevalence of comorbidities among patients managing multiple medications, an adherence scale tailored for multiple NCDs is essential for accurate evaluation and targeted interventions
Most existing tools focus on self-reported adherence, which is prone to recall and social desirability biases, reducing their reliability in real-world settings [67,112]. Integrating objective methods such as electronic pill monitoring or biochemical markers alongside self-reports can mitigate these challenges.
A major limitation in current adherence measurement is the lack of consideration for socioeconomic and cultural factors. Many scales focus predominantly on behavioral adherence while neglecting critical influences such as financial constraints, access to medications, cultural beliefs, and healthcare system challenges, which are particularly significant in low- and middle-income countries (LMICs). These challenges shape patients’ perceptions of medication necessity and efficacy [184]. Economic factors, including out-of-pocket expenditures and access to healthcare services, play a significant role in medication adherence, especially in developing countries like India [185]. Indirect healthcare costs, including transportation expenses, can lead to missed clinic appointments and reduced access to pharmacies [186,187]. Overlooking these aspects may lead to inaccurate adherence assessments and ineffective interventions [188]. The inclusion of constructs related to financial burden, treatment-related stress, and patient-provider communication could improve the contextual relevance of adherence assessments in LMICs [189,190].
Without robust cross-cultural validation, existing adherence scales may not generalize to diverse healthcare settings, increasing the risk of measurement bias and limiting their utility in resource-limited contexts. Tools like the GMAS require broader adaptation to enhance their relevance beyond specific regional settings. Additionally, validating these scales across different healthcare contexts ensures their generalizability beyond hospital-based and urban cohorts [22]. Expanding their application can enhance real-world usability and increase their adoption in healthcare systems with varied socioeconomic backgrounds.
From a clinical perspective, adherence scales should incorporate factors such as patient engagement, shared decision-making, and trust in healthcare providers, as these elements significantly impact medication-taking behavior [62]. As evidenced in a study by Gellad W F et al. [7], hypertensive patients who discussed their condition with their physician were significantly more likely to be adherent to their blood pressure medication.
Despite their critical role in adherence, current scales lack structured assessments of trust and shared decision-making [191], limiting their applicability in patient-centered care. Incorporating these dimensions into adherence assessment tools could improve their predictive validity and real-world applicability. In addition, the use of patient-centered communication strategies, such as motivational interviewing, has shown promise in improving adherence and should be explored in future scale development [192].
Psychosocial factors, including stress and mental health conditions, significantly influence medication adherence. A study by Kretchy I A et al. [193] found that individuals experiencing stress were significantly more likely to exhibit nonadherence compared to those with low or no stress levels. Patients displaying stress symptoms might be more vulnerable to the adverse effects of their medications, often leading to discontinuation [193]. The psychological dimensions of medication adherence have been considered in the Lebanese Medication Adherence Scale [167]. However, these psychological factors were not incorporated into most other scales we reviewed. Evolving medication adherence scales should explicitly integrate these dimensions to ensure a comprehensive and accurate assessment. Emerging evidence also suggests that integrating patient-reported outcome measures (PROMs) related to mental health into adherence scales can improve predictive validity [194].
Methodologically, the use of qualitative inputs from patients and experts during item development, as seen in SEAMS and GMAS, can guide the creation of more nuanced tools. The exploratory sequential mixed-method approach, involving qualitative and quantitative components, is widely recognized for scale construct development and validation [195]. While internal consistency is frequently reported (e.g., Cronbach’s alpha > 0.7 for most scales), fewer studies assess test-retest reliability or sensitivity and specificity. Analysis of the psychometric properties of various scales revealed significant variability in sensitivity, specificity, reliability, and validity across different settings. For instance, the MMAS-8 showed varying sensitivity across different studies [51,56,59,76,126], which may not be universally applicable. Future scale development must employ robust psychometric analyses to ensure temporal stability and diagnostic accuracy. Scales such as the MMAS-4 and BMQ have shown effectiveness but require contextual validation in low-literacy populations and under-resourced healthcare settings. Developing pictorial or voice-assisted tools could improve accessibility and usability in these populations.
Current scales, like MMAS-8, predominantly assess implementation. A meta-analysis by DiMatteo et al. reported that about 24% of patients discontinue their medication prematurely, which can significantly impact treatment outcomes [196]. Future tools should evaluate all stages of adherence—initiation, implementation, and discontinuation—to provide a comprehensive understanding of medication-taking behaviors. Given the limitations of self-reported adherence, integrating digital health solutions—such as mobile-based adherence interventions and electronic monitoring—can provide real-time insights and reduce recall bias. These technologies can complement traditional adherence scales, enhancing both measurement accuracy and patient engagement [197].
Bridging these gaps through participatory research and rigorous validation will yield adherence assessment tools that are not only reliable and inclusive but also aligned with real-world patient needs. Strengthening adherence measurement methodologies will not only improve clinical outcomes but also optimize healthcare resource utilization globally.
This review was limited to English-language studies for feasibility reasons, which may have led to the exclusion of relevant adherence scales published in other languages. This linguistic restriction is a methodological limitation, potentially impacting the comprehensiveness of our findings, particularly in non-English-speaking regions.
Conclusion
In conclusion, this scoping review emphasizes the complexity of measuring medication adherence for NCDs through scales like MMAS-8, GMAS, and BMQ. While these tools are valuable, they fail to capture key factors such as socio-economic, cultural influences, and multimorbidity—especially in low-literacy populations. Most scales address only parts of the medication-taking process and lack rigorous psychometric validation using objective measures like Medication Event Monitoring System (MEMS). In light of these findings, it is clear that the existing adherence scales should not only be revised but also rethought to address the evolving challenges in patient care. These updated scales must be developed using a comprehensive, evidence-based approach, considering the dynamic nature of patient behaviors and the complex context in which they exist.
Future scale development should focus on creating context-specific, culturally sensitive tools that assess adherence in patients with multiple NCDs. These tools should incorporate factors such as patient trust, stress, and beliefs and employ a robust methodological framework with advanced algorithms which can improve the predictive power and reliability of these tools. Such improvements could ultimately lead to more precise adherence measurement and better patient outcomes, enhancing both clinical practice and research efforts.
Supporting information
S1 AppendixSearch Strategy, Critical appraisal of articles, Scoring developed for JBI critical appraisal checklist, List of excluded studies and reasons for exclusion and Psychometric properties of translational studies of scales.(PDF)
S2 DatasetData charting excel and data extracted from studies.(XLSX)
S3 TextPRISMA-ScR-Checklist.(DOCX)
S4 TextScoping review protocol.(PDF)
S5 DatasetStudy screening and selection process.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burkhart PV, SabatéE. Adherence to long-term therapies: evidence for action. J Nurs Scholarsh. 2003;35(3):207. doi: 10.1111/j.1547-5069.2003.tb 00001.x 14562485 · doi ↗ · pubmed ↗
- 2Non communicable diseases. [2023 Dec 13]. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases
- 3Omotayo O, Maduka CP, Muonde M, Olorunsogo TO, Ogugua JO. The rise of non-communicable diseases: A global health review of challenges and prevention strategies. Int Med Sci Res J. 2024;4(1):74–88.
- 4Miranda SAD, Aguilar RR. Related factors with NCD in developing countries: Economic, diet and risk factors dimensions. EAI Endorsed Transactions on Pervasive Health Technologies. 2024 [2024 Dec 9];10. Available from: https://publications.eai.eu/index.php/phat/article/view/3499
- 5Jin J, Sklar GE, Oh VMS, Li SC. Factors affecting therapeutic compliance: A review from the patient’s perspective. Ther Clin Risk Manag. 2008;4(1):269–86.18728716 10.2147/tcrm.s 1458 PMC 2503662 · doi ↗ · pubmed ↗
- 6Bosworth HB, Granger BB, Mendys P, Brindis R, Burkholder R, Czajkowski SM, et al. Medication adherence: A call for action. Am Heart J. 2011;162(3):412–24. doi: 10.1016/j.ahj.2011.06.007 21884856 PMC 3947508 · doi ↗ · pubmed ↗
- 7Gellad WF, Grenard JL, Marcum ZA. A systematic review of barriers to medication adherence in the elderly: Looking beyond cost and regimen complexity. Am J Geriatr Pharmacother. 2011;9(1):11–23. doi: 10.1016/j.amjopharm.2011.02.004 21459305 PMC 3084587 · doi ↗ · pubmed ↗
- 8Currie CJ, Peyrot M, Morgan CL, Poole CD, Jenkins-Jones S, Rubin RR, et al. The impact of treatment noncompliance on mortality in people with type 2 diabetes. Diabetes Care. 2012;35(6):1279–84. doi: 10.2337/dc 11-1277 22511257 PMC 3357221 · doi ↗ · pubmed ↗