The differential burden of acute rhinovirus infections in children with underlying conditions
María Isabel Sánchez Códez, Isabel Benavente Fernández, Katherine Moyer, Amy L. Leber, Octavio Ramilo, Asuncion Mejias, Kevin Looi, Tai-Heng Chen, Tai-Heng Chen, Tai-Heng Chen

TL;DR
This study shows that children with certain health conditions, like asthma or heart disease, are more likely to have severe outcomes from rhinovirus infections.
Contribution
The study identifies specific comorbidities and factors associated with severe rhinovirus disease in children.
Findings
Asthma/atopy, prematurity, and congenital heart disease are consistently linked to severe rhinovirus outcomes.
Higher viral loads and bacterial co-infections are associated with worse clinical outcomes.
The prevalence of comorbidities increases with age in children with rhinovirus infections.
Abstract
Rhinoviruses (RVs) are a well-known trigger of wheezing episodes in children with asthma. Their role in other pediatric chronic medical conditions is not fully known. Patients ≤21 years hospitalized or evaluated as outpatients with symptomatic RV infection were identified from 2011–2013. Patients were categorized based on the type of underlying disease and differences in clinical parameters, RV loads (CT values), viral, bacterial and fungal co-infections and clinical outcomes were compared between groups. Multivariable analyses were performed to identify the comorbidities associated with oxygen requirement, PICU admission, and prolonged hospitalization. Of 1,899 children identified, 77.7% (n = 1477) had an underlying comorbidity including asthma/atopy (36.8%), prematurity (7.7%), chronic respiratory diseases (6.4%), congenital heart disease (CHD, 3.2%), immunocompromised hosts (ICH;…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
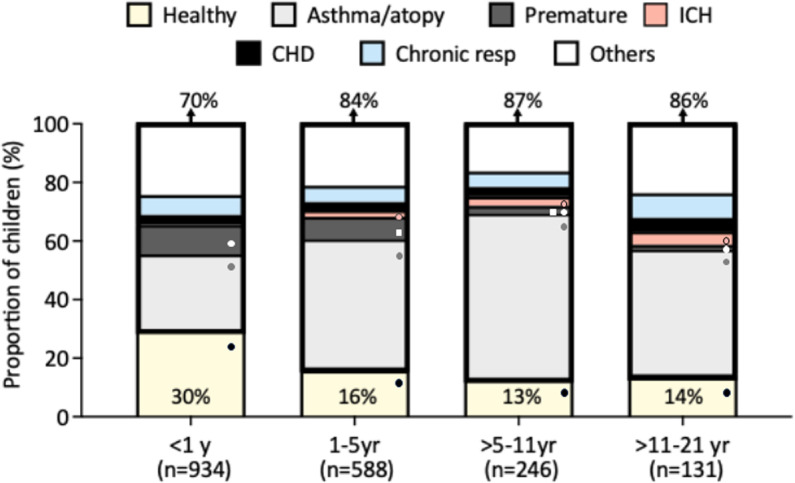 Fig 1
Fig 1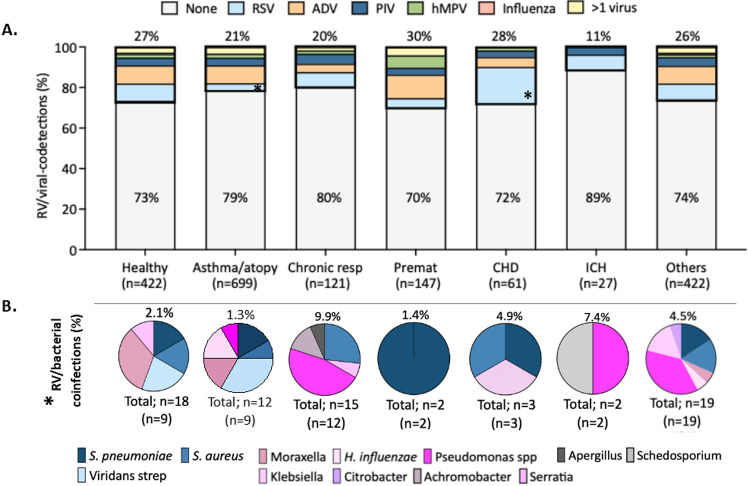 Fig 2
Fig 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory viral infections research · Asthma and respiratory diseases · Respiratory and Cough-Related Research
Introduction
Rhinoviruses (RVs) are a leading cause of upper and lower respiratory tract infections (LRTI) in children and adults [1,2]. The causative role of RVs in respiratory diseases has been underestimated as they are commonly detected in asymptomatic subjects and associated with prolonged shedding [3–6]. Nonetheless, RVs have been recognized as important triggers of wheezing episodes in asthmatic children [7]. In addition to asthma, pediatric studies suggest that certain underlying conditions, such as immunocompromised hosts (ICH), prematurity, or congenital heart disease (CHD), have an increased risk for severe RV infections (ARI) [1,8–11]. Whether the increased risk for severe RV disease extends to children with other comorbidities, and whether specific clinical parameters or co-detection with other pathogens are associated with increased morbidity is not fully known.
The aim of the present study was to define the clinical phenotype and the differences in clinical presentation, healthcare utilization and the impact of RV loads and of co-infections in a large cohort of pediatric patients with RVs infection according to the type of underlying condition.
Materials and methods
Patient population and study design
This was a retrospective study including a convenience sample of children and adolescents ≤21 years of age with symptomatic RVs infection diagnosed in the inpatient setting or as outpatients from 7/2011–12/2013. We included patients up to 21 years of age since this was the catchment population that is cared for at Nationwide Children’s Hospital (NCH), a common practice in US pediatric hospitals [12]. Children and adolescents were identified by virology reports, clinical was data extracted from electronic healthcare records (EHR), and manually reviewed by two independent investigators. Children with incomplete data and non-respiratory diagnoses were excluded. To ensure that the episodes analyzed were distinct, duplicate encounters during the same calendar year were also excluded, as RV can be shed for months after the acute episode. The present study involves the analysis of a subset of children as part of a larger cohort that has been previously published [13].
RV testing was performed per standard of care in respiratory samples using a RV rt-PCR targeting the 5´NCR (or 5´UTR) region as described [14,15]. RV molecular typing was not performed. Semiquantitative RV viral loads were reported as cycle threshold (C_T_) values, with a C_T_ value > 40 being considered not detected. RV testing was run in parallel with individual PCRs for respiratory syncytial virus (RSV), parainfluenza virus (PIV), influenza virus A/B, adenovirus (ADV), and human metapneumovirus (hMPV) as part of a panel [16]. EHR were assessed for pertinent demographic and clinical data including the admission diagnosis, laboratory and radiologic findings and co-infections. Viral co-detections were defined as the simultaneous detection by PCR of one of the other respiratory viruses included in the panel. Bacterial or fungal co-infections were defined as the isolation of these pathogens by culture from a sterile site (blood, pleural fluid) or the lower respiratory tract. In addition, in symptomatic children with cystic fibrosis (CF), throat culture samples were considered valid for detecting both bacterial and fungal pathogens. We collected information regarding healthcare utilization including medications, need for hospitalization, supplemental oxygen, PICU care and total length of stay. For analysis purposes children were grouped into seven categories based on the type of underlying disease: asthma/atopy; other chronic respiratory conditions including chronic lung disease (CLD) or CF; prematurity without CLD; CHD; ICH; others (i.e., endocrine, renal, etc); and none (previously healthy). Children with more than one comorbidity were included in the disease category that had the greatest impact on RV disease severity based on previous studies [8–11,17], such as that a child with asthma/atopy and renal disease was categorized under asthma/atopy. The hierarchical order used for children with more than one underlying condition was as follows: ICH; asthma/atopy; other chronic respiratory conditions; prematurity without CLD; CHD and others (endocrine, renal, etc).
The study was approved by NCH Institutional Review Board (IRB#13–00796). It was granted exemption from obtaining informed consent due to its retrospective design in accordance with the US Department of Health and Human Services regulations, specifically 45 CFR 46. Data was accessed from EHR over a 11-month period (February 6^th^ through December 19^th^ of 2014), and any identifier linked to participant individuals destroyed upon data collection and curation.
Statistical analysis
Qualitative data were expressed as percentages, and quantitative variables as medians and 25%-75% interquartile range (IQR) as data were not normally distributed. Chi-squared test or Fisher’s exact tests were used to compare proportions, and Kruskal–Wallis tests for continuous data followed by the Holm post-hoc test to adjust for multiple comparisons. In addition, the Bonferroni correction was applied to correct for multiple testing when analyzing families that included multiple parameters such as diagnoses, medications used or underlying conditions. Multivariable logistic regression was performed to define the risk for supplemental oxygen administration, PICU admission and longer length of stay according to the type of comorbidity, adjusted by age, sex, RV loads and viral and bacterial co-infections. For analysis purposes length of stay was dichotomized by the median which was 2.1 days. Two-sided p-values <0.05 were considered statistically significant. Analyses were conducted using STATA 16.0. (StataCorp, College Station, TX, USA).
Results
Demographic and clinical characteristics
Of the 1,899 children with symptomatic RV infection, 77.7% (n = 1,477) had underlying comorbidities. Asthma/atopy was the most prevalent (36.8%; 699) followed by prematurity (7.7%; 147); other chronic respiratory diseases (6.4%; 121); CHD (3.2%; 61); and ICH (1.4%; 27). Chronic respiratory diseases included CF (0.9%; 18), CLD (3.2%; 61), and less common conditions such as tracheoesophageal fistula, pulmonary hypertension, spontaneous pneumothorax, airway malacia, subglottic stenosis, cleft palate, and Pierre-Robin sequence. The remaining children with other comorbidities (22.2%; 422) included genetic syndromes (6.9%; 132), gastrointestinal diseases (3.6%; 68), neurologic disorders (1.9%; 36), hematologic diseases (0.9%; 17), and a variety of other conditions, including endocrine, osteoarticular and genitourinary abnormalities (8.9%; 169) (S1 Table in S1 File).
Median age for children with comorbidities (15.8 [4.9–52.9] months) was greater than for previously healthy (4.7 [1.5–19.9] months, p = 0.0001); Table 1.
Table 1: Demographics, laboratory, radiology parameters and distribution of diagnoses of children and adolescents with RV infection.
ICH were the oldest group (68.6 [42.5–116.3] months). The prevalence of comorbidities increased after the first year of life, when 84% to 87% of children had a chronic medical condition vs 70% in infants (p < 0.0001; Fig 1).
Distribution of underlying conditions according to age.The Y axis depicts the proportion of children and adolescents with RV ARI and the X axis the different age groups, with the number of patients included in each age group underneath the bars. Percentages at the top of the bars indicate the overall proportion of children with underlying conditions for that age group, and those at the bottom the proportion of previously healthy children per age group, that are color-coded in yellow. The different underlying comorbidities are represented as follows: grey (asthma/atopy), dark grey (premature), red (ICH), black (CHD), blue (chronic resp diseases) and white (others). CHD, congenital heart diseases; Chronic resp, other chronic respiratory conditions; ICH, immunocompromised host; yr, years. Analyses by χ2 test. Significant p values <0.05 values are represented by symbols (●, ◼). Matching symbols indicate the groups for which significant differences were identifed.
The prevalence of asthma/atopy doubled in children >1 year (45%-57%) vs infants (26%; p = 0.007). Prematurity was more common in infants and children 1–5 years (10% and 7.6% respectively) than in older children (1.5%-2.5%; p = 0.007). Only 0.2% of infants were ICH vs 4.6% of children 11 to < 21 yr (p = 0.007; S2 Table in S1 File). Upper respiratory infection (URI) was the most common diagnosis in ICH (55.6%) and healthy children (48.3%) while wheezing illnesses predominated in children with asthma/atopy (63.4%) and prematurity (49.7%). Pneumonia was the initial diagnosis in 42.2% of children with chronic respiratory conditions and in 18.5% of healthy children (p = 0001). Fever, acute otitis media or sinusitis represented <4% of the admitting diagnoses.
In terms of laboratory data, 52.4% (995/1899) of children underwent blood work-up. Leukocytosis was more common in asthmatic/atopic children while leukopenia predominated in ICH. Abnormal radiologic findings were reported in 50% of ICH children vs 75%-85% of children with other comorbidities (p = 0.017). The most common radiologic patterns were bronchial wall thickening and atelectasis in 56.0% to 67.2% of children respectively (S3 Table in S1 File).
RV loads and viral and bacterial co-infections
Semiquantitative RV loads (C_T_ values) were similar between healthy (25.6 C_T_ values) and children with comorbidities (25.05 C_T_ values), irrespective of the type of comorbidity (S4 Table in S1 File). A concomitant respiratory virus was identified in 26.5% (112/422) of healthy children and 19.8%-29.9% (347/1477) of those with comorbidities (Fig 2A, S4 Table in S1 File). ADV and RSV followed by PIV were the most common co-detected viruses. RV/ADV co-detection was more common in asthmatic/atopic (8.9%) and premature children (11.6%; p = 0.05), whereas RV/RSV co-detections were more frequent in CHD (18.0%), chronic respiratory conditions (7.4%) and children with other comorbidities (7.8%). In healthy children, rates of RV/ADV or RV/RSV co-detection were comparable and ~ 9%. Co-detection of other respiratory viruses in ICH was rare and identified in only three children (RV/RSV, n = 2; RV/PIV, n = 1). More than one additional respiratory virus was identified in 2.8% (n = 54) of children and the most frequent combination was RV/ADV/RSV in two-third of cases.
RV/viral co-detections and RV/bacterial/fungal co-infections in children and adolescents with RV infections.(A) Bars represent the proportion of viral co-detections in children with RV infection in the different disease groups (healthy, asthma/atopy, chronic respiratory diseases, prematurity, CHD, ICH and others). The proportion of RV-single infections are depicted inside the bars colored in grey, and the percentages of RV/viral co-detections are above each bar. RV/RSV is color coded in blue, RV/ADV in orange, RV/PIV in dark blue, RV/hPMV in green and RV/ > 1 respiratory virus in yellow. Analyses by χ2 test. The asterisk indicates the two groups that were significantly different showing that children with CHD had significantly higher rates of RSV infection than those with asthma/atopy (p < 0.01). (B) Pie charts represent the proportion of the different microorganisms isolated in each group with the total percentage of bacterial/fungal co-infections identified include above each pie chart. The total number of pathogens identified is depicted underneath the pies along with the number of patients (in parenthesis). Pink and blue colors indicate gram-negative and gram-positive bacteria respectively. Grey color indicates fungal pathogen. Analyses by χ2 test. For bacterial co-infections significant differences were identified between children with chronic respiratory conditions vs. all the type of comorbidities except CHD and others (p < 0.05). RV, rhinovirus, RSV, respiratory syncytial virus, ADV, adenovirus; hMPV, human metapneumovirus; PIV, parainfluenza virus; CHD, congenital heart diseases; ICH, immunocompromised host; Premat, premature; resp, respiratory.
Bacterial co-infections were identified in 56 (2.9%) children based on lower respiratory/BAL cultures (n = 48), throat cultures from patients with CF (n = 4), or blood cultures (n = 4) and were more common in children with chronic respiratory conditions (9.9%) and ICH (7.4%); p = 0.001; (S4 Table in S1 File, Fig 2B). The most common bacteria identified were S. pneumoniae, S. aureus and P. aeruginosa. The proportion of gram-positive bacteria was greater in asthmatic/atopy children (58.3%) while gram-negative bacteria were mor commonly cultured in children with chronic respiratory conditions (71.4%). Differences did not reach statistical significance.
Healthcare utilization in children with RV ARI
We assessed the use of medications and other indicators of healthcare utilization (Table 2).
Table 2: Healthcare utilization in children and adolescents with RV infection.
Systemic steroids were used more commonly in children with asthma/atopy, chronic respiratory conditions and prematurity (41.5–62.4%) than in healthy children (20.7%; p = 0.0001). Bronchodilators including albuterol, ipratropium bromide or magnesium sulfate, were administered to ~ 75% of children with asthma/atopy and other chronic respiratory diseases and in 14.8% of ICH, with no differences between groups (p > 0.05). Antibiotics were administered to ~ 40% of children, and their use was significantly higher in ICH (67%; p < 0.001).
Overall, 86% of children with comorbidities were hospitalized vs 77% of previously healthy (p = 0.0001). The number of children who required supplemental oxygen was also higher in children with comorbidities (p < 0.001). This difference was mainly driven by children with asthma/atopy (65.2%), CHD (65.6%) and other chronic respiratory diseases (65.3%) vs healthy (35%) or ICH (18.5%). PICU admission was higher in children with comorbidities (34%) vs healthy (17%) or ICH (11%); p = 0.0001. This difference was also driven by children with asthma/atopy and CHD. Children with chronic respiratory diseases, CHD, prematurity or other underlying diseases required mechanical ventilation more commonly (11%-16%) than children with asthma/atopy, ICH or those previously healthy (<5%). Total length of stay was shorter for healthy children than those with comorbidities (1.7 vs 2.4 days; p = 0.0001).
Mortality and predictors of clinical outcomes
Thirty children died, all but two had major comorbidities including asthma/atopy (n = 7), ICH (n = 4), CHD (n = 2), chronic respiratory conditions (CLD; n = 1), prematurity (n = 1) and other comorbidities (genetic syndromes, n = 11; neuromuscular diseases, n = 1; central diabetes insipidus, n = 1). Most of these children (63.3%; 19/30) had high RV loads (≤25 C_T_), intermediate (26–32 C_T_) in 23.3% (7/30), and low (>32 C_T_) in 4 (13.3%) children. A concomitant viral (n = 6), bacterial (n = 5) or fungal (n = 1) co-infection was identified in 12 (40%) children. The per patient underlying condition, age, RV loads (ct values) and specific co-infection is included in S5 Table in S1 File.
Last, we performed multivariable analyses to define which comorbidities, adjusted by age, sex, RV loads and viral and bacterial co-infections, were associated with clinical outcomes defined as need for supplemental oxygen, PICU admission and longer length of stay, Table 3. Mortality was not included as an outcome due to the small sample size.
Table 3: Adjusted risk factors associated with RV disease severity.
Of all comorbidities, asthma/atopy, prematurity and CHD were associated with increased odds of supplemental oxygen, PICU care and longer hospital stay. Chronic respiratory diseases were also independently associated with increase odds of oxygen supplementation and prolonged length of stay. Bacterial co-infections increased the risk of all three clinical outcomes, while older age and higher RV loads (<25 Ct values) were associated with increased odds of PICU care.
Discussion
In this study including ~2,000 children and adolescents with RV ARI, we found that the majority had a chronic medical condition, and that the healthcare utilization, morbidity and even mortality was high and differed according to the type of comorbidity. Importantly, bacterial co-infections, older age and higher RV loads were also related to increased disease severity. To our knowledge this is the largest study conducted to date that analyzed the differential impact of symptomatic RV infections in children with existing comorbidities considering key factors that may have influenced clinical outcomes.
Studies have attributed lower rates of adverse outcomes among children with RV ARI which may be partially explained by the prolonged shedding of RV in the upper respiratory tract and the high rates of asymptomatic carriage [4,5]. In our study, we found a high prevalence of underlying comorbidities in children with RV ARI, with asthma/atopy and prematurity being the most common, which has been previously described [8,18–21]. We also found that the burden associated with RV ARI was high and that the need for hospitalization, supplemental oxygen, PICU admission or mechanical ventilation differed according to the type of underlying condition [8,19,22–27]. While ICH had the lowest rate of healthcare utilization, asthma/atopy, prematurity and CHD were consistently and independently associated with worse disease severity [8,11,18]. The lower rate of healthcare utilization in ICH was surprising and results should be viewed cautiously due to the limited number of ICH children included in the study. Nonetheless, differences in results between studies might be explained in part to the patients analyzed, as we only included children with symptomatic RV ARI [28–31]. Semiquantitative viral loads (C_T_ values) were available for all children, and median RV loads were overall intermediate-high suggesting the potential contribution of RV to the clinical phenotype. Older age was also associated with worse clinical outcomes, which contrasts with other respiratory viruses such as RSV, which is typically linked to increased disease severity in young children [19,20,32,33].
Studies have reported rates of viral co-detection in children with RV ARI ranging from 15% to 50% depending on the study population and PCR platform used, a trend that has persisted post COVID-19 [8,20,21,34,35]. We found that the rates of RV/viral co-detections were common and ranged from 20% to 30%. These proportions were consistent across the different types of underlying conditions except for ICH in whom RV/viral co-detections were rare. While these results are intriguing, they need to be interpreted with caution as the number of ICH children included in the study was small, and the median age of these children high, which may partially explain the lower rates of RV/viral co-detections identified in these children. As shown by others we also found that the most common co-detected viruses were ADV, RSV and PIV [18,20,34]. Interestingly, the type of RV/viral co-detection differed based on the underlying condition, with RV/ADV being more common in premature and children with asthma/atopy, and RV/RSV in children with CHD and chronic respiratory diseases.
Bacterial co-infections in children with RV ARI are not well described, likely due to the low prevalence of bacteremia in children with LRTI or that lower respiratory or pleural fluid samples are often unavailable, yet antibiotics are frequently used. Studies have reported antibiotic use in < 30% of children with RV ARI, which is slightly lower than the 40% found in our study. This likely related to the higher prevalence of children with comorbidities that required hospitalization including ICH, that may have biassed clinical decision making [27,36]. A case-control study of children with RV ARI found that bacterial co-infections were identified by sputum or throat cultures in ~ 70% of inpatients vs 1% of outpatients [21]. We identified bacterial co-infections in 2.9% of children, especially in ICH and those with chronic respiratory conditions. Our rates are similar to a study conducted in children requiring PICU care, that also defined bacterial co-infections according to lower respiratory tract or sterile site cultures [35]. In our study, 1.5% of children died, and all but two had chronic medical conditions, with 40% having a viral or bacterial co-infection. While bacterial co-infections were relatively infrequent in our cohort, our data suggest that coinfections may be associated with worse clinical outcomes and warrant the analysis of this parameter as possible contributor to RV disease severity in future studies.
This study has limitations. First, due to the retrospective study design, data collection was limited to information recorded in the EHR. However, to address missing or incomplete data, we analyzed objective outcomes, and two independent investigators manually reviewed and curated the data to ensure accuracy. The patient population represented a convenience sample, which may have introduced potential bias by over-representing the more severe forms of the disease. However, the study included children evaluated in the outpatient setting, and although viral testing was performed at the discretion of the attending physician, it aligned with hospital policy during the study period. The viral panel did not include viruses like endemic coronaviruses or bocaviruses, which may have played a role in disease presentation and outcomes. We, however, accounted for viral co-detections as well as RV loads in multivariable analyses and did not find a significant effect of these factors on clinical outcomes. RV typing was not performed, which limited our ability to assess the prevalence of RV-A, -B or -C infections in children with specific comorbidities and their contribution to clinical disease severity.
In summary, this study provides an in-depth characterization of the different comorbidities associated with severe RV infections in a large cohort of children and adolescents with RV ARI. It also highlights the potential role of RV loads, age or bacterial co-infections in RV-associated clinical outcomes. Defining the clinical phenotype of severe RV infections may help with resource allocation and patient management, with the ultimate goal of improving clinical outcomes.
Supporting information
S1 FilePLoS One_supplementary material_R2_F.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gern JE. The AB Cs of rhinoviruses, wheezing, and asthma. J Virol. 2010;84(15):7418–26. doi: 10.1128/JVI.02290-09 20375160 PMC 2897627 · doi ↗ · pubmed ↗
- 2Martin EK, Kuypers J, Chu HY, Lacombe K, Qin X, Strelitz B, et al. Molecular epidemiology of human rhinovirus infections in the pediatric emergency department. J Clin Virol. 2015;62:25–31. doi: 10.1016/j.jcv.2014.11.006 25542466 PMC 4403738 · doi ↗ · pubmed ↗
- 3Drysdale SB, Mejias A, Ramilo O. Rhinovirus - not just the common cold. J Infect. 2017;74 Suppl 1:S 41–6. doi: 10.1016/S 0163-4453(17)30190-1 28646961 · doi ↗ · pubmed ↗
- 4Byington CL, Ampofo K, Stockmann C, Adler FR, Herbener A, Miller T, et al. Community surveillance of respiratory viruses among families in the utah better identification of germs-longitudinal viral epidemiology (BIG-Lo VE) study. Clin Infect Dis. 2015;61(8):1217–24. doi: 10.1093/cid/civ 486 26245665 PMC 4583580 · doi ↗ · pubmed ↗
- 5Singleton RJ, Bulkow LR, Miernyk K, De Byle C, Pruitt L, Hummel KB, et al. Viral respiratory infections in hospitalized and community control children in Alaska. J Med Virol. 2010;82(7):1282–90. doi: 10.1002/jmv.21790 20513097 PMC 7167028 · doi ↗ · pubmed ↗
- 6Sundell N, Andersson L-M, Brittain-Long R, Sundvall P-D, AlsiöÅ, Lindh M, et al. PCR detection of respiratory pathogens in asymptomatic and symptomatic adults. J Clin Microbiol. 2019;57(1):e 00716-18. doi: 10.1128/JCM.00716-18 30355759 PMC 6322459 · doi ↗ · pubmed ↗
- 7Jackson DJ, Gern JE. Rhinovirus infections and their roles in asthma: etiology and exacerbations. J Allergy Clin Immunol Pract. 2022;10(3):673–81. doi: 10.1016/j.jaip.2022.01.006 35074599 PMC 10314805 · doi ↗ · pubmed ↗
- 8Costa LF, Queiróz DAO, Lopes da Silveira H, Bernardino Neto M, de Paula NT, Oliveira TFMS, et al. Human rhinovirus and disease severity in children. Pediatrics. 2014;133(2):e 312-21. doi: 10.1542/peds.2013-2216 24420808 · doi ↗ · pubmed ↗